TABLE of CONTENTS Chapter 5: Enhancing RQHR’S Capacity
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Preliminary Demographic Analysis of First Nations and Métis People
○○○○○○○○○○○○○○○○○○○○○○○○○○○○○○○○○○○○○○○○○○○○○○○○○○○○○○○○○○○○○○○○ APPENDIX F Preliminary Demographic Analysis of First Nations and Métis People A Background Paper Prepared for the Regina QuAppelle Health Region Working Together Towards Excellence Project September 2002 1. Introduction ........................................................................ 2 By Project Staff Team: Rick Kotowich 2. Findings Joyce Racette ........................................................................ 3 Dale Young The Size of the First Nations and Métis Alex Keewatin Populations ..................................................... 3 John Hylton The Characteristics of These Populations....... 6 The Trends ...................................................... 8 3. Conclusion ........................................................................ 9 Appendix F 1 ○○○○○○○○○○○○○○○○○○○○○○○○○○○○○○○○○○○○○○○○○○○○○○○○○○○○○○○○○○○○○○○○ 1. Introduction 2. It has been well documented that even in the CMAs where census data is available, it often significantly underestimates the true size of the Aboriginal Regina Qu’Appelle Health Region population. This occurs for many reasons, including the fact that Aboriginal people tend to fill out fewer The purpose of this brief paper is to provide a census forms. Moreover, conventional methods for preliminary analysis of available population and estimating the gap in reporting do not always take demographic data for the First Nations and Métis account of the larger size of Aboriginal people who live within the geographic -
Diabetes Directory
Saskatchewan Diabetes Directory February 2015 A Directory of Diabetes Services and Contacts in Saskatchewan This Directory will help health care providers and the general public find diabetes contacts in each health region as well as in First Nations communities. The information in the Directory will be of value to new or long-term Saskatchewan residents who need to find out about diabetes services and resources, or health care providers looking for contact information for a client or for themselves. If you find information in the directory that needs to be corrected or edited, contact: Primary Health Services Branch Phone: (306) 787-0889 Fax : (306) 787-0890 E-mail: [email protected] Acknowledgement The Saskatchewan Ministry of Health acknowledges the efforts/work/contribution of the Saskatoon Health Region staff in compiling the Saskatchewan Diabetes Directory. www.saskatchewan.ca/live/health-and-healthy-living/health-topics-awareness-and- prevention/diseases-and-disorders/diabetes Table of Contents TABLE OF CONTENTS ........................................................................... - 1 - SASKATCHEWAN HEALTH REGIONS MAP ............................................. - 3 - WHAT HEALTH REGION IS YOUR COMMUNITY IN? ................................................................................... - 3 - ATHABASCA HEALTH AUTHORITY ....................................................... - 4 - MAP ............................................................................................................................................... -
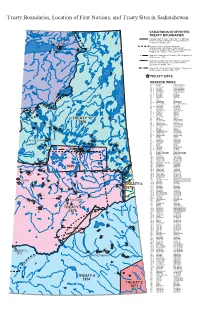
Treaty Boundaries Map for Saskatchewan
Treaty Boundaries, Location of First Nations, and Treaty Sites in Saskatchewan VARIATIONS IN DEPICTED TREATY BOUNDARIES Canada Indian Treaties. Wall map. The National Atlas of Canada, 5th Edition. Energy, Mines and 229 Fond du Lac Resources Canada, 1991. 227 General Location of Indian Reserves, 225 226 Saskatchewan. Wall Map. Prepared for the 233 228 Department of Indian and Northern Affairs by Prairie 231 224 Mapping Ltd., Regina. 1978, updated 1981. 232 Map of the Dominion of Canada, 1908. Department of the Interior, 1908. Map Shewing Mounted Police Stations...during the Year 1888 also Boundaries of Indian Treaties... Dominion of Canada, 1888. Map of Part of the North West Territory. Department of the Interior, 31st December, 1877. 220 TREATY SITES RESERVE INDEX NO. NAME FIRST NATION 20 Cumberland Cumberland House 20 A Pine Bluff Cumberland House 20 B Pine Bluff Cumberland House 20 C Muskeg River Cumberland House 20 D Budd's Point Cumberland House 192G 27 A Carrot River The Pas 28 A Shoal Lake Shoal Lake 29 Red Earth Red Earth 29 A Carrot River Red Earth 64 Cote Cote 65 The Key Key 66 Keeseekoose Keeseekoose 66 A Keeseekoose Keeseekoose 68 Pheasant Rump Pheasant Rump Nakota 69 Ocean Man Ocean Man 69 A-I Ocean Man Ocean Man 70 White Bear White Bear 71 Ochapowace Ochapowace 222 72 Kahkewistahaw Kahkewistahaw 73 Cowessess Cowessess 74 B Little Bone Sakimay 74 Sakimay Sakimay 74 A Shesheep Sakimay 221 193B 74 C Minoahchak Sakimay 200 75 Piapot Piapot TREATY 10 76 Assiniboine Carry the Kettle 78 Standing Buffalo Standing Buffalo 79 Pasqua -

Annual Report September 2019
ANNUAL REPORT SEPTEMBER 2019 File Hills Qu’Appelle Tribal Council HEALTH SERVICES FHQ Health Services is respected globally for exceeding quality in the delivery of safe health care services that embrace First Nations cultures and our traditions of wholistic physical, mental, emotional and spiritual wellbeing contributing to healthy individuals, families and communities. SEPTEMBER 2019 Table of Contents INTRODUCTION 3 MANAGEMENT, HEALTH PLANNING & ADMIINISTRATION 5 INFORMATION TECHNOLOGY 6 HEALTH EDUCATION 7 DIABETES EDUCATION 15 ENVIRONMENTAL HEALTH 16 HOME CARE 17 COMMUNITY HEALTH NURSING 18 COMPLEMENTARY SERVICES 19 FHQ HEALTH SERVICES An integrated approach to health care delivery. 2 File Hills Qu’Appelle Tribal Council Health Services File Hills Qu’Appelle (FHQ) Health Services is an entity of the FHQ Tribal Council in Fort Qu’Appelle, Saskatchewan and is part of Treaty 4 Territory. The program provides services to the member communities: Mission Statement FILE HILLS AGENCY QU’APPELLE AGENCY FHQ Health Services is a program of Carry the Kettle Nakoda Nation Muscowpetung Saulteaux First the FHQTC dedicated to the delivery Nation of safe, client centred wholistic care and supportive services for and with Little Black Bear’s Band of Cree Nekaneet First Nation our member First Nations that are & Assiniboine Nations Pasqua First Nation consistent with our values and meet Okanese First Nation the needs of our communities. Our Piapot First Nation services include: Peepeekisis Cree Nation • Health Promotion and Education Standing Buffalo Dakota Nation Chronic Disease and Injury Prevention Star Blanket Cree Nation Wood Mountain Lakota First • Healthy Children and Youth Nation • Environmental Health • Communicable Diseases FHQ Health Services embraces the values of Respect, • Home and Community Care Accountability, Cooperation and Integrity in respect to all aspects of health care. -

National Assessment of First Nations Water and Wastewater Systems
National Assessment of First Nations Water and Wastewater Systems Saskatchewan Regional Roll-Up Report FINAL Department of Indian Affairs and Northern Development January 2011 Neegan Burnside Ltd. 15 Townline Orangeville, Ontario L9W 3R4 1-800-595-9149 www.neeganburnside.com National Assessment of First Nations Water and Wastewater Systems Saskatchewan Regional Roll-Up Report Final Department of Indian and Northern Affairs Canada Prepared By: Neegan Burnside Ltd. 15 Townline Orangeville ON L9W 3R4 Prepared for: Department of Indian and Northern Affairs Canada January 2011 File No: FGY163080.4 The material in this report reflects best judgement in light of the information available at the time of preparation. Any use which a third party makes of this report, or any reliance on or decisions made based on it, are the responsibilities of such third parties. Neegan Burnside Ltd. accepts no responsibility for damages, if any, suffered by any third party as a result of decisions made or actions based on this report. Statement of Qualifications and Limitations for Regional Roll-Up Reports This regional roll-up report has been prepared by Neegan Burnside Ltd. and a team of sub- consultants (Consultant) for the benefit of Indian and Northern Affairs Canada (Client). Regional summary reports have been prepared for the 8 regions, to facilitate planning and budgeting on both a regional and national level to address water and wastewater system deficiencies and needs. The material contained in this Regional Roll-Up report is: preliminary in nature, to allow for high level budgetary and risk planning to be completed by the Client on a national level. -

Calling to Justice, 1St Annual Conference for Change
Calling to Justice, 1st Annual Conference for Change Presented by the Saskatchewan First Nations Women’s Commission MARCH 24-25-26, 2021 CALLING TO JUSTICE, 1ST ANNUAL CONFERENCE FOR CHANGE This March 24-26, the Saskatchewan First Nations Women’s Commission presents the first annual We Rise Conference, dedicated to advancing a regional action plan for change. In 2007, the United Nations Declaration on the Rights of Indigenous Peoples (UNDRIP) moved to enshrine the rights that “constitute the minimum standards for the survival, dignity and well-being of the indigenous peoples of the world.” In 2015, the Truth & Reconciliation Commission released 94 Calls to Action to redress the legacy of residential schools and advance reconciliation. Four years later, Reclaiming Power and Place: the Final Report of the National Inquiry into Missing and Murdered Indigenous Women and Girls called for transformative legal and social changes to resolve the crisis that has devastated Indigenous communities across the country. Many First Nations people in Saskatchewan have shared their insight and experiences to build a better world for future generations. This three-day conference acknowledges our part in advocating for change, and that of our allies, and reflects on what we’ve accomplished so far, helping us to move forward to the next steps, together. A Red Eagle Lodge event, all associated proceeds from We Rise will be directed toward front-line programs and services for First Nations women, the keepers of the home fire, and devote resources to strategic goals including the advancement of Women’s Rights and Sovereignty. ONLINE DELIVERY: Due to COVID-19 restrictions, We Rise will be delivered in an online format through Webinar Ninja. -

5 Traditional Land and Resource Use
CA PDF Page 1 of 92 Energy East Project Part B: Saskatchewan and Manitoba Volume 16: Socio-Economic Effects Assessment Section 5: Traditional Land and Resource Use This section was not updated in 2015, so it contains figures and text descriptions that refer to the October 2014 Project design. However, the analysis of effects is still valid. This TLRU assessment is supported by Volume 25, which contains information gathered through TLRU studies completed by participating Aboriginal groups, oral traditional evidence and TLRU-specific results of Energy East’s aboriginal engagement Program from April 19, 2014 to December 31, 2015. The list of First Nation and Métis communities and organizations engaged and reported on is undergoing constant revision throughout the discussions between Energy East and potentially affected Aboriginal groups. Information provided through these means relates to Project effects and cumulative effects on TLRU, and recommendations for mitigating effects, as identified by participating Aboriginal groups. Volume 25 for Prairies region provides important supporting information for this section; Volume 25 reviews additional TRLU information identifies proposed measures to mitigate potential effects of the Project on TRLU features, activities, or sites identified, as appropriate. The TLRU information provided in Volume 25 reflects Project design changes that occurred in 2015. 5 TRADITIONAL LAND AND RESOURCE USE Traditional land and resource use (TLRU)1 was selected as a valued component (VC) due to the potential for the Project to affect traditional activities, sites and resources identified by Aboriginal communities. Project Aboriginal engagement activities and the review of existing literature (see Appendix 5A.2) confirmed the potential for Project effects on TLRU. -

Ressources Naturelles Canada
111° 110° 109° 108° 107° 106° 105° 104° 103° 102° 101° 100° 99° 98° n Northwest Territories a i d n i a r i e Territoires du Nord-Ouest d M i n r a e h i Nunavut t M 60° d r 60° i u r d o e n F M o c e d S r 1 i 2 h 6 23 2 2 T 21 20 19 18 17 16 15 14 1 126 12 11 10 9 Sovereign 4 3 2 125 8 7 6 5 4 3 9 8 7 6 5 Thainka Lake 23 Lake 19 18 17 16 15 13 12 11 10 Tazin Lake Ena Lake Premier 125 124 125 Lake Selwyn Lake Ressources naturelles Sc ott Lake Dodge Lake 124 123 Tsalwor Lake Canada 124 Misaw Lake Oman Fontaine Grolier Bonokoski L. 123 1 Harper Lake Lake 22 Lake 123 Lake Herbert L. Young L. CANADA LANDS - SASKATCHEWAN TERRES DU CANADA – SASKATCHEWAN 122 Uranium City Astrolabe Lake FIRST NATION LANDS and TERRES DES PREMIÈRES NATIONS et 121 122 Bompas L. Beaverlodge Lake NATIONAL PARKS OF CANADA PARCS NATIONAUX DU CANADA 121 120 121 Fond du Lac 229 Thicke Lake Milton Lake Nunim Lake 120 Scale 1: 1 000 000 or one centimetre represents 10 kilometres Chipman L. Franklin Lake 119 120 Échelle de 1/1 000 000 – un centimètre représente 10 kilomètres Fond du Lac 227 119 0 12.5 25 50 75 100 125 150 1 Lake Athabasca 18 Fond-du-Lac ! 119 Chicken 225 Kohn Lake Fond du Lac km 8 Fond du Lac 228 Stony Rapids 11 117 ! Universal Transverse Mercator Projection (NAD 83), Zone 13 233 118 Chicken 226 Phelps Black Lake Lake Projection de Mercator transverse universelle (NAD 83), zone 13 Fond du Lac 231 117 116 Richards Lake 59° 59° 117 Chicken NOTE: Ath 224 This map is an index to First Nation Lands (Indian Lands as defined by the Indian Act) abasca Sand Dunes Fond du Lac 232 Provincial Wilderne Black Lake 116 1 ss Park and National Parks of Canada. -

Analysis Report
Analysis Report WHETHER TO DESIGNATE THE NINE AGRICULTURAL DRAINAGE NETWORK PROJECTS IN SASKATCHEWAN December 2019 TABLE OF CONTENTS PURPOSE ........................................................................................................................................................... 2 PROJECTS .......................................................................................................................................................... 2 CONTEXT OF REQUESTS ..................................................................................................................................... 2 PROJECT CONTEXT ............................................................................................................................................ 3 Project Overview ........................................................................................................................................... 3 Project Components and Activities ............................................................................................................... 5 Blackbird Creek Drainage Network (Red/Assiniboine River watershed) ........................................................... 5 Saline Lake Drainage Network (Upper Assiniboine River watershed) ............................................................... 6 600 Creek Drainage Network (Lower Souris River watershed) ......................................................................... 6 Vipond Drainage Network (Moose Mountain Lake and Lower Souris River watersheds) -

Federation of Saskatchewan Indian Nations Year End Report 2012-2013
Federation of Saskatchewan Indian Nations Year End Report 2012-2013 APM-REP-00621-0004 June 11, 2013 Federation of Saskatchewan Indian Nations NWMO-TMP-AD-0007 R001 Year-End Report 2012-2013 Information Sessions regarding NWMO Prepared by: Lands and Resources Secretariat Federation of Saskatchewan Indian Nations -Submitted to- Nuclear Waste Management Organization Date Submitted: June 11, 2013 Staffing Report: The following is the list of the FSIN Lands and Resources staff positions and contractors under the Executive Director for the fiscal year 2012/2013: A. Marlene Lumberjack, FSIN-NWMO Technician / Interim Executive Director B. Chris Morin, Interim Executive Director C. Brian Scribe, FSIN-NWMO Technician D. Josephine Williams, Administrative Assistant E. Milton Gamble, Consultant F. Barbara Lavallee, Consultant Financial Update: Confirmed: NWMO - $577,544.00 (Salaries, travel, 10% FSIN fee, office operations, information sessions, Lands and Resources Commission, and FSIN discretionary). The FSIN annual audited report will be provided to you by July 31, 2013. 1 Introduction The Federation of Saskatchewan Indian Nations (FSIN) Lands and Resources Secretariat (LRS) has recently expended the third year of funds available under the Contribution Agreement between the Nuclear Waste Management Organization (NWMO), and is pleased to provide the NWMO with the 2012-2013 FSIN-NWMO Contribution Agreement Year-End Report. The term of the Agreement was for October 1, 2010 to March 31, 2013 with potential extension of long-term funding pending activity in Saskatchewan. The purpose of the Agreement was, and continues to be, to build internal capacity within the FSIN that will provide education and awareness to all First Nations and Tribal/Agency/Grand Councils in Saskatchewan involved in the NWMO’s site selection process for Adaptive Phased Management and general information to all First Nations in Saskatchewan. -
BATC CDC Annual Report 2008-2009
Committed to providing fair, equitable and non-biased community support Table of Contents BATC CDC Strategic Plan Page 3—4 Background Page 5 Message from the Chairman Page 6 Members of the Board Page 7 Staff Page 8 Grant Distribution Summary Page 9-15 Testimonials Page 15—18 Photo Collection Page 19—22 Auditor’s Report Page 23—28 Management Discussion and Analysis Page 29 2 BATC CDC Strategic Plan The Battleford Agency Tribal Chief’s Strategic Planning sessions were held in North Battleford commencing October 15, 2008 with final draft approved on August 11, 2009. Rationale Section 7.10.1 of the amended Gaming Agreement: The CDC shall provide as part of its annual report a statement of goals, objectives, and performance meas- ures – each year will be measured by how well you have performed in pursuit of your goals and objectives. Core Values The Core Values of the BATC CDC are as follows: Good governance practice Communication Improve quality of life Respect for culture Sharing Vision The BATC CDC’s vision is to create healthier, self-sufficient, and more vibrant communities by supporting projects. Mission BATC CDC facilitates distribution of a portion of casino proceeds to make measurable and lasting im- provements to the quality of life. 3 BATC CDC Strategic Plan—continued Goals and Objectives CORE VALUE OBJECTIVE GOAL TIMELINE MEASUREMENT Good Governance Practice Having good policies Review once yearly May 31/09 Resolution receiving report and Effective management team Evaluation Mar 31/10 update as necessary Having effective Board Audit Mar 31/10 Management regular reporting to Accountability/Transparency Board Compliant with Gaming Agreement Communication Create public awareness of CDC Have information booth at May/09 – July/ 09 Reporting Treaty Days in catchment area Public Information Sessions 4 – 5 /year Newspaper Supplement Promote and publicize programs Improve Quality of Life Provide economic development Mailouts re: promotion and Reporting on each of opportunities for communities update projects…completion, etc. -

Saskatchewan Official Road
PRINCE ALBERT MELFORT MEADOW LAKE Population MEADOW LAKE PROVINCIAL PARK Population 35,926 Population 40 km 5,992 5,344 Prince Albert Visitor Information Centre Visitor Information 4 3700 - 2nd Avenue West Prince Albert National Park / Waskesieu Nipawin 142 km Northern Lights Palace Meadow Lake Tourist Information Centre Phone: 306-682-0094 La Ronge 88 km Choiceland and Hanson Lake Road Open seasonally 110 Mcleod Avenue W 79 km Hwy 4 and 9th Ave W GREEN LAKE 239 km 55 Phone: 306-752-7200 Phone: 306-236-4447 ve E 49 km Flin Flon t A Chamber of Commerce 6 RCMP 1s 425 km Open year-round 2nd Ave W 3700 - 2nd Avenue West t r S P.O. Phone: 306-764-6222 3 e iv M e R 5th Ave W r e Prince Albert . t Open year-round e l e n c f E v o W ru e t p 95 km r A 7th Ave W t S C S t y S d Airport 3 Km 9th Ave W H a 5 r w 3 Little Red 55 d ? R North Battleford T River Park a Meadow Lake C CANAM o Radio Stations: r HIGHWAY Lions Regional Park 208 km 15th St. N.W. 15th St. N.E. Veteran’s Way B McDonald Ave. C CJNS-Q98-FM e RCMP v 3 Mall r 55 . A e 3 e Meadow Lake h h v RCMP ek t St. t 5 km Northern 5 A Golf Club 8 AN P W Lights H ark . E Airport e e H Ave.