WHO-HAC May 05.Pub
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Mapping a Healthier Future
Health Planning Department, Ministry of Health, Uganda Directorate of Water Development, Ministry of Water and Environment, Uganda Uganda Bureau of Statistics International Livestock Research Institute World Resources Institute The Republic of Uganda Health Planning Department MINISTRY OF HEALTH, UGANDA Directorate of Water Development MINISTRY OF WATER AND ENVIRONMENT, UGANDA Uganda Bureau of Statistics Mapping a Healthier Future ISBN: 978-1-56973-728-6 How Spatial Analysis Can Guide Pro-Poor Water and Sanitation Planning in Uganda HEALTH PLANNING DEPARTMENT MINISTRY OF HEALTH, UGANDA Plot 6 Lourdel Road P.O. Box 7272 AUTHORS AND CONTRIBUTORS Kampala, Uganda http://www.health.go.ug/ This publication was prepared by a core team from fi ve institutions: The Health Planning Department at the Ministry of Health (MoH) leads eff orts to provide strategic support Health Planning Department, Ministry of Health, Uganda to the Health Sector in achieving sector goals and objectives. Specifi cally, the Planning Department guides Paul Luyima sector planning; appraises and monitors programmes and projects; formulates, appraises and monitors Edward Mukooyo national policies and plans; and appraises regional and international policies and plans to advise the sector Didacus Namanya Bambaiha accordingly. Francis Runumi Mwesigye Directorate of Water Development, Ministry of Water and Environment, Uganda DIRECTORATE OF WATER DEVELOPMENT Richard Cong MINISTRY OF WATER AND ENVIRONMENT, UGANDA Plot 21/28 Port Bell Road, Luzira Clara Rudholm P.O. Box 20026 Disan Ssozi Kampala, Uganda Wycliff e Tumwebaze http://www.mwe.go.ug/MoWE/13/Overview Uganda Bureau of Statistics The Directorate of Water Development (DWD) is the lead government agency for the water and sanitation Thomas Emwanu sector under the Ministry of Water and Environment (MWE) with the mandate to promote and ensure the rational and sustainable utilization, development and safeguard of water resources for social and economic Bernard Justus Muhwezi development, as well as for regional and international peace. -

Erin's Guide to Gulu
Edited 10/2019 GHCE Global Health Clinical Elective 2020 GUIDE TO YOUR CLINICAL ELECTIVE IN Gulu, UGANDA Disclaimer: This booklet is provided as a service to UW students going to Gulu, Uganda, based on feedback from previous students. The Global Health Resource Center is not responsible for any inaccuracies or errors in the booklet's contents. Students should use their own common sense and good judgment when traveling, and obtain information from a variety of reliable sources. Please conduct your own research to ensure a safe and satisfactory experience. TABLE OF CONTENTS Contact Information 3 Entry Requirements 5 Country Overview 6 Packing Tips 8 Money 13 Communication 13 Travel to/from Gulu 14 Phrases 16 Food 16 Budgeting 17 Fun 17 Health and Safety Considerations 18 How not to make an ass of yourself 19 Map 21 Cultural Adjustment 24 Guidelines for the Management of Body Fluid Exposure 26 2 CONTACT INFORMATION - U.S. Name Address Telephone Email or Website UW In case of emergency: +1-206-632-0153 www.washington.edu/glob International 1. Notify someone in country (24-hr hotline) alaffairs/emergency/ Emergency # 2. Notify CISI (see below) 3. Call 24-hr hotline [email protected] 4. May call Scott/McKenna [email protected] GHCE Director(s) Dr. Scott +206-473-0392 [email protected] McClelland (Scott, cell) [email protected] 001-254-731- Dr. McKenna 490115 (Scott, Eastment Kenya) GHRC Director Daren Wade Harris Hydraulics +1-206-685-7418 [email protected] (office) Building, Room [email protected] #315 +1-206-685-8519 [email protected] 1510 San Juan (fax) Road Seattle, WA 98195 Insurance CISI 24/7 call center [email protected] available at 888-331- nce.com 8310 (toll-free) or 240-330-1414 (accepts Collect calls) Hall Health Anne Terry, 315 E. -

Uganda Humanitarian Update
UGANDA HUMANITARIAN UPDATE MAY – JUNE 2010 I. HIGHLIGHTS AMID HEAVY RAINS, HUMANITARIAN ACCESS IN PARTS OF KARAMOJA AND TESO HAMPERED BY DETERIORATING ROAD CONDITIONS OVER 1,000 CHOLERA CASES REGISTERED IN KARAMOJA SINCE APRIL 2010 90% OF IDPS IN NORTHERN UGANDA NO LONGER LIVING IN CAMPS, BUT LAND CONFLICTS AND LANDMINES IMPEDING RETURN IN SOME AREAS II. SECURITY AND ACCESS SECURITY The general situation in Karamoja remained fragile, according to the United Nations Department for Safety and Security (UNDSS). Cattle raids, including on protected kraals, particularly affected Moroto and Kotido, with some resulting in fierce clashes between the Uganda People’s Defence Forces and the raiders. In South Karamoja incidents associated with food distributions involved theft of food and non-food items (NFIs), and attacks on food distributors as well as on food recipients. Following three road ambushes in Alerek sub-county of Abim District during the month, UNDSS issued an advisory limiting UN movement along the Abim-Kotido road to between 09.00Hrs and 16.00Hrs with effect from 28 June 2010. Three civilians were killed in one of those ambushes. In northern Uganda, Amuru District officials and partners carried out a joint assessment in the wake of a violent land dispute that occurred in Koli village of Pabbo sub-county on 23 June. Preliminary findings indicated that one person was killed and several others injured in the dispute involving two clans. Some 40 huts were torched and many members of either clan had fled the village. Also of concern in the region during the reporting period were raids by illegally armed Karamojong, particularly in Pader District. -

Country Operations Plan
COUNTRY OPERATIONS PLAN Country: Uganda Planning Year: 2004 2004 Country Operations Plan – Uganda __________________________________________________________________________________________ Part I: Executive - Summary 1.1 Context and Beneficiary Populations UNHCR’s presence in Uganda dates back from the 1960s. Though the earlier arrivals of Rwandan refugees had returned in 1994, the country still hosts 18,500 Rwandans who are residual caseloads of the 1996 repatriation from Tanzania. There are some 5,000 Rwandans who entered Mbarara district of Uganda from Tanzania when the Rwandan refugees were being repatriated from there in 2002. The Government of Uganda has not yet decided their status. The majority of the refugees in the country today are Southern Sudanese hosted in northern Uganda and who number about 172,300 (86%) of the total refugee population of 200,800 as of 28 February 2003. About 8,500 Congolese refugees hosted in the Southwest are from the Democratic Republic of Congo (DRC). There are other smaller groups from Somalia, Ethiopia and Kenya that are also being assisted. Sudanese and Congolese refugees are granted status on a prima facie basis, while the status of others is ascertained through individual refugee status determination. Almost all the refugees fled their respective countries of origin because of the civil war and fear of persecution caused by ethnic rivalries and political differences. The Government of Uganda, continues to host refugees from the neighbouring countries. Refugees who are in designated settlememnts are provided with agricultural lands, tools and seeds with the objective of making them self-sufficient. As a result, refugees in the northern settlements have managed to produce a certain percentage of their food requirements, thereby reducing dependence on the food assistance from WFP. -

Ministry of Health
UGANDA PROTECTORATE Annual Report of the MINISTRY OF HEALTH For the Year from 1st July, 1960 to 30th June, 1961 Published by Command of His Excellency the Governor CONTENTS Page I. ... ... General ... Review ... 1 Staff ... ... ... ... ... 3 ... ... Visitors ... ... ... 4 ... ... Finance ... ... ... 4 II. Vital ... ... Statistics ... ... 5 III. Public Health— A. General ... ... ... ... 7 B. Food and nutrition ... ... ... 7 C. Communicable diseases ... ... ... 8 (1) Arthropod-borne diseases ... ... 8 (2) Helminthic diseases ... ... ... 10 (3) Direct infections ... ... ... 11 D. Health education ... ... ... 16 E. ... Maternal and child welfare ... 17 F. School hygiene ... ... ... ... 18 G. Environmental hygiene ... ... ... 18 H. Health and welfare of employed persons ... 21 I. International and port hygiene ... ... 21 J. Health of prisoners ... ... ... 22 K. African local governments and municipalities 23 L. Relations with the Buganda Government ... 23 M. Statutory boards and committees ... ... 23 N. Registration of professional persons ... 24 IV. Curative Services— A. Hospitals ... ... ... ... 24 B. Rural medical and health services ... ... 31 C. Ambulances and transport ... ... 33 á UGANDA PROTECTORATE MINISTRY OF HEALTH Annual Report For the year from 1st July, 1960 to 30th June, 1961 I.—GENERAL REVIEW The last report for the Ministry of Health was for an 18-month period. This report, for the first time, coincides with the Government financial year. 2. From the financial point of view the year has again been one of considerable difficulty since, as a result of the Economy Commission Report, it was necessary to restrict the money available for recurrent expenditure to the same level as the previous year. Although an additional sum was available to cover normal increases in salaries, the general effect was that many economies had to in all be made grades of staff; some important vacancies could not be filled, and expansion was out of the question. -

Free Mover Clinical Clerkships
FREE MOVER CLINICAL CLERKSHIPS Students interested in spending a clerkship activity abroad without participating in the Erasmus+ programs can enroll as Free-Movers (Fee-paying Visiting Students or Independent Students or Contract Students) at some foreign University hospitals where they can attend clinical rotations. The Free-Mover Clinical Clerkship Period is an optional part of the medical course and as such must be accounted for. Students not willing to participate still have to attend clinical rotations at the University of Milan. The Clerkship abroad represents a mutual contract between Supervisor and Student and is subject to supervision by the Faculty. In this document, there is the list of possible destinations and university hospitals in which the clinical clerkship period can be performed. For some of the destinations, students are advised to clearly declare their student status, as they may be allowed to participate only as observers and not and interns. 1 AFRICA Egypt Ethiopia Benin Botswana IvoryCoast Ghana Cameroon Kenya Libya Morocco Namibia Nigeria Rwanda Zambia Senegal Sudan SouthAfrica Tanzania Tunisia Uganda Zimbabwe ASIA China India Indonesia Japan Cambodia Malaysia Mongolia Nepal Philippines Singapore SriLanka SouthKorea Taiwan Thailand Vietnam 2 THE MIDDLE EAST Bahrain Iran Israel Jordan Qatar Lebanon Oman Palestine SaudiArabia Syria United Arab Emirates OCEANIA Australia Adelaide Canberra Melbourne Newcastle NewSouthWales Perth Queensland Sydney Tasmania New Zealand EUROPE Belgium Bosnia-Herzigowina Bulgaria Denmark -

WHO UGANDA BULLETIN February 2016 Ehealth MONTHLY BULLETIN
WHO UGANDA BULLETIN February 2016 eHEALTH MONTHLY BULLETIN Welcome to this 1st issue of the eHealth Bulletin, a production 2015 of the WHO Country Office. Disease October November December This monthly bulletin is intended to bridge the gap between the Cholera existing weekly and quarterly bulletins; focus on a one or two disease/event that featured prominently in a given month; pro- Typhoid fever mote data utilization and information sharing. Malaria This issue focuses on cholera, typhoid and malaria during the Source: Health Facility Outpatient Monthly Reports, Month of December 2015. Completeness of monthly reporting DHIS2, MoH for December 2015 was above 90% across all the four regions. Typhoid fever Distribution of Typhoid Fever During the month of December 2015, typhoid cases were reported by nearly all districts. Central region reported the highest number, with Kampala, Wakiso, Mubende and Luweero contributing to the bulk of these numbers. In the north, high numbers were reported by Gulu, Arua and Koti- do. Cholera Outbreaks of cholera were also reported by several districts, across the country. 1 Visit our website www.whouganda.org and follow us on World Health Organization, Uganda @WHOUganda WHO UGANDA eHEALTH BULLETIN February 2016 Typhoid District Cholera Kisoro District 12 Fever Kitgum District 4 169 Abim District 43 Koboko District 26 Adjumani District 5 Kole District Agago District 26 85 Kotido District 347 Alebtong District 1 Kumi District 6 502 Amolatar District 58 Kween District 45 Amudat District 11 Kyankwanzi District -

Using Life Histories to Explore Gendered Experiences of Conflict in Gulu District, Northern Uganda: Implications for Post-Conflict Health Reconstruction
South African Review of Sociology ISSN: 2152-8586 (Print) 2072-1978 (Online) Journal homepage: http://www.tandfonline.com/loi/rssr20 Using life histories to explore gendered experiences of conflict in Gulu District, northern Uganda: Implications for post-conflict health reconstruction Sarah N. Ssali & Sally Theobald To cite this article: Sarah N. Ssali & Sally Theobald (2016) Using life histories to explore gendered experiences of conflict in Gulu District, northern Uganda: Implications for post- conflict health reconstruction, South African Review of Sociology, 47:1, 81-98, DOI: 10.1080/21528586.2015.1132634 To link to this article: https://doi.org/10.1080/21528586.2015.1132634 © 2016 The Author(s). Published by Unisa Published online: 24 Mar 2016. Press and Informa UK Limited, trading as Taylor & Francis Group Submit your article to this journal Article views: 145 View related articles View Crossmark data Citing articles: 8 View citing articles Full Terms & Conditions of access and use can be found at http://www.tandfonline.com/action/journalInformation?journalCode=rssr20 USING LIFE HISTORIES TO EXPLORE GENDERED EXPERIENCES OF CONFLICT IN GULU DISTRICT, NORTHERN UGANDA: IMPLICATIONS FOR POST-CONFLICT HEALTH RECONSTRUCTION Sarah N. Ssali School of Women and Gender Studies Makerere University [email protected]; [email protected] Sally Theobald Department of International Public Health Liverpool School of Tropical Medicine [email protected] ABSTRACT The dearth of knowledge about what life was like for different women and men, communities and institutions during conflict has caused many post-conflict developers to undertake reconstruction using standardised models that may not always reflect the realities of the affected populations. -
Arcview Print
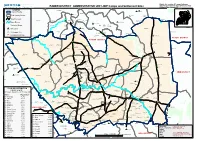
District, Sub counties, IDP camps, Settlement Sites,Transport Network, Rivers & Protected Areas PADER DISTRICT ADMINISTRATIVE UNIT- IDP Camps and Settlement Sites Reference Date: January 2007 Ayuu Anak Labworoye à LEGENDà à LAYAMO Nam Okora $Z Moyo Koboko Kaabong District Border Yumbe Kitgum Maracha Paibony Adjumani Kotido AMIDA Arua PADER Gulu Abim Amuru Layamo Moroto $Z Nebbi à Oyam Lira Sub County Border Amuria Lapana Buliisa Guda Masindi Apac Dokolo à Kaberamaido Katakwi Nakapiripirit Amolatar à Soroti Kumi Hoima Kapchorwa Nakasonola Bukedea Pallisa Bukwa Nakaseke Kamuli BudakaSironko Kaliro Bududa Bundibugyo Kiboga Kibaale Kayunga ButaleMjabale Namutumba Manafwa Luwero Road Network OROM Kyenjojo Iganga Tororo Kabarole Mubende Jinja Busia Lukwor Bugiri Mityana Mayuge Pawena KITGUM TC Kamwenge Kampala Lumule Kasese Panykel Akwan$Zg à NAMOKORA Sembabule Mpigi Wakiso à Ibanda Mukono à à Lyantonde Bushenyi Kiruhura Major Rivers $ZOmiya-Anyima Masaka Mbarara Kalangala Rukungiri Rakai Kitgum Matidi Kanungu Isingiro Opette $Z Ntungamo Amid$Za à KisoKraobale Protected Areas Lamit tum Lamola àAlel Pàawidi à à à Teso Bar Aparo Hil $Z IDP Camp $ZOryang à PAIMOL Okidài KACHERI à Settlement Site Lagoro àDure Akuna Làab $Z OMIYA- ANYIMA AKWANG Degazzetted Camp Lakwor $ZOmia-Pacha c PALABEK GEM à Laber Bàul KOTIDO DISTRICT KITGUM DISTRICT $ZAcholibur $ZWol $ZPaimol Mutu LAGUTI àLajeng $ZLatanya àLamin Nyi àOkinga ALEREK PALARO ACHOLIBUR Toromàa WOL Lagu$Zti Amilobo Bur Lobo à $ZPorogali Kokil à Ku Ywee à àOtok P/S Amoko à AWACH Awal à à àApil $ZKalongo -

Psychiatric Hospitals in Uganda
Psychiatric hospitals in Uganda A human rights investigation w www.mdac.org mentaldisabilityadvocacy @MDACintl Psychiatric hospitals in Uganda A human rights investigation 2014 December 2014 ISBN 978-615-80107-7-1 Copyright statement: Mental Disability Advocacy Center (MDAC) and Mental Health Uganda (MHU), 2014. All rights reserved. Contents Foreword ...................................................................................................................................................................................................... 4 Executive summary ......................................................................................................................................................................................................... 6 1. Introduction, torture standards and hospitals visited.............................................................................................................................. 9 1(A). The need for human rights monitoring........................................................................................................................................................... 9 1(B). Uganda country profile .................................................................................................................................................................................... 10 1(C). Mental health ................................................................................................................................................................................................... -
Assessment of the Capacity of Ugandan Health Facilities, Personnel, and Resources to Prevent and Control Noncommunicable Diseases
Yale University EliScholar – A Digital Platform for Scholarly Publishing at Yale Public Health Theses School of Public Health January 2014 Assessment Of The aC pacity Of Ugandan Health Facilities, Personnel, And Resources To Prevent And Control Noncommunicable Diseases Hilary Eileen Rogers Yale University, [email protected] Follow this and additional works at: http://elischolar.library.yale.edu/ysphtdl Recommended Citation Rogers, Hilary Eileen, "Assessment Of The aC pacity Of Ugandan Health Facilities, Personnel, And Resources To Prevent And Control Noncommunicable Diseases" (2014). Public Health Theses. 1246. http://elischolar.library.yale.edu/ysphtdl/1246 This Open Access Thesis is brought to you for free and open access by the School of Public Health at EliScholar – A Digital Platform for Scholarly Publishing at Yale. It has been accepted for inclusion in Public Health Theses by an authorized administrator of EliScholar – A Digital Platform for Scholarly Publishing at Yale. For more information, please contact [email protected]. ASSESSMENT OF THE CAPACITY OF UGANDAN HEALTH FACILITIES, PERSONNEL, AND RESOURCES TO PREVENT AND CONTROL NONCOMMUNICABLE DISEASES By Hilary Rogers A Thesis Presented to the Faculty of the Yale School of Public Health in Partial Fulfillment of the Requirements for the Degree of Masters of Public Health in the Department of Chronic Disease Epidemiology New Haven, Connecticut April 2014 Readers: Dr. Adrienne Ettinger, Yale School of Public Health Dr. Jeremy Schwartz, Yale School of Medicine ABSTRACT Due to the rapid rise of noncommunicable diseases (NCDs), the Uganda Ministry of Health (MoH) has prioritized NCD prevention, early diagnosis, and management. In partnership with the World Diabetic Foundation, MoH has embarked on a countrywide program to build capacity of the health facilities to address NCDs. -
Planned Shutdown Web October 2020.Indd
PLANNED SHUTDOWN FOR SEPTEMBER 2020 SYSTEM IMPROVEMENT AND ROUTINE MAINTENANCE REGION DAY DATE SUBSTATION FEEDER/PLANT PLANNED WORK DISTRICT AREAS & CUSTOMERS TO BE AFFECTED Kampala West Saturday 3rd October 2020 Mutundwe Kampala South 1 33kV Replacement of rotten vertical section at SAFARI gardens Najja Najja Non and completion of flying angle at MUKUTANO mutundwe. North Eastern Saturday 3rd October 2020 Tororo Main Mbale 1 33kV Create Two Tee-offs at Namicero Village MBALE Bubulo T/C, Bududa Tc Bulukyeke, Naisu, Bukigayi, Kufu, Bugobero, Bupoto Namisindwa, Magale, Namutembi Kampala West Sunday 4th October 2020 Kampala North 132/33kV 32/40MVA TX2 Routine Maintenance of 132/33kV 32/40MVA TX 2 Wandegeya Hilton Hotel, Nsooda Atc Mast, Kawempe Hariss International, Kawempe Town, Spencon,Kyadondo, Tula Rd, Ngondwe Feeds, Jinja Kawempe, Maganjo, Kagoma, Kidokolo, Kawempe Mbogo, Kalerwe, Elisa Zone, Kanyanya, Bahai, Kitala Taso, Kilokole, Namere, Lusanjja, Kitezi, Katalemwa Estates, Komamboga, Mambule Rd, Bwaise Tc, Kazo, Nabweru Rd, Lugoba Kazinga, Mawanda Rd, East Nsooba, Kyebando, Tilupati Industrial Park, Mulago Hill, Turfnel Drive, Tagole Cresent, Kamwokya, Kubiri Gayaza Rd, Katanga, Wandegeya Byashara Street, Wandegaya Tc, Bombo Rd, Makerere University, Veterans Mkt, Mulago Hospital, Makerere Kavule, Makerere Kikumikikumi, Makerere Kikoni, Mulago, Nalweuba Zone Kampala East Sunday 4th October 2020 Jinja Industrial Walukuba 11kV Feeder Jinja Industrial 11kV feeders upgrade JINJA Walukuba Village Area, Masese, National Water Kampala East