Genetics of Endocrine Diseases in Miniature Schnauzer
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Miniature Schnauzer Secrets
Miniature Schnauzer Secrets Disclaimer The ebook is intended for information only. The publisher and author do not imply any results to those using this ebook, nor are they responsible for any results brought about by the usage of the information contained herein. The publisher and author disclaim any personal liability, loss, or risk incurred as a result of the use of any information or advice contained herein, either directly or indirectly. Furthermore, the publisher and author do not guarantee that the holder of this information will generate the same results as each Miniature Schnauzer dog is consider an individual that have many variables. This manual contains material protected under International and Federal Copyright Laws and Treaties. Any unauthorized reprint or use of this material is prohibited. This means any unauthorized use, sharing, reproduction or distribution of these materials by any means, electronic, mechanical, or otherwise is strictly prohibited. No portion of these materials may be reproduced in any manner whatsoever, without the express written consent of the publisher or author. Page 3 Miniature Schnauzer Secrets Table of Contents Introduction ................................................................................................. 7 Miniature Schnauzer Dogs At A Glance ....................................................... 8 What Is A Miniature Schnauzer?................................................................ 10 Miniature Schnauzers As Pets .................................................................. -

Giant Schnauzer)
FEDERATION CYNOLOGIQUE INTERNATIONALE (AISBL) SECRETARIAT GENERAL: 13, Place Albert 1 er B – 6530 Thuin (Belgique) ______________________________________________________________________________ 10.06.2021/ EN FCI-Standard N° 181 RIESENSCHNAUZER (Giant Schnauzer) 2 TRANSLATION : Mrs. C. Seidler. Official language (DE). ORIGIN : Germany. DATE OF PUBLICATION OF THE OFFICIAL VALID STANDARD : 25.05.2021. UTILIZATION : Utility and Companion Dog. FCI-CLASSIFICATION : Group 2 Pinscher and Schnauzer- Molossoid breeds - Swiss Mountain and Cattle Dogs. Section 1 Pinscher and Schnauzer type. With working trial. BRIEF HISTORICAL SUMMARY : Originally the Giant Schnauzer was used in the region of Southern Germany to drive cattle. Around the turn of the century, determined breeders realised that he had outstanding working capabilities and particularly valuable traits in character. Since 1913 the breed has been registered in a stud book, and in 1925 already the Giant Schnauzer has officially been recognised as a working dog. GENERAL APPEARANCE : Large, powerful, stocky rather than slim. An enlarged, powerful image of the Schnauzer. An imperturbable dog, prepared for defence, whose appearance fills with respect. IMPORTANT PROPORTIONS : • Square build in which height at the withers is nearly equal to the body length. FCI-St. N° 181 / 10.06.2021 3 • The length of the head (measured from the tip of the nose to the occiput) corresponds to half the length of the topline (measured from the withers to the set on of the tail). BEHAVIOUR / TEMPERAMENT : Typical characteristics of this dog are his good natured, even temperament and his incorruptible loyalty towards his master. He has highly developed sense organs, intelligence, trainability, strength, endurance, speed, resistance to weather and diseases. -

Miniature Schnauzer)
FEDERATION CYNOLOGIQUE INTERNATIONALE (AISBL) SECRETARIAT GENERAL: 13, Place Albert 1er B – 6530 Thuin (Belgique) ______________________________________________________________________________ _______________________________________________________________ 18.04.2007/EN _______________________________________________________________ FCI-Standard N° 183 ZWERGSCHNAUZER (Miniature Schnauzer) 2 TRANSLATION: Mrs C. Seidler. Official language (DE). COUNTRY OF ORIGIN: Germany. DATE OF PUBLICATION OF THE OFFICIAL VALID STANDARD: 06.03.07. UTILISATION: House and Companion Dog FCI-CLASSIFICATION: Group 2 Pinscher and Schnauzer- Molossoid breeds - Swiss Mountain and Cattle Dogs. Section 1 Pinscher and Schnauzer type. Without working trial. BRIEF HISTORICAL SUMMARY: Around the turn of the century a dwarf Schnauzer from the Frankfurt/Main area went on his way, then still described as a rough haired Zwergpinscher (Miniature Pinscher). Due to the different shapes, sizes and types and the muddle of harsh, soft and silky coat textures, it was no easy task to evolve a small dog with the appearance and the characteristic qualities of his bigger brother, the Schnauzer. GENERAL APPEARANCE: Small, strong, stocky rather than slim, rough coated, elegant. A reduced image of the Schnauzer without the drawback of a dwarfed appearance. IMPORTANT PROPORTIONS: • Square build in which the height at the withers is nearly equal to the body length. • The length of the head (measured from the tip of the nose to the occiput) corresponds to half the length of the topline (measured from the withers to the set on of the tail). FCI-St. N° 183 / 18.04.2007 3 BEHAVIOUR/TEMPERAMENT: His nature is similar to that of the Schnauzer and is determined by the temperament and the behaviour of a small dog. Intelligence, fearlessness, endurance, and alertness make the Miniature Schnauzer an agreeable house dog as well as a watch and companion dog which can be kept even in a small apartment without problems. -

Dane Line Reimagined
Dane Line Reimagined Published by the Great Dane Club of New England January 2021 Be Sure to Join Us for Our Up-Coming Shows: Supported Entry at the Chickadee Classic, Maine June 26-27, 2021 2021 Fall Specialties Thanksgiving Classic Springfield November 27-28 The shows will fall on Thanksgiving weekend President—Sue Davis Shaw Vice President—Marcia Roddy Recording Secretary—Kim Thurler Corresponding Secretary—Tiffany Cross Treasurer—Sharon Boldeia Directors—Suzanne Kelley, Normand Vadenais & Dianne Powers President’s Letter January 2021 Happy New Year everyone! I know it will be a better one for all of us. Welcome to the first issue of our ‘bigger and better’ bulletin thanks to the talented Carol Urick. Carol was the editor of Daneline for many years and evolved it into the wonderful publication that it was. We only ended it due to lack of funds in the club and the increasing cost of publication. Since I’ve been doing Throwback Thursday, I’ve heard from several people across the country who told me that they looked forward to getting it each year at the National. I hope everyone will get on board with getting your brags and litters listed. We are planning an every other month publication so the next deadline should be March 1st. I would like to welcome our new Associate Members, Michelle Hojdysz from New Rochelle, NY and Anne Sanders from Gardiner, NY. We hope to actually meet you in person when dog shows open up again. January is the month when we hold our annual meeting and election of officers. -

Investigation of an Inherited Cerebellar Malformation in the Eurasier Breed Dog
Investigation of an inherited cerebellar malformation in the Eurasier breed dog von Filipa de Faria Pedro Bernardino Inaugural-Dissertation zur Erlangung der Doktorwürde der Tierärztlichen Fakultät der Ludwig-Maximilians-Universität München Investigation of an inherited cerebellar malformation in the Eurasier breed dog von Filipa de Faria Pedro Bernardino aus Guimarães, Portugal München 2015 Aus dem Zentrum für Klinische Tiermedizin der Tierärztlichen Fakultät der Ludwig-Maximilians-Universität München Lehrstuhl: Innere Medizin der kleinen Haustiere und Heimtiere Arbeit angefertigt unter der Leitung von: apl. Prof. Andrea Fischer Gedruckt mit Genehmigung der Tierärztlichen Fakultät der Ludwig-Maximilians-Universität München Dekan: Univ.-Prof. Dr. Joachim Braun Berichterstatter: Prof. Dr. Andrea Fischer Korreferent: Univ.-Prof. Dr. Dr. Habil. Joris Peters Tag der Promotion: 18. Juli 2015 For my beloved family. “Learn from yesterday, live for today, hope for tomorrow. The important thing is to not stop questioning.” Albert Einstein Table of contents VI TABLE OF CONTENTS I. INTRODUCTION ...................................................................................... 7 II. REVIEW OF THE LITERATURE .......................................................... 9 1. THE HISTORY OF THE EURASIER BREED ..................................... 9 2. The caudal fossa: the cerebellum and the fourth ventricle…… ..........10 2.1. The development of the cerebellum ...........................................................10 2.2. The development of the -

Dog Breeds in Groups
Dog Facts: Dog Breeds & Groups Terrier Group Hound Group A breed is a relatively homogeneous group of animals People familiar with this Most hounds share within a species, developed and maintained by man. All Group invariably comment the common ancestral dogs, impure as well as pure-bred, and several wild cousins on the distinctive terrier trait of being used for such as wolves and foxes, are one family. Each breed was personality. These are feisty, en- hunting. Some use created by man, using selective breeding to get desired ergetic dogs whose sizes range acute scenting powers to follow qualities. The result is an almost unbelievable diversity of from fairly small, as in the Nor- a trail. Others demonstrate a phe- purebred dogs which will, when bred to others of their breed folk, Cairn or West Highland nomenal gift of stamina as they produce their own kind. Through the ages, man designed White Terrier, to the grand Aire- relentlessly run down quarry. dogs that could hunt, guard, or herd according to his needs. dale Terrier. Terriers typically Beyond this, however, generali- The following is the listing of the 7 American Kennel have little tolerance for other zations about hounds are hard Club Groups in which similar breeds are organized. There animals, including other dogs. to come by, since the Group en- are other dog registries, such as the United Kennel Club Their ancestors were bred to compasses quite a diverse lot. (known as the UKC) that lists these and many other breeds hunt and kill vermin. Many con- There are Pharaoh Hounds, Nor- of dogs not recognized by the AKC at present. -

Read Book Miniature Schnauzer Kindle
MINIATURE SCHNAUZER PDF, EPUB, EBOOK Judy Childerley | 148 pages | 31 Oct 2011 | First Stone Publishing | 9781906305512 | English | Lydney, United Kingdom Miniature Schnauzer PDF Book That combined with his stubbornness will keep you on your toes. Consider whether you have the time and patience for a dog who needs a lot of grooming, or the money to pay someone else to do it. This quickly helped set type and made them a distinct breed from the German Pinscher. Home All Breeds Breeds Quiz. Daily jaunts will also help prevent a pup from becoming overweight; this breed is known for its healthy appetite. If you are looking for puppies for sale or a particular stud dog in your area you can also check our puppies for sale and stud dog sections. Myotonia Congenita: Only recently discovered in Miniature Schnauzers, this is a hereditary skeletomuscular disorder similar to muscular dystrophy. Both charming and attractive, the Miniature Schnauzer is perky and devoted to his home and family. When picking a breed, consider your own activity level and lifestyle, and think about whether you'll find a frisky, energetic dog invigorating or annoying. Schnauzers have always been prized for their working ability. If you've got a laid-back attitude toward slobber, fine; but if you're a neatnik, you may want to choose a dog who rates low in the drool department. While small bladder stones may pass on their own, your vet should be consulted. Puppies ready for a new home in March. Height: 12 — 14 inches. George St. Common in most breeds during puppyhood and in Retriever breeds at all ages, mouthiness means a tendency to nip, chew, and play-bite a soft, fairly painless bite that doesn't puncture the skin. -
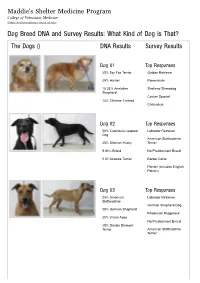
Dog Breed DNA and Survey Results: What Kind of Dog Is That? the Dogs () DNA Results Survey Results
Maddie's Shelter Medicine Program College of Veterinary Medicine (https://sheltermedicine.vetmed.ufl.edu) Dog Breed DNA and Survey Results: What Kind of Dog is That? The Dogs () DNA Results Survey Results Dog 01 Top Responses 25% Toy Fox Terrier Golden Retriever 25% Harrier Pomeranian 15.33% Anatolian Shetland Sheepdog Shepherd Cocker Spaniel 14% Chinese Crested Chihuahua Dog 02 Top Responses 50% Catahoula Leopard Labrador Retriever Dog American Staffordshire 25% Siberian Husky Terrier 9.94% Briard No Predominant Breed 5.07 Airedale Terrier Border Collie Pointer (includes English Pointer) Dog 03 Top Responses 25% American Labrador Retriever Staffordshire German Shepherd Dog 25% German Shepherd Rhodesian Ridgeback 25% Lhasa Apso No Predominant Breed 25% Dandie Dinmont Terrier American Staffordshire Terrier Dog 04 Top Responses 25% Border Collie Wheaten Terrier, Soft Coated 25% Tibetan Spaniel Bearded Collie 12.02% Catahoula Leopard Dog Briard 9.28% Shiba Inu Cairn Terrier Tibetan Terrier Dog 05 Top Responses 25% Miniature Pinscher Australian Cattle Dog 25% Great Pyrenees German Shorthaired Pointer 10.79% Afghan Hound Pointer (includes English 10.09% Nova Scotia Duck Pointer) Tolling Retriever Border Collie No Predominant Breed Dog 06 Top Responses 50% American Foxhound Beagle 50% Beagle Foxhound (including American, English, Treeing Walker Coonhound) Harrier Black and Tan Coonhound Pointer (includes English Pointer) Dog 07 Top Responses 25% Irish Water Spaniel Labrador Retriever 25% Siberian Husky American Staffordshire Terrier 25% Boston -
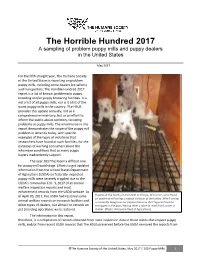
2017 Horrible Hundred Report
The Horrible Hundred 2017 A sampling of problem puppy mills and puppy dealers in the United States May 2017 For the fifth straight year, The Humane Society of the United States is reporting on problem puppy mills, including some dealers (re-sellers) and transporters. The Horrible Hundred 2017 report is a list of known, problematic puppy breeding and/or puppy brokering facilities. It is not a list of all puppy mills, nor is it a list of the worst puppy mills in the country. The HSUS provides this update annually, not as a comprehensive inventory, but as an effort to inform the public about common, recurring problems at puppy mills. The information in this report demonstrates the scope of the puppy mill problem in America today, with specific examples of the types of violations that researchers have found at such facilities, for the purposes of warning consumers about the inhumane conditions that so many puppy buyers inadvertently support. The year 2017 has been a difficult one for puppy mill watchdogs. Efforts to get updated information from the United States Department of Agriculture (USDA) on federally-inspected puppy mills were severely crippled due to the USDA’s removal on Feb. 3, 2017 of all animal welfare inspection reports and most enforcement records from the USDA website. As of April 20, 2017, the USDA had restored some Puppies at the facility of Alvin Nolt in Thorpe, Wisconsin, were found on unsafe wire flooring, a repeat violation at the facility. Wire flooring animal welfare records on research facilities and is especially dangerous for puppies because their legs can become other types of dealers, but almost no records on entrapped in the gaps, leaving them unable to reach food, water or pet breeding operations were restored. -

Is a Giant Schnauzer the Right Dog for You? by Daphne Cooke
Is a Giant Schnauzer the Right Dog for You? by Daphne Cooke Reprinted from What You Should Know About The Giant Schnauzer, 5th Edition ©1988 FREQUENTLY ASKED QUESTIONS ARE GIANT SCHNAUZERS GOOD WITH CHILDREN? This question should be reversed. Are your children good with dogs? No dog, Giant Schnauzer or otherwise, should be expected to put up with abusive treatment or teasing from children who have not been taught to treat animals with kindness. Even very young children can and must be taught respect for the family dog, or you can expect problems. All too often parents purchase a dog for the kids. They envision the kids taking care of the new puppy and everyone playing together happily. Puppies should never be bought for the children. At least one adult must accept the ultimate responsibility for the dog. One who really wants it and understands the care, training and love that the dog will need. Even a responsible teenager who asks for a dog should be reminded that teenagers usually leave home and leave their pets behind. Who will take care of the Giant Schnauzer then? ARE GIANT SCHNAUZERS ROAMERS? Any dog who is not on a leash or in a fenced yard is a potential roamer, and possible troublemaker. Giant Schnauzers should be fenced at home or reliably trained for voice control, and you should be on the end of the leash when not at home. It is your responsibility to keep the dog safe from unfamiliar dangers (cars, trucks, garbage, irate neighbors) and to clean up after it. -

Pinscher and Schnauzer - Molossoid Breeds
PDF 120TH PDF BREED SPECIALTY DOG SHOW December 04, 2016 PCCI ACTIVITY CENTER, MARIKINA CITY PINSCHER AND SCHNAUZER - MOLOSSOID BREEDS DOBERMANN JEDY DAVID KRIST CHUA (PHILIPPINES) ENTRY # NAME OF DOG, PCCISB No. AWARDS POINTS 1 ASAWOOD'S COWBOY GENERAL, PCCISB 33093J3 WD,BOW 5 Owner : CARMELITA & JOEY MANCILLA Breeder: CARMELITA & JOEY MANCILLA 4 LORD OF THE NIGHTS I-CIRO, PCCISB 32593J3 RWD 0 Owner : CLYDE S NEBRES Breeder: CLYDE S NEBRES 7 PHIL/JR CH ZACK I DE AKIDO SAN (ARG), PCCISB 32540J3 RBD,AOM 0 Owner : EDWIN L OLIVAREZ Breeder: LARUCCIA, ANDREA FABIANA 10 PHIL CH NACHO DE AKIDO SAN (ARG), PCCISB 32499J3 BOB,BD,BISS 5 Owner : RONNIE F NATIVIDAD & EUGENE CHUA Breeder: LARUCCIA, ANDREA FABIANA 15 MICK RICKS REMEMBRANCE OF ASAWOOD (USA), PCCISB 32488J3 WB 5 Owner : JOEY,CARMENCITA,KEVIN MANCILLA & GRACE KELLY Breeder: MICHRLE LAUZON & KAREN BAHR 16 WIND DANCE DE BLACK SHADOW (ARG), PCCISB 32932J3 RWB 0 Owner : DR. PABLO R OLIVAREZ Breeder: ELSA BEATRIZ CAMPISCIANO/JUAN CARLOS 22 PHIL GR CH TOOTSIE DE AKIDO SAN (ARG), PCCISB 32498J3 BOS,BB 5 Owner : DR. PABLO R OLIVAREZ Breeder: LARUCCIA, ANDREA FABIANA 23 PHIL HOF/PW'15/SEA/APAC CH BACCARAT AKIRA V REBELYEL, PCCISB 3 RBB,BPB,BPBISS 0 Owner : EDRICH CABRERA Breeder: RICHARD THOMAS JOSON/ROLAND JOSEPH PDF 121ST PDF BREED SPECIALTY DOG SHOW December 04, 2016 PCCI ACTIVITY CENTER, MARIKINA CITY PINSCHER AND SCHNAUZER - MOLOSSOID BREEDS DOBERMANN LORELEI UY (PHILIPPINES) ENTRY # NAME OF DOG, PCCISB No. AWARDS POINTS 4 LORD OF THE NIGHTS I-CIRO, PCCISB 32593J3 RWD 0 Owner : CLYDE S NEBRES Breeder: CLYDE S NEBRES 6 KINTANAR'S PACIFIC RIM, PCCISB 31367J3 WD,BOW 5 Owner : ESAKU FRANCIS OTSUKI & IMELDA B MARTINEZ Breeder: MRS. -

The Miniature Schnauzer Origin
THE MINIATURE SCHNAUZER ORIGIN: Miniature Schnauzers were originally developed in the 19th century in Germany where they were used to guard livestock and chase vermin. Their name is derived from the word “Schnauze” which means “muzzle.” They were developed by cross breeding small Standard Schnauzers with the Affenpinscher or Poodle. They still make a good watchdog today, but their primary function is that of a household pet. PERSONALITY: This little dog is very intelligent and easy to train. They are active, alert, spirited, friendly, and loyal. Since they were bred to chase vermin, they can be aggressive towards small animals. They are extremely protective and want to please their family. As with any dog, you must teach young children how to properly play with them to avoid any unintentional injuries. APPEARANCE: Miniature Schnauzers usually weigh between 10 to 18 pounds, and their height averages between 11 and 14 inches tall. They have a square-shaped body that is surprisingly muscular for such a small dog. Their ears may be cropped to stand erect or left long to fold over. Eyebrows on a Miniature Schnauzer are distinctive and arched, and their whiskers are long and the fur grows into a “beard” on both sexes. Traditional colors of Miniature Schnauzers are black, black & white or salt and pepper with their coat being wiry. INTERESTING FACTS: Miniature Schnauzers are the 6th most popular dog registered with America's Pet Registry Inc. As this little dog doesn’t shed much, they are considered hypoallergenic. According to Stanley Coren in his book The Intelligence of Dogs, the Miniature Schnauzer rates under “Excellent Working Dogs” as number 12 with understanding 5 to 15 repetitions of new commands and obeys the first command 85 percent of the time or better.