American Urological Association (AUA) Guideline
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Interpretation of Canine and Feline Urinalysis
$50. 00 Interpretation of Canine and Feline Urinalysis Dennis J. Chew, DVM Stephen P. DiBartola, DVM Clinical Handbook Series Interpretation of Canine and Feline Urinalysis Dennis J. Chew, DVM Stephen P. DiBartola, DVM Clinical Handbook Series Preface Urine is that golden body fluid that has the potential to reveal the answers to many of the body’s mysteries. As Thomas McCrae (1870-1935) said, “More is missed by not looking than not knowing.” And so, the authors would like to dedicate this handbook to three pioneers of veterinary nephrology and urology who emphasized the importance of “looking,” that is, the importance of conducting routine urinalysis in the diagnosis and treatment of diseases of dogs and cats. To Dr. Carl A. Osborne , for his tireless campaign to convince veterinarians of the importance of routine urinalysis; to Dr. Richard C. Scott , for his emphasis on evaluation of fresh urine sediments; and to Dr. Gerald V. Ling for his advancement of the technique of cystocentesis. Published by The Gloyd Group, Inc. Wilmington, Delaware © 2004 by Nestlé Purina PetCare Company. All rights reserved. Printed in the United States of America. Nestlé Purina PetCare Company: Checkerboard Square, Saint Louis, Missouri, 63188 First printing, 1998. Laboratory slides reproduced by permission of Dennis J. Chew, DVM and Stephen P. DiBartola, DVM. This book is protected by copyright. ISBN 0-9678005-2-8 Table of Contents Introduction ............................................1 Part I Chapter 1 Sample Collection ...............................................5 -

A Dipstick Test Combined with Urine Specific Gravity Improved the Accuracy of Proteinuria Determination in Pregnancy Screening
Kobe J. Med. Sci., Vol. 56, No. 4, pp. E165-E172, 2010 A Dipstick Test Combined with Urine Specific Gravity Improved the Accuracy of Proteinuria Determination in Pregnancy Screening NATSUKO MAKIHARA1, MINEO YAMASAKI1,2, HIROKI MORITA1, and HIDETO YAMADA1* 1Division of Obstetrics and Gynecology, Department of Surgery-related, and 2Division of Integrated Medical Education, Department of Community Medicine and Social Healthcare Science, Kobe University Graduate School of Medicine, 7-5-1 Kusunoki-cho, Chuo-ku, Kobe, 650-0017, Japan. Received 12 July 2010/ Accepted 20 August 2010 Key Words: dipstick test, pregnancy proteinuria, protein/creatinine ratio, urine specific gravity Proteinuria screening using a semi-quantitative dipstick test of the spot urine in antenatal clinic is known to have high false-positive rates. The aim of this study was to assess availability of a dipstick test combined with the urine specific gravity for the determination of pathological proteinuria. A dipstick test was performed on 582 urine samples obtained from 283 pregnant women comprising 260 with normal blood pressure and 23 with pregnancy-induced hypertension. The urine protein (P) and creatinine (C) concentrations, specific gravity (SG), P/C ratio were determined, and compared with dipstick test results. The P concentration increased along the stepwise augmentations in dipstick test result. Frequencies of the urine samples with 0.265 or more P/C ratio were 0.7% with − dipstick test result, 0.7% with the ± result, 3.3% with the 1+ result, and 88.9% with the ≥2+ result. However, if the urine specific gravity was low, frequencies of the high P/C ratio were 5.0% with ± dipstick test result and 9.3% with the 1+ result. -

Specific Gravity, Urine
Lab Dept: Urine/Stool Test Name: SPECIFIC GRAVITY, URINE General Information Lab Order Codes: USG Synonyms: N/A CPT Codes: 81003 – Urinalysis; automated, without microscopy Test Includes: Specific gravity measurement by colorimetric reagent strip. Logistics Test Indications: Useful for evaluating the concentrating and excretory power of the kidney. Lab Testing Sections: Urinalysis Phone Numbers: MIN Lab: 612-813-6280 STP Lab: 651-220-6550 Test Availability: Daily, 24 hours Turnaround Time: 2 - 4 hours Special Instructions: Indicate method of collection on request form (catheterized, clean- catch, or void). Deliver to lab within 30 minutes of collection. Refrigerate specimen if there is a delay in transport of 30 minutes or more. Specimen Specimen Type: Urine Container: Urine cup Draw Volume: Entire urine collection Processed Volume: Minimum volume: 1 mL Collection: Collect a clean-catch urine specimen as follows: Males: Clean glans with soap and water. Rinse area with wet gauze pads. While holding foreskin retracted, begin voiding. After several mL’s have passed, collect midstream portion without stopping flow of urine. Place the cap on the cup and tighten securely. Refrigerate specimen after collection and promptly forward to the lab. Females: Thoroughly clean urethral area with soap and water. Rinse area with wet gauze pads. While holding labia apart, begin voiding. After several mL’s have passed, collect midstream portion without stopping the flow of urine. Place the cap on the cup and tighten securely. Refrigerate specimen after collection and promptly forward to the lab. Note: Indicate type of specimen (catheterized or void) and time of collection on the label. Special Processing: N/A Patient Preparation: See above Sample Rejection: Less than 1 mL urine; mislabeled or unlabeled specimens Interpretive Reference Range: Age: Specific Gravity: Infant (0 days - 1 year): 1.002 - 1.006 >1 year: 1.001 - 1.030 Critical Values: N/A Limitations: Radiographic dyes in urine increase the specific gravity by hydrometer or refractometer. -
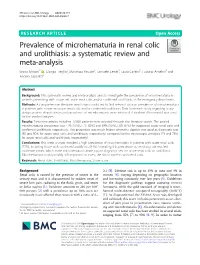
Prevalence of Microhematuria in Renal Colic and Urolithiasis: a Systematic Review and Meta-Analysis
Minotti et al. BMC Urology (2020) 20:119 https://doi.org/10.1186/s12894-020-00690-7 RESEARCH ARTICLE Open Access Prevalence of microhematuria in renal colic and urolithiasis: a systematic review and meta-analysis Bruno Minotti1* , Giorgio Treglia2, Mariarosa Pascale3, Samuele Ceruti4, Laura Cantini5, Luciano Anselmi5 and Andrea Saporito5 Abstract Background: This systematic review and meta-analysis aims to investigate the prevalence of microhematuria in patients presenting with suspected acute renal colic and/or confirmed urolithiasis at the emergency department. Methods: A comprehensive literature search was conducted to find relevant data on prevalence of microhematuria in patients with suspected acute renal colic and/or confirmed urolithiasis. Data from each study regarding study design, patient characteristics and prevalence of microhematuria were retrieved. A random effect-model was used for the pooled analyses. Results: Forty-nine articles including 15′860 patients were selected through the literature search. The pooled microhematuria prevalence was 77% (95%CI: 73–80%) and 84% (95%CI: 80–87%) for suspected acute renal colic and confirmed urolithiasis, respectively. This proportion was much higher when the dipstick was used as diagnostic test (80 and 90% for acute renal colic and urolithiasis, respectively) compared to the microscopic urinalysis (74 and 78% for acute renal colic and urolithiasis, respectively). Conclusions: This meta-analysis revealed a high prevalence of microhematuria in patients with acute renal colic (77%), including those with confirmed urolithiasis (84%). Intending this prevalence as sensitivity, we reached moderate values, which make microhematuria alone a poor diagnostic test for acute renal colic or urolithiasis. Microhematuria could possibly still important to assess the risk in patients with renal colic. -

Urinary System Diseases and Disorders
URINARY SYSTEM DISEASES AND DISORDERS BERRYHILL & CASHION HS1 2017-2018 - CYSTITIS INFLAMMATION OF THE BLADDER CAUSE=PATHOGENS ENTERING THE URINARY MEATUS CYSTITIS • MORE COMMON IN FEMALES DUE TO SHORT URETHRA • SYMPTOMS=FREQUENT URINATION, HEMATURIA, LOWER BACK PAIN, BLADDER SPASM, FEVER • TREATMENT=ANTIBIOTICS, INCREASE FLUID INTAKE GLOMERULONEPHRITIS • AKA NEPHRITIS • INFLAMMATION OF THE GLOMERULUS • CAN BE ACUTE OR CHRONIC ACUTE GLOMERULONEPHRITIS • USUALLY FOLLOWS A STREPTOCOCCAL INFECTION LIKE STREP THROAT, SCARLET FEVER, RHEUMATIC FEVER • SYMPTOMS=CHILLS, FEVER, FATIGUE, EDEMA, OLIGURIA, HEMATURIA, ALBUMINURIA ACUTE GLOMERULONEPHRITIS • TREATMENT=REST, SALT RESTRICTION, MAINTAIN FLUID & ELECTROLYTE BALANCE, ANTIPYRETICS, DIURETICS, ANTIBIOTICS • WITH TREATMENT, KIDNEY FUNCTION IS USUALLY RESTORED, & PROGNOSIS IS GOOD CHRONIC GLOMERULONEPHRITIS • REPEATED CASES OF ACUTE NEPHRITIS CAN CAUSE CHRONIC NEPHRITIS • PROGRESSIVE, CAUSES SCARRING & SCLEROSING OF GLOMERULI • EARLY SYMPTOMS=HEMATURIA, ALBUMINURIA, HTN • WITH DISEASE PROGRESSION MORE GLOMERULI ARE DESTROYED CHRONIC GLOMERULONEPHRITIS • LATER SYMPTOMS=EDEMA, FATIGUE, ANEMIA, HTN, ANOREXIA, WEIGHT LOSS, CHF, PYURIA, RENAL FAILURE, DEATH • TREATMENT=LOW NA DIET, ANTIHYPERTENSIVE MEDS, MAINTAIN FLUIDS & ELECTROLYTES, HEMODIALYSIS, KIDNEY TRANSPLANT WHEN BOTH KIDNEYS ARE SEVERELY DAMAGED PYELONEPHRITIS • INFLAMMATION OF THE KIDNEY & RENAL PELVIS • CAUSE=PYOGENIC (PUS-FORMING) BACTERIA • SYMPTOMS=CHILLS, FEVER, BACK PAIN, FATIGUE, DYSURIA, HEMATURIA, PYURIA • TREATMENT=ANTIBIOTICS, -

Role of Urinalysis in the Diagnosis of Chronic Kidney Disease (CKD)
Research and Reviews Role of Urinalysis in the Diagnosis of Chronic Kidney Disease (CKD) JMAJ 54(1): 27–30, 2011 Kunitoshi ISEKI*1 Abstract As of the end of Year 2008, 1 out of 450 people was a dialysis patient in Japan, and patients with chronic kidney disease (CKD) at stages 3 and 4 accounted for nearly 10% of the total population. An epidemiological study in Okinawa that used the introduction of dialysis treatment as the outcome revealed that the 10-year cumulative incident rate of end-stage renal disease (ESRD) was about 3% of the participants who were positive (Ն 1ϩ) for both proteinuria and hematuria, while there was hardly any difference between those who were positive for hematuria alone and those who were negative for both proteinuria and hematuria. When the incidence of ESRD (dialysis introduction) was examined in relation to the severity of proteinuria (5 grades ranging from [Ϫ] to [Ն 3ϩ]) as determined by dipstick, the cumulative incidence rate during the 17-year observation period was 16% for proteinuria (Ն 3ϩ) and about 7% for proteinuria (2ϩ). In contrast, among participants who were negative for proteinuria, the rate of dialysis introduction in 10 years is about 1 out of 1 million. The CKD Practice Guide of the Japanese Society of Nephrology recommends referral to a nephrologist when a case meets any of the following 3 criteria: 1) 0.5g/g creatinine or higher, or proteinuria (Ն 2ϩ), 2) an estimated glomerular filtration rate of less than 50ml/min/1.73m2, or 3) positive results (Ն 1ϩ) for both proteinuria and hematuria tests. -

Hematuria in the Child
Hematuria and Proteinuria in the Pediatric Patient Laurie Fouser, MD Pediatric Nephrology Swedish Pediatric Specialty Care Hematuria in the Child • Definition • ³ 1+ on dipstick on three urines over three weeks • 5 RBCs/hpf on three fresh urines over three weeks • Prevalence • 4-6% for microscopic hematuria on a single specimen in school age children • 0.3-0.5% on repeated specimens Sources of Hematuria • Glomerular or “Upper Tract” – Dysmorphic RBCs and RBC casts – Tea or cola colored urine – Proteinuria, WBC casts, renal tubular cells • Non-Glomerular or “Lower Tract” – RBCs have normal morphology – Clots/ Bright red or pink urine The Glomerular Capillary Wall The Glomerular Capillary Wall Glomerular Causes of Hematuria • Benign or self-limiting – Benign Familial Hematuria – Exercise-Induced Hematuria – Fever-Induced Hematuria Glomerular Causes of Hematuria • Acute Glomerular Disease – Poststreptococcal/ Postinfectious – Henoch-Schönlein Purpura – Sickle Cell Disease – Hemolytic Uremic Syndrome Glomerular Causes of Hematuria • Chronic Glomerular Disease – IgA Nephropathy – Henoch-Schönlein Purpura or other Vasculitis – Alport Syndrome – SLE or other Collagen Vascular Disease – Proliferative Glomerulonephritis Non-Glomerular Hematuria • Extra-Renal • UTI • Benign urethralgia +/- meatal stenosis • Calculus • Vesicoureteral Reflux, Hydronephrosis • Foreign body • Rhabdomyosarcoma • AV M • Coagulation disorder Non-Glomerular Hematuria • Intra-Renal • Hypercalciuria • Polycystic Kidney Disease • Reflux Nephropathy with Renal Dysplasia • -

Hematuria Is a Risk Factor Towards End-Stage Renal
Nephrology and Renal Diseases Research Article Hematuria is a risk factor towards end-stage renal disease - A propensity score analysis Tomoko Shima* Department of Internal Medicine, Teikyo University School of Medicine, Tokyo, Japan Abstract Background: It remains unclear whether microscopic hematuria accelerates the progression of chronic kidney disease (CKD). Since the risk of microscopic hematuria was expected very weak, we employed a propensity score analysis. Methods: A retrospective CKD cohort of 803 participants in a single institution was analyzed. The degree of microscopic hematuria was scaled as 0, 0.5, 1, 2, 3 for negative, ±, 1+, 2+, 3+ in the urinary qualitative analysis by dipstick, respectively. Time-averaged microscopic hematuria (TA-MH) was calculated by trapezoidal rule. The propensity score was estimated using 23 baseline covariates by multivariate binary logistic regression for the threshold of TA-MH at ≥ 0.5 or ≥ 1.0. Kaplan-Meier analysis after propensity score matching was also examined. Results: The incidence rate of end-stage renal disease (ESRD) was 33.9 per 1,000 person-years over median follow-up of 4.3 years. A Cox regression analysis stratified by quintile on the propensity scores showed that TA-MH ≥ 0.5 was a risk for ESRD (HR 1.72, 95% CI 1.08-2.75, p = 0.023) but not TA-MH ≥ 1.0 (HR 1.34, 95% CI 0.76-2.40, p = 0.315). Kaplan-Meier analysis after propensity score matching reproduced the similar results (TA-MH ≥ 0.5, HR 1.80, 95% CI 1.03-3.12, p = 0.046; TA-MH ≥ 1.0, HR 1.73, 95% CI 0.84-3.54, p = 0.145). -
Urine Specific Gravity
Please purchase PDFcamp Printer on http://www.verypdf.com/ to remove this watermark. Urine Specific Gravity Urine Specific Gravity (SG) Specific gravity (SG) is a measurement of the kidneys' ability to concentrate urine. The test compares the density of urine against the density of distilled water, which has an SG of 1.000. Because urine is a solution of minerals, salts, and compounds dissolved in water, the SG is a measure of the density of the dissolved chemicals in the specimen. As a measurement of specimen density, SG is influenced by both the number of particles present and the size of the particles. Osmolality is a more exact measurement and may be needed in certain circumstances. Please purchase PDFcamp Printer on http://www.verypdf.com/ to remove this watermark. • The range of urine SG depends on the state of hydration and varies with urine volume and the load of solids to be excreted under standardized conditions; when fluid intake is restricted or increased, SG measures the concentrating and diluting functions of the kidney. Loss of these functions is an indication of renal dysfunction. Please purchase PDFcamp Printer on http://www.verypdf.com/ to remove this watermark. • Reference Values • Normal • 1.005-1.030 (usually between 1.010 and 1.025) • Concentrated urine: 1.025-1.030+ • Dilute urine: 1.001-1.010 • Infant < 2 years old: 1.001-1.018 Please purchase PDFcamp Printer on http://www.verypdf.com/ to remove this watermark. • Procedure • Test SG with the use of a multiple-test dipstick that has a separate reagent area for SG. -

Blood Or Protein in the Urine: How Much of a Work up Is Needed?
Blood or Protein in the Urine: How much of a work up is needed? Diego H. Aviles, M.D. Disclosure • In the past 12 months, I have not had a significant financial interest or other relationship with the manufacturers of the products or providers of the services discussed in my presentation • This presentation will not include discussion of pharmaceuticals or devices that have not been approved by the FDA Screening Urinalysis • Since 2007, the AAP no longer recommends to perform screening urine dipstick • Testing based on risk factors might be a more effective strategy • Many practices continue to order screening urine dipsticks Outline • Hematuria – Definition – Causes – Evaluation • Proteinuria – Definition – Causes – Evaluation • Cases You are about to leave when… • 10 year old female seen for 3 day history URI symptoms and fever. Urine dipstick showed 2+ for blood and no protein. Questions? • What is the etiology for the hematuria? • What kind of evaluation should be pursued? • Is this an indication of a serious renal condition? • When to refer to a Pediatric Nephrologist? Hematuria: Definition • Dipstick > 1+ (large variability) – RBC vs. free Hgb – RBC lysis common • > 5 RBC/hpf in centrifuged urine • Can be – Microscopic – Macroscopic Hematuria: Epidemiology • Microscopic hematuria occurs 4-6% with single urine evaluation • 0.1-0.5% of school children with repeated testing • Gross hematuria occurs in 1/1300 Localization of Hematuria • Kidney – Brown or coke-colored urine – Cellular casts • Lower tract – Terminal gross hematuria – (Blood -

Reliability of Three Urinalysis Methods Used in the Assessment of Hydration
International Journal of Sport, Exercise and Health Research 2018; 2(2): 100-105 Research Article Reliability of three urinalysis methods used in the IJSEHR 2018; 2(2): 100-105 © 2018, All rights reserved assessment of hydration www.sportscienceresearch.com Received: 30-08-2018 Aric J. Warren1, Matthew S. O’Brien1, Doug B. Smith2 Accepted: 18-10-2018 1 Associate Professor, Department of Athletic Training, Oklahoma State University Center for Health Sciences, 1111 W. 17th Street, Tulsa, OK 74107, USA 2 Professor, Oklahoma State University, School of Kinesiology, Applied Health and Recreation, Stillwater, OK 74078, USA Abstract Objective: The purpose of this study was to determine the intratester and intertester reliability of three common methods of assessing hydration; urine color chart (UCC), dipstick reagent strip (DRS) and refractometer (REF). Methods: Twenty-three male collegiate wrestlers (n = 23, age = 20.09 ± 1.35, weight = 78.73 ± 11.25 kg, height = 174.49 ± 7.23 cm) provided urine samples on three separate occasions totaling 69 samples (n = 69). Samples were analyzed with repeated measures by three testers, three trials, and three separate methods of assessment. Results: All methods had very high intertester reliability as demonstrated by Cronbach’s Alpha coefficients; DRS (r = .985), UCC (r = .973) and REF (r = .968). Intraclass correlation coefficient ranges were also very high; DRS .983 - .994, UCC 964-.983, and REF .829-.996. Conclusions: The three modes of urine hydration assessment are highly reliable, and are a practical, noninvasive method to evaluate hydration status in the field. Keywords: Hydration; Reliability; Urinalysis. INTRODUCTION Athletes that compete in body weight restrictive sports such as wrestling, judo, and rowing sometimes go to extreme measures to qualify for a specific weight class or event. -

Diagnostic Utility of Microhematuria in Renal Colic Patients in Emergency Medicine: Correlation with Findings from Multidetector Computed Tomography
Available online at www.medicinescience.org Medicine Science ORIGINAL RESEARCH International Medical Journal Medicine Science 2019; ( ): Diagnostic utility of microhematuria in renal colic patients in emergency medicine: correlation with findings from multidetector computed tomography Murat Daş ORCID: 0000-0003-0893-6084 Okan Bardakci ORCID: 0000-0001-6829-7435 Erşan Yurtseven ORCID: 0000-0003-0469-5260 Canan Akman ORCID: 0000-0002-3427-5649 Yavuz Beyazit ORCID: 0000-0001-6247-2714 Okhan Akdur ORCID: 0000-0003-3099-6876 1Canakkale Onsekiz Mart Universty, Faculty of Medicine, Department of Emergency Medicine, Canakkale, Turkey 2Canakkale Onsekiz Mart Universty, Department of Internal Medicine, Canakkale, Turkey Received 19 November2018; Accepted 28 December 2018 Available online 30.01.2019 with doi:10.5455/medscience.2018.07.8974 Copyright © 2019 by authors and Medicine Science Publishing Inc. Abstract Although urine analysis is a simple and inexpensive method for the initial evaluation of renal colic patients presenting in emergency departments, it is regarded as unreliable for an exact diagnosis of urinary system stones. The aim of the present study is to assess the association between clinical demographics, and stone size and location, with the combined utility of urinalysis and unenhanced multidetector computed tomography (MDCT) in the emergency department. After gaining local Ethics Committee approval, a retrospective study was conducted with data from 186 patients who presented at our emergency service with flank pain and documented urolithiasis. Stone location and size was determined by MDCT, and the presence of microhematuria confirmed by urinalysis. The presence of hydronephrosis and clinical complaints were also recorded. A total of 186 patients were included in the present study, in which an absence of microhematuria was recorded in 24.7% patients.