Reliability of Current Estimates of Schistosomiasis Prevalence in The
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Universidade Federal De Pernambuco Centro De Tecnologia E Geociências Departamento De Engenharia Civil Programa De Pós-Graduação Em Engenharia Civil
UNIVERSIDADE FEDERAL DE PERNAMBUCO CENTRO DE TECNOLOGIA E GEOCIÊNCIAS DEPARTAMENTO DE ENGENHARIA CIVIL PROGRAMA DE PÓS-GRADUAÇÃO EM ENGENHARIA CIVIL GADADHARA DE FIGUEIREDO FERRAZ SIMULAÇÃO HIDROLÓGICA E HIDRODINÂMICA DO IMPACTO DE ENCHENTES NA BACIA DO RIO SIRINHAÉM E AVALIAÇÃO DE SISTEMA DE CONTROLE PROPOSTO Recife 2019 GADADHARA DE FIGUEIREDO FERRAZ SIMULAÇÃO HIDROLÓGICA E HIDRODINÂMICA DO IMPACTO DE ENCHENTES NA BACIA DO RIO SIRINHAÉM E AVALIAÇÃO DE SISTEMA DE CONTROLE PROPOSTO Dissertação apresentada ao Programa de Pós-graduação em Engenharia Civil do Centro de Tecnologia e Geociências da Universidade Federal de Pernambuco, como requisito parcial à obtenção do grau de Mestre em Engenharia Civil. Área de concentração: Tecnologia Ambiental e Recursos Hídricos. Orientador: Profº. Dr. José Almir Cirilo. Recife 2019 Catalogação na fonte Bibliotecária Maria Luiza de Moura Ferreira, CRB-4 / 1469 F381s Ferraz, Gadadhara de Figueiredo. Simulação hidrológica e hidrodinâmica do impacto de enchentes na bacia do rio Sirinhaém e avaliação de sistema de controle proposto / Gadadhara de Figueiredo Ferraz. - 2019. 117 folhas, il., tabs., abr. e sigl. Orientador: Profº. Dr. José Almir Cirilo. Dissertação (Mestrado) – Universidade Federal de Pernambuco. CTG. Programa de Pós-Graduação em Engenharia Civil, 2019. Inclui Referências. 1. Engenharia Civil. 2. HEC-HAS. 3. CAWM V. 4. Controle de cheias. I. Cirilo, José Almir Cirilo (Orientador). II. Título. UFPE 624 CDD (22. ed.) BCTG/2019-186 GADADHARA DE FIGUEIREDO FERRAZ SIMULAÇÃO HIDROLÓGICA E HIDRODINÂMICA DO IMPACTO DE ENCHENTES NA BACIA DO RIO SIRINHAÉM E AVALIAÇÃO DE SISTEMA DE CONTROLE PROPOSTO Dissertação apresentada ao Programa de Pós-graduação em Engenharia Civil do Centro de Tecnologia e Geociências da Universidade Federal de Pernambuco, como requisito parcial à obtenção do grau de Mestre em Engenharia Civil, área de Tecnologia Ambiental e Recursos Hídricos. -
O C E a N O Atlâ N Tic O
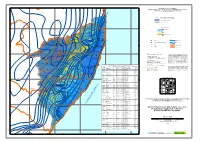
W. Gr -37° 400 480 -36° 560 -35° 640 720 -34° MINISTÉRIO DE MINAS E ENERGIA Cabedelo P SECRETARIA DE GEOLOGIA, MINERAÇÃO E TRANSFORMAÇÃO MINERAL -7° 0 0 -7° 0 0 COMPANHIA DE PESQUISA DE RECURSOS MINERAIS 6 4 1 Serviço Geológico do Brasil 6 0 0 0 0 5 JOÃO PESSOA P Rio Cuiá a Estações pluviométricas selecionadas mbab Rio Mu a " e u para o estudo do Projeto Atlas Pluviométrico m g a Á aba amu m Pa Conde a o M r io B R G Isoietas totais anuais (mm) o io i R R Ri o G R ara io u A Limite sub-bacia 39 PARAÍBA t e r R Itambé r io M Itambé (Ipa), 1143 mPm o ucatu P Camutan"ga Alhandra Rio PERNAMBUCO P Abia Pedras de Fogo P í P a Ferreiros ang Tiúma Pit io Rio P R Guararema Pitimbu T PTimbaúba Caaporã Precipitação Média Anual ch. FariP 9160 0 R a 9160 gi s an 0 Macaparana Cru 1 Valor máximo : 2.118 mm P io Goiana Megão R o 1 P i i São Vicente Ferrer rig R P Si P io RP Aliança Goiana (Itapirema - Ipa), 1809 mm P Itaquitinga " iro 0 Vicência ibe P Umbuzeiro, 931 mm Rio R 0 Machados P im 4 d 400 " Buenos Aires ar Valor mínimo : 394 mm 1 J o . Casinhas Or b ch ó P P Orobó Rio Buenos Aire"s, 1032 mm R Ilha de Itamaracá P P mP Santa Cecília " é Nazaré da Mata P Bom Jardim, 909 mm ha do Gr P Vertente do Lério un P . -

Programa Federativo De Enfrentamento Ao Coronavírus No Estado De Pernambuco
+ Programa Federativo de Enfrentamento ao Coronavírus no Estado de Pernambuco Os valores destinados ao Estado de Pernambuco, decorrentes da distribuição estabelecida nos termos do Programa Federativo de Enfrentamento ao Coronavírus, são os seguintes: - dentre os recursos a serem aplicados na área de saúde pública: - R$ 368 milhões para o Estado, conforme critérios de população e incidência de COVID-19*; - R$ 136 milhões para os Municípios, conforme critério populacional; - R$ 1,078 bilhão de livre aplicação, pertencentes ao Estado; - R$ 730 milhões de livre aplicação, pertencentes aos Municípios; - R$ 1,465 bilhão pela suspensão no pagamento da dívida* com organismos internacionais e com a União, incluindo dívidas do Estado e dos respectivos Municípios. O total é de R$ 3,776 bilhões, mas além desses valores ainda é necessário somar a eventual dívida com bancos privados. *Observação: os dados relativos à suspensão de dívidas foram fornecidos pelo Ministério da Economia, e os referentes à incidência de COVID-19 em 29/04/2020, pelo Ministério da Saúde. % Recebido Auxílio Recebido pelo Pop. Estimada UF Município pelo Município [IBGE] Município (total nacional de 20+3bi) PE Abreu e Lima 99.990 1,05% R$ 9.062.220,11 PE Afogados da Ingazeira 37.259 0,39% R$ 3.376.830,27 PE Afrânio 19.635 0,21% R$ 1.779.544,87 PE Agrestina 24.885 0,26% R$ 2.255.359,01 PE Água Preta 36.771 0,38% R$ 3.332.602,22 PE Águas Belas 43.443 0,45% R$ 3.937.294,01 PE Alagoinha 14.636 0,15% R$ 1.326.479,18 PE Aliança 38.386 0,40% R$ 3.478.971,71 PE Altinho 22.972 0,24% R$ -

Rua Da Aurora
POLÍCIA CIVIL DE PERNAMBUCO DIRETORIA DE TECNOLOGIA DA INFORMAÇÃO GESTÃO DE TELEMÁTICA CHEFIA DE POLÍCIA CIVIL Endereço: Rua da Aurora, 405 - Boa Vista – Recife/PE - CEP: 50.050-000 Fones: (81) GABPCPE - Chefia de Polícia 3184-3803 ASSGAB - Assessoria da Chefia 3184-3813 SEGAB – Secretaria da Chefia 3184-3805 Permanência 3184-3800 E-mail: [email protected] SUBCHEFIA DE POLÍCIA CIVIL Endereço: Rua da Aurora, 405 - Boa Vista – Recife/PE - CEP: 50.050-000 Fones: (81) SUBCP - Subchefia de Polícia 3184-3814 / 3184-3812 ASSUBCP - Assessoria da Subchefia 3184-3809 / 3184-3810 ASSCOM – Assessoria de Comunicação Social da Polícia Civil – 3184-3823 / 3184-3824 / 3184-3825 E-mail: [email protected] DIVAC – Divisão de Administração e Controle 3184-3816 ASSCOM – ASSESSORIA DE COMUNICAÇÃO SOCIAL Endereço: Rua da Aurora, 405 - Boa Vista – Recife/PE - CEP: 50.050-000 Fones: (81) Chefe 3184-3823 Seção Administrativa 3184-3824, 3184-3825 E-mail: [email protected] UNICEV - UNIDADE DE PLANEJAMENTO E COORDENAÇÃO DE EVENTOS Endereço: Rua da Aurora, 487 – Boa Vista – Recife/PE - CEP: 50.050-000 Fones: (81) Chefe 3184-3255 E-mail: [email protected] UNAJUR – UNIDADE APOIO JURÍDICO Endereço: Rua da Aurora, 405 - Boa Vista – Recife/PE - CEP: 50.050-000 Fones: (81) Chefe 3184-3819 Seção Administrativa 3184-3820 E-mail: [email protected] UCI/SUBCP - UNIDADE DE CONTROLE INTERNO Endereço: Rua da Aurora, 405 - Boa Vista – Recife/PE - CEP: 50.050-000 Fones: (81) 3184-3821 DIVCAC – Divisão de Controladoria -

3.6 Sirinhaém
Agência Estadual de Meio Ambiente 80 Diretoria de Recursos Hídricos e Florestais Supervisão de Gestão de Recursos Hídricos 3.6 SIRINHAÉM Área de drenagem: 2.069,60Km2 Municípios: Água Preta (parte), Amaraji (sede), Barra da Guabiraba (sede), Bonito (parte), Camocim de São Félix (sede), Cortês, Escada (parte), Gameleira (sede), Gravatá (parte), Ipojuca (parte), Joaquim Nabuco (parte), Primavera (parte), Ribeirão, Rio Formoso (parte), Sairé (sede), São Joaquim do Monte (parte), Sirinhaém (sede), Tamandaré (parte). População: 181.703 habitantes Urbana: 100.770 habitantes Rural: 80.933 habitantes Constituintes principais: Rios Amaraji, Oncinha, Machado, Bonito Grande, Tanque de Piabas, Várzea Grande, Camaragibe, Tapiruçu, Aripibu, Caranguejo e Brejo Novo. Reservatórios: Brejão. Uso do solo: • Ocupação urbana e industrial. • Policultura. • Áreas de Mata Atlântica e Manguezal. Áreas de proteção: APA de Sirinhaém e APA de Guadalupe. Uso da água: • Abastecimento público. • Recepção de efluentes domésticos. • Recepção de efluentes agroindustrial e industrial. Atividades industriais na bacia: Sucroalcooleira, produtos alimentares e borracha. Agência Estadual de Meio Ambiente 81 Diretoria de Recursos Hídricos e Florestais Supervisão de Gestão de Recursos Hídricos Diagrama unifilar Amaraji/Matadouro Amaraji/Matadouro 30Km U. Montevideu U. Montevideu iche p Rio Siribó Camela Camela 12Km Rio Tapicurú Tapicurú Rio Ribeirão / Matadouro Ribeirão municipal 3Km Rio Camaragibe Gameleira U. Pedrosa Rio Amaraji Amaraji Rio Usina Tra Usina Usina Cucaú Cucaú -

Municípios Com Operação Regular Do Aterro Sanitário
Municípios com Operação Regular do Aterro Sanitário Apuração 2012 Apuração 2013 Apuração 2014 (Fonte CPRH) (Fonte CPRH) (Fonte CPRH) 1 Abreu e Lima Abreu e Lima Abreu e Lima 2 Agrestina Agrestina Agrestina 3 Alagoinha Alagoinha Alagoinha 4 Altinho Altinho Altinho 5 Amaraji Amaraji Amaraji 6 Araçoiaba Araçoiaba Araçoiaba 7 Arcoverde Arcoverde Arcoverde 8 Barra de Guabiraba Barra de Guabiraba Barra de Guabiraba 9 Barreiros Barreiros Barreiros 10 Belém de Maria Belém de Maria Belém de Maria 11 Belo Jardim Belo Jardim Belo Jardim 12 Bonito Bonito Bonito 13 Buíque Buíque Buíque 14 Cabo de Santo Agostinho Cabo de Santo Agostinho Cabo de Santo Agostinho 15 Cachoeirinha Cachoeirinha Cachoeirinha 16 Caetés Caetés Caetés 17 Capoeiras Capoeiras Capoeiras 18 Caruaru Caruaru Caruaru 19 Chã Grande Chã Grande Chã Grande 20 Condado Condado Condado 21 Correntes Correntes Correntes 22 Cortês Cortês Cortês 23 Escada Escada Escada 24 Gameleira Gameleira Gameleira 25 Garanhuns Garanhuns Garanhuns 26 Gravatá Gravatá Gravatá 27 Goiana Goiana Goiana 28 Iati Iati Iati 29 Ibimirim Ibimirim Ibimirim 30 Ipojuca Ipojuca Ipojuca 31 Ibirajuba Ibirajuba Ibirajuba 32 Igarassu Igarassu Igarassu 33 Itamaracá Itamaracá Itamaracá 34 Itapissuma Itapissuma Itapissuma 35 Jaboatão dos Guararapes Jaboatão dos Guararapes Jaboatão dos Guararapes 36 Jurema Jurema Jurema 37 Lagoa do Ouro Lagoa do Ouro Lagoa do Ouro 38 Lagoa dos Gatos Lagoa dos Gatos Lagoa dos Gatos 39 Lajedo Lajedo Lajedo 40 Moreno Moreno Moreno 41 Olinda Olinda Olinda 42 Paulista Paulista Paulista 43 Pesqueira Pesqueira -

Universidade Federal De Pernambuco Centro De Filosofia E Ciências Humanas Departamento De Ciências Geográficas Programa De Pós-Graduação Em Geografia
UNIVERSIDADE FEDERAL DE PERNAMBUCO CENTRO DE FILOSOFIA E CIÊNCIAS HUMANAS DEPARTAMENTO DE CIÊNCIAS GEOGRÁFICAS PROGRAMA DE PÓS-GRADUAÇÃO EM GEOGRAFIA DINÂMICAS ESPACIAIS E RESULTADOS SOCIOAMBIENTAIS EM ASSENTAMENTOS DE REFORMA AGRÁRIA: A ESPACIALIZAÇÃO NO ASSENTAMENTO ESTIVAS EM AMARAJI - PE ELIANA MARIA VIEIRALVES LINHARES RECIFE 2006 ELIANA MARIA VIEIRALVES LINHARES DINÂMICAS ESPACIAIS E RESULTADOS SOCIOAMBIENTAIS EM ASSENTAMENTOS DE REFORMA AGRÁRIA: A ESPACIALIZAÇÃO NO ASSENTAMENTO ESTIVAS EM AMARAJI - PE Dissertação apresentada ao Programa de Pós- graduação em Geografia do Departamento Ciências Geográficas da Universidade Federal de Pernambuco, como parte dos requisitos necessários à obtenção do grau de Mestre em Geografia. Orientadora: Profa. Dra. Vanice Santiago Fragoso Selva RECIFE 2006 L755d Linhares, Eliana Maria Vieiralves Dinâmicas espaciais e resultados socioambientais em assentamentos de reforma agrária: a espacialização no assentamento Estivas em Amaraji - PE. – Recife: O Autor, 2006. 135 folhas: il., tab., graf., quadros, fotos, mapas. Orientadora: Vanice Santiago Fragoso Selva Dissertação (mestrado) – Universidade Federal de Pernambuco. CFCH. Programa de Pós-graduação em Geografia. Recife, 2006. Inclui bibliografia e apêndice. 1. Reforma agrária. 2. Assentamento rural. 3. Produção familiar. 4. Conflitos fundiários. I. Título. 333.013.6 CDU (2.ed.) UFPE 333.31 CDD (22.ed.) BCFCH2006/31 Ao meu marido Edson, eterno companheiro de muitas lutas, às minhas filhas Isabela e Karina, às minhas netas Camila e Júlia, pelo apoio, paciência e estímulo para a realização deste trabalho. AGRADECIMENTOS As contribuições recebidas para a realização desta pesquisa foram inúmeras ao longo dos dois anos em que esta dissertação foi elaborada. Muitas foram as pessoas que me proporcionaram os mais variados tipos de apoio, a quem desejo deixar registrados os meus agradecimentos: Inicialmente, à minha orientadora, Profa. -

Tribunal De Justiça De Pernambuco Poder Judiciário
PODER JUDICIÁRIO TRIBUNAL DE JUSTIÇA DE PERNAMBUCO Entrânci Grau Cidade Órgão Jurisdicional email a 1 2 ABREU E LIMA 1ª VARA CÍVEL DA COMARCA DE ABREU E LIMA [email protected] 1 2 ABREU E LIMA 2ª VARA CÍVEL DA COMARCA DE ABREU E LIMA [email protected] 1 2 ABREU E LIMA 3ª VARA CÍVEL DA COMARCA DE ABREU E LIMA [email protected] 1 2 ABREU E LIMA VARA CRIMINAL DA COMARCA DE ABREU E LIMA [email protected] 1 2 AFOGADOS DA INGAZEIRA 1ª VARA CÍVEL DA COMARCA DE AFOGADOS DA INGAZEIRA [email protected] 1 2 AFOGADOS DA INGAZEIRA 2ª VARA CÍVEL DA COMARCA DE AFOGADOS DA INGAZEIRA [email protected] 1 2 AFOGADOS DA INGAZEIRA CENTRO JUDICIÁRIO DE SOLUÇÃO DE CONFLITOS E CIDADANIA DA COMARCA DE AFOGADOS DA INGAZEIRA [email protected] 1 2 AFOGADOS DA INGAZEIRA VARA CRIMINAL DA COMARCA DE AFOGADOS DA INGAZEIRA [email protected] 1 2 AFOGADOS DA INGAZEIRA VARA REGIONAL DA INFÂNCIA E JUVENTUDE DA 13ª CIRCUNSCRIÇÃO - AFOGADOS DA INGAZEIRA [email protected] 1 1 AFRÂNIO VARA ÚNICA DA COMARCA DE AFRÂNIO [email protected] 1 1 AGRESTINA VARA ÚNICA DA COMARCA DE AGRESTINA [email protected] 1 2 AGUA PRETA 1ª VARA DA COMARCA DE ÁGUA PRETA [email protected] 1 2 AGUA PRETA 2ª VARA DA COMARCA DE ÁGUA PRETA [email protected] 1 1 AGUAS BELAS VARA ÚNICA DA COMARCA DE ÁGUAS BELAS [email protected] 1 1 ALAGOINHA VARA ÚNICA DA COMARCA DE ALAGOINHA [email protected] 1 1 ALIANÇA VARA ÚNICA DA COMARCA DE ALIANÇA -

Governo Entrega Obras Públicas Em Quipapá
Diário Oficial Estado de Pernambuco Ano XCIII • N0 113 Poder Executivo Recife, sábado, 18 de junho de 2016 ZONA DA MATA SUL Governo entrega obras públicas em Quipapá O governador Paulo Câmara cumpriu agenda no município da Zona da Mata Sul, nesta sexta-feira (17) e entregou dois novos equipamentos públicos à população local. FOTO: ALUISIO MOREIRA/SEI primeiro deles é o principalmente com a saúde, Abatedouro Regio- ofertando um produto de OO nal Luiz Buarque qualidade para toda a popu- Wanderley, que vai garantir lação”, afirmou o secretário uma maior qualidade no de Agricultura e Reforma fornecimento de carnes para Agrária, Nilton Mota. Ao os moradores da região. O todo, serão beneficiadas outro é a nova sede da Escola cerca de 75 mil pessoas dos Municipal João Antônio de municípios de Quipapá, Souza Filho, que tem São Benedito do Sul, Jaquei- capacidade para atender 300 ra e Panelas. estudantes do 10 ao 50 ano. A unidade de ensino rece- FEM - Foram concluídas beu um aporte de R$ 2,1 mi- também obras de requalifica- lhões e faz parte do primeiro ção e urbanização realizadas lote do Projeto Recons- através do Fundo Estadual de trução, que prevê a constru- Apoio ao Desenvolvimento ção de 13 unidades estaduais Municipal (FEM). Com in- e municipais em oito cidades vestimentos na ordem de da região. Na ocasião, o R$ 2 milhões, a intervenção chefe do Executivo estadual contemplou a pavimentação defendeu e reafirmou o com- em diversas ruas da Vila do promisso do Governo com a Cruzeiro e de outras áreas da promoção da educação de cidade, além da construção qualidade e integrada. -

Pluviosidade Média Anual - 2011
ANUÁRIO ESTATÍSTICO DE PERNAMBUCO - 2015 Pluviosidade média anual - 2011 41°0'0"W 40°0'0"W 39°0'0"W 38°0'0"W 37°0'0"W 36°0'0"W 35°0'0"W Brejinho ! CEARÁ ! ! PARAÍBA Camutanga Santa Terezinha Itapetim ! ! ! Itambé ! Ferreiros ! São José do Egito ! Exu Macaparana Tabira ! Timbaúba ! ! Solidão ! São Vicent!e Aliança ! ! ! Araripina Ipubi ! ! Ferrer Condado Goiana ! Moreilândia Tuparetama Vicência! ! Afogados ! ! ! Nazaré Itaquitinga ! ! da Ingazeira Ingazeira Vertente do Orobó Machados ! Trindade Santa Cruz da Quixaba ! da Mata Itapissuma ! Bodocó Granito ! Lério ! Buenos Aires ! ! Cedro Baixa Verde ! Casinhas Araçoiaba ! Ilha de ! Santa Maria Bom Jardim Tracunhaém ! ! ! Carpina ! Itamaracá ! Carnaíba do Cambucá ! ! ! Lagoa do ! ! ! Iguaraci ! João Alfredo ! ! Igarassu Flores Taquaritinga ! ! Carro Ouricuri ! São José do Belmonte Triunfo Santa Cruz do Vertentes Surubim Lagoa do do Norte ! ! ! Abreu e Lima ! ! Capibaribe S!algadinho Limoeiro Itaenga PIAUÍ Serrita ! ! !Frei ! Paudalho ! S Calumbi ! ! Paulista S " ! Miguelinho Feira Nova Chã de Alegria " 0 Verdejante ! Camaragibe 0 ' To!ritama ! ! ! ! ! Olin!da ' 0 Jataúba ! 0 ° Serra Talhada Passira Glória do Goitá São Lourenço ° 8 Riacho Cumaru 8 da Mata ! ! Sertânia ! das Recife Parnamirim ! ! ! Brejo da Madre Almas Pombos ! Salgueiro Custódia ! ! ! de Deus ! Moreno ! ! Terra Nova Mirandiba Vitória de Jaboatão dos ! Caruaru Gravatá Bezerros Santo Antão Guararapes Santa Filomena ! ! Chã Grande ! Betânia Poção ! ! ! Sairé Cabo de Santo Agostinho Santa Cruz Belo Jardim ! ! ! o ! ! ! ! Primav!era -

Crimes Violentos Letais Intencionais
CRIMES VIOLENTOS LETAIS INTENCIONAIS EVOLUÇÃO ANUAL DOS NÚMEROS DE VÍTIMAS DE CVLI EM PERNAMBUCO POR MUNICÍPIO JANEIRO DE 2004 A DEZEMBRO DE 2020 MUNICÍPIO 2004 2005 2006 2007 2008 2009 2010 2011 2012 2013 2014 2015 2016 2017 2018 2019 2020 ABREU E LIMA 48 52 67 57 63 49 54 45 49 32 44 43 42 71 48 41 36 AFOGADOS DA INGAZEIRA 10 8 10 8 5 7 14 6 7 3 1 5 3 7 2 7 4 AFRANIO 2 1 0 3 2 1 1 2 1 1 1 4 2 3 3 5 0 AGRESTINA 13 11 16 8 18 14 13 18 12 16 13 16 27 18 14 17 9 AGUA PRETA 10 7 8 12 12 7 5 8 6 6 7 15 20 10 11 14 15 AGUAS BELAS 10 13 10 13 7 17 12 14 14 9 8 14 22 19 19 14 15 ALAGOINHA 3 5 6 3 2 2 4 4 5 2 2 1 2 6 6 0 8 ALIANCA 24 29 28 11 17 14 9 14 18 13 14 14 19 15 17 13 11 ALTINHO 6 10 8 16 11 7 3 9 4 3 11 15 10 25 13 12 14 AMARAJI 10 13 21 20 7 15 14 9 10 6 15 4 30 21 17 23 23 ANGELIM 3 1 1 3 3 3 4 3 2 5 4 6 5 4 7 6 4 ARACOIABA 3 4 3 3 6 3 10 6 6 3 8 9 19 11 7 6 12 ARARIPINA 9 26 17 18 23 24 15 30 20 12 19 28 42 35 26 15 21 ARCOVERDE 37 34 32 44 35 22 30 19 29 22 21 23 33 36 25 30 11 BARRA DE GUABIRABA 4 2 2 1 3 3 2 2 5 4 8 10 6 13 11 4 7 BARREIROS 8 18 14 24 17 13 13 17 21 22 39 26 23 30 16 19 24 BELEM DE MARIA 2 4 3 1 4 8 8 3 3 4 5 3 5 4 4 2 10 BELEM DE SAO FRANCISCO 7 4 5 11 16 6 7 5 13 1 11 12 5 5 8 1 1 BELO JARDIM 15 31 27 31 20 19 17 27 21 28 27 31 39 62 37 30 26 BETANIA 2 2 3 5 4 7 3 5 4 1 5 2 2 4 3 3 2 BEZERROS 20 46 57 38 50 30 20 11 25 22 34 44 50 49 33 26 26 BODOCO 6 2 3 2 1 12 4 3 10 12 5 3 6 14 2 2 5 BOM CONSELHO 6 5 10 8 16 15 9 16 9 13 12 15 12 9 15 6 13 BOM JARDIM 12 8 10 11 15 10 8 7 11 6 12 18 13 28 17 6 16 BONITO 7 -

Crescimento Urbano Do Município De Gravatá E Suas Consequências Na Sociedade Local
CRESCIMENTO URBANO DO MUNICÍPIO DE GRAVATÁ E SUAS CONSEQUÊNCIAS NA SOCIEDADE LOCAL Josias Ivanildo Flores de CARVALHO 1 Laryssa de Aragão SOUSA 2 Maurílio Bernardino do Nascimento JÚNIOR 3 1. INTRODUÇÃO O crescimento urbano deve ser visto como um processo que gera consequências na sociedade. Dessa maneira a cidade de Gravatá vem sofrendo nos últimos quinze anos uma grande aceleração no que diz respeito ao seu processo de urbanização. De acordo com Santos (1986) esse crescimento é motivado por causa da industrialização, que se consolidou no Brasil ao longo do século XX nas grandes metrópoles e em cidades de médio porte, onde a população brasileira fez o êxodo rural, em razão da busca de trabalho e de melhores condições de vida. Entretanto esse fenômeno urbanístico em Gravatá é um acontecimento característico da atualidade, hoje as grandes cidades brasileiras estão sofrendo um verdadeiro caos, por conta da falta de planejamento urbano. Sendo assim, uma parcela da população se destaca nesse processo de urbanização em Gravatá, são eles, empresários e a população da classe média alta que buscam tranquilidade e conforto neste município. Uma constatação que distingue essa urbanização é a forma de construção das casas e condomínios de veraneios, que diferentemente das metrópoles que são na vertical, no referido município estudado as construções são totalmente na horizontal, por conta da 1 Graduando na Universidade Federal de Pernambuco- UFPE. Graduação Plena em Geografia (Licenciatura) /3º período. E-mail: [email protected]. 2Graduando na Universidade Federal de Pernambuco- UFPE. Graduação Plena em Geografia (Licenciatura) / 1º período. E-mail: [email protected].