WADA Technical Document – TD2021NA HARMONIZATION of ANALYSIS and REPORTING of 19-NORSTEROIDS RELATED to NANDROLONE 1.0 Introdu
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Hormonal Treatment Strategies Tailored to Non-Binary Transgender Individuals
Journal of Clinical Medicine Review Hormonal Treatment Strategies Tailored to Non-Binary Transgender Individuals Carlotta Cocchetti 1, Jiska Ristori 1, Alessia Romani 1, Mario Maggi 2 and Alessandra Daphne Fisher 1,* 1 Andrology, Women’s Endocrinology and Gender Incongruence Unit, Florence University Hospital, 50139 Florence, Italy; [email protected] (C.C); jiska.ristori@unifi.it (J.R.); [email protected] (A.R.) 2 Department of Experimental, Clinical and Biomedical Sciences, Careggi University Hospital, 50139 Florence, Italy; [email protected]fi.it * Correspondence: fi[email protected] Received: 16 April 2020; Accepted: 18 May 2020; Published: 26 May 2020 Abstract: Introduction: To date no standardized hormonal treatment protocols for non-binary transgender individuals have been described in the literature and there is a lack of data regarding their efficacy and safety. Objectives: To suggest possible treatment strategies for non-binary transgender individuals with non-standardized requests and to emphasize the importance of a personalized clinical approach. Methods: A narrative review of pertinent literature on gender-affirming hormonal treatment in transgender persons was performed using PubMed. Results: New hormonal treatment regimens outside those reported in current guidelines should be considered for non-binary transgender individuals, in order to improve psychological well-being and quality of life. In the present review we suggested the use of hormonal and non-hormonal compounds, which—based on their mechanism of action—could be used in these cases depending on clients’ requests. Conclusion: Requests for an individualized hormonal treatment in non-binary transgender individuals represent a future challenge for professionals managing transgender health care. For each case, clinicians should balance the benefits and risks of a personalized non-standardized treatment, actively involving the person in decisions regarding hormonal treatment. -

Us Anti-Doping Agency
2019U.S. ANTI-DOPING AGENCY WALLET CARDEXAMPLES OF PROHIBITED AND PERMITTED SUBSTANCES AND METHODS Effective Jan. 1 – Dec. 31, 2019 CATEGORIES OF SUBSTANCES PROHIBITED AT ALL TIMES (IN AND OUT-OF-COMPETITION) • Non-Approved Substances: investigational drugs and pharmaceuticals with no approval by a governmental regulatory health authority for human therapeutic use. • Anabolic Agents: androstenediol, androstenedione, bolasterone, boldenone, clenbuterol, danazol, desoxymethyltestosterone (madol), dehydrochlormethyltestosterone (DHCMT), Prasterone (dehydroepiandrosterone, DHEA , Intrarosa) and its prohormones, drostanolone, epitestosterone, methasterone, methyl-1-testosterone, methyltestosterone (Covaryx, EEMT, Est Estrogens-methyltest DS, Methitest), nandrolone, oxandrolone, prostanozol, Selective Androgen Receptor Modulators (enobosarm, (ostarine, MK-2866), andarine, LGD-4033, RAD-140). stanozolol, testosterone and its metabolites or isomers (Androgel), THG, tibolone, trenbolone, zeranol, zilpaterol, and similar substances. • Beta-2 Agonists: All selective and non-selective beta-2 agonists, including all optical isomers, are prohibited. Most inhaled beta-2 agonists are prohibited, including arformoterol (Brovana), fenoterol, higenamine (norcoclaurine, Tinospora crispa), indacaterol (Arcapta), levalbuterol (Xopenex), metaproternol (Alupent), orciprenaline, olodaterol (Striverdi), pirbuterol (Maxair), terbutaline (Brethaire), vilanterol (Breo). The only exceptions are albuterol, formoterol, and salmeterol by a metered-dose inhaler when used -
Guidelines for the Management of Heavy Menstrual Bleeding
i GUIDELINES FOR THE MANAGEMENT OF HEAVY MENSTRUAL BLEEDING Prepared by a Working Party on behalf of the National Health Committee ii MAY 1998 Women reporting with heavy menstrual bleeding 50% of women have menstrual blood loss Full menstrual history ● Examination ● Full blood count note1 Yes Prolonged irregular cycles No Refer Yes Abnormal exam specialist uterine size >12wks note 2 No mild or severe anaemic moderate treat < 80 g/l (80-115g/l) anaemia No Assess risk of endometrial hyperplasia low Offer medical therapy ● risk Unexplaine bodyweight 90kg heavy menstrual ● note5 note 6 age 45 years <2% bleeding ● other risk factors have 90% of women note 3 ● levonorgestrel endometrial >8% have hyperplasia intrauterine system ● tranexamic acid ● Assess endometrium nonsteroidal ● transvaginal ultrasound antiinflammatory agents ● (TVS) norethisterone long course or normal ● oc pill endometrium ● ● endometrial biopsy if danazol if one medical therapyfails endometrium 12mm others can be used note 7 or if TVS not available note 4 Treatment Hyperplastic endometrium success? or carcinoma No Yes Refer to specialist for hysteroscopic evaluation Continue Refer specialist me d i c a l for surgery therapy note8 note9 iii note 1 O In women <20 years old pelvic examination is unlikely to contribute to management of heavy bleeding (C) and the likelihood of pathology is small (C) O Increased likelihood (70%) of heavy menstrual blood loss >80mls/cycle if Hb <120g/l (A) O Consider pictorial blood loss assessment charts (appendix 6.5) for women with normal -

(12) Patent Application Publication (10) Pub. No.: US 2014/0296.191 A1 PATEL Et Al
US 20140296.191A1 (19) United States (12) Patent Application Publication (10) Pub. No.: US 2014/0296.191 A1 PATEL et al. (43) Pub. Date: Oct. 2, 2014 (54) COMPOSITIONS OF PHARMACEUTICAL (52) U.S. Cl. ACTIVES CONTAINING DETHYLENE CPC ............... A61K 47/10 (2013.01); A61 K9/0019 GLYCOL MONOETHYLETHER OR OTHER (2013.01); A61 K9/0048 (2013.01); A61 K ALKYL DERVATIVES 45/06 (2013.01) USPC ........... 514/167: 514/177; 514/178: 514/450; (71) Applicant: THEMIS MEDICARE LIMITED, 514/334: 514/226.5: 514/449; 514/338; Mumbai (IN) 514/256; 514/570; 514/179; 514/174: 514/533; (72) Inventors: Dinesh Shantilal PATEL, Mumbai (IN); 514/629; 514/619 Sachin Dinesh PATEL, Mumbai (IN); Shashikant Prabhudas KURANI, Mumbai (IN); Madhavlal Govindlal (57) ABSTRACT PATEL, Mumbai (IN) (73) Assignee: THEMIS MEDICARE LIMITED, The present invention relates to pharmaceutical compositions Mumbai (IN) of various pharmaceutical actives, especially lyophilic and hydrophilic actives containing Diethylene glycol monoethyl (21) Appl. No.: 14/242,973 ether or other alkyl derivatives thereofas a primary vehicle and/or to pharmaceutical compositions utilizing Diethylene (22) Filed: Apr. 2, 2014 glycol monoethyl ether or other alkyl derivatives thereofas a primary vehicle or as a solvent system in preparation of Such (30) Foreign Application Priority Data pharmaceutical compositions. The pharmaceutical composi Apr. 2, 2013 (IN) ......................... 1287/MUMA2013 tions of the present invention are safe, non-toxic, exhibits enhanced physical stability compared to conventional formu Publication Classification lations containing such pharmaceutical actives and are Suit able for use as injectables for intravenous and intramuscular (51) Int. Cl. administration, as well as for use as a preformed solution/ A647/ (2006.01) liquid for filling in and preparation of capsules, tablets, nasal A6 IK 45/06 (2006.01) sprays, gargles, dermal applications, gels, topicals, liquid oral A6 IK9/00 (2006.01) dosage forms and other dosage forms. -

Steroid Abuse by School Age Children
epartment .D of .S Ju U s t ic U.S. Department of Justice e . n o i Drug Enforcement Administration t a r t is D in Office of Diversion Control r m ug d E t A nforcemen www.dea.gov www.DEAdiversion.usdoj.gov epartment .D of .S Ju U s t ic e . n o i t a r t is D in r m ug d E t A nforcemen Office of Diversion Control www.dea.gov STEROID ABUSE BY SCHOOL AGE CHILDREN nce viewed as a problem strictly associated with body builders, Ofitness “buffs,” and professional athletes, abuse of anabolic steroids by school age children has significantly increased over the past decade. The National Institute on Drug Abuse (NIDA) estimates that more than a half million 8th and 10th grade students are now using these dangerous drugs, and increasing numbers of high school seniors do not believe steroids are risky. Students are acquiring and taking anabolic steroids without any knowledge of the dangers associated with steroid abuse. The short- term adverse physical effects of anabolic steroid abuse are fairly well known. However, the long-term adverse physical effects of anabolic steroid abuse have not been studied, and as such, are not known. In addition, this type of abuse may result in harmful side-effects as well as serious injury and death. The abuser in most cases is unaware of these hidden dangers. Presented as a public service by: This guide will help you understand why steroids are being misused, Drug Enforcement Administration and how you can provide counseling and implement procedures to Office of Diversion Control educate our youth about the dangers of these drugs. -
NORETHISTERONE This Document Should Be Read in Conjunction with This DISCLAIMER
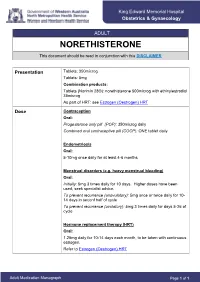
King Edward Memorial Hospital Obstetrics & Gynaecology ADULT NORETHISTERONE This document should be read in conjunction with this DISCLAIMER Presentation Tablets: 350microg Tablets: 5mg Combination products: Tablets (Norimin 28®): norethisterone 500microg with ethinylestradiol 35microg As part of HRT: see Estrogen (Oestrogen) HRT Dose Contraception Oral: Progesterone only pill (POP): 350microg daily Combined oral contraceptive pill (COCP): ONE tablet daily Endometriosis Oral: 5-10mg once daily for at least 4-6 months Menstrual disorders (e.g. heavy menstrual bleeding) Oral: Initially: 5mg 3 times daily for 10 days. Higher doses have been used; seek specialist advice. To prevent recurrence (anovulatory): 5mg once or twice daily for 10- 14 days in seconf half of cycle To prevent recurrence (ovulatory): 5mg 3 times daily for days 5-26 of cycle Hormone replacement therapy (HRT) Oral: 1.25mg daily for 10-14 days each month, to be taken with continuous estrogen. Refer to Estrogen (Oestrogen) HRT Adult Medication Monograph Page 1 of 1 Norethisterone – Adult Administration Oral To be taken at the same time each day (or within 3 hours of the usual dose time). For Contraception: Start 4 weeks after the birth of baby (increased risk of abnormal vaginal bleeding if started earlier) Pregnancy 1st Trimester: Contraindicated 2nd Trimester: Contraindicated 3rd Trimester: Contraindicated Breastfeeding Considered safe to use. Progestogens are the preferred hormonal contraceptives as they do not inhibit lactation. Clinical Guidelines Estrogen (Oestrogen) HRT and Policies Progesterone Only Pill Contraception: Post Partum Gynaecology (Non-Oncological) Australian Medicines Handbook. Norethisterone. In: Australian References Medicines Handbook [Internet]. Adelaide (South Australia): Australian Medicines Handbook; 2017 [cited 2017 Apr 12]. -

Nur-Isterate Injection
SELECT THE REQUIRED INFORMATION PROFESSIONAL INFORMATION PATIENT INFORMATION LEAFLET SCHEDULING STATUS: S4 PROPRIETARY NAME AND DOSAGE FORM: NUR-ISTERATE Oily solution for intramuscular injection COMPOSITION: 1 ml contains norethisterone enantate (17-ethinyl-17-heptanoyloxy-4-estrene-3-one) 200 mg. Other ingredients are: benzyl benzoate, castor oil for injection. PHARMACOLOGICAL CLASSIFICATION: A. 21.8.2 Progesterones without estrogens. PHARMACOLOGICAL ACTION: Pharmacodynamic properties: Protection against conception is based primarily upon an alteration of the cervical mucous. This alteration is present for the whole of the duration of action and prevents the ascent of the sperm into the uterine cavity. Radioimmunological studies have shown that, during the first 5 to 7 weeks after injection, ovulation is suppressed as a result of the high plasma level of norethisterone. In addition, NUR- ISTERATE causes morphological changes in the endometrium which have the effect of rendering nidation of a fertilised egg difficult. Pharmacokinetic properties: Norethisterone enantate was completely absorbed after intramuscular injection. The ester was eventually completely hydrolysed to its pharmacologically active compound norethisterone once it was released from the depot. Maximum levels of norethisterone were measured at about 3 to 10 days after IM administration. They amounted on average to 13.4 5.4 ng/ml and 12.2 2.7 ng/ml about 7 days (median) after IM administration of 200 mg norethisterone enantate in 2 ml and 1 ml oily solution, respectively. Plasma levels of norethisterone declined in two disposition phases with half-lives of 4 to 5 days and 15 to 20 days, respectively, which were due to a biphasic release of norethisterone enantate from the depot. -

(12) United States Patent (10) Patent No.: US 6,284,263 B1 Place (45) Date of Patent: Sep
USOO6284263B1 (12) United States Patent (10) Patent No.: US 6,284,263 B1 Place (45) Date of Patent: Sep. 4, 2001 (54) BUCCAL DRUG ADMINISTRATION IN THE 4,755,386 7/1988 Hsiao et al. TREATMENT OF FEMALE SEXUAL 4,764,378 8/1988 Keith et al.. DYSFUNCTION 4,877,774 10/1989 Pitha et al.. 5,135,752 8/1992 Snipes. 5,190,967 3/1993 Riley. (76) Inventor: Virgil A. Place, P.O. Box 44555-10 5,346,701 9/1994 Heiber et al. Ala Kahua, Kawaihae, HI (US) 96743 5,516,523 5/1996 Heiber et al. 5,543,154 8/1996 Rork et al. ........................ 424/133.1 (*) Notice: Subject to any disclaimer, the term of this 5,639,743 6/1997 Kaswan et al. patent is extended or adjusted under 35 6,180,682 1/2001 Place. U.S.C. 154(b) by 0 days. * cited by examiner (21) Appl. No.: 09/626,772 Primary Examiner Thurman K. Page ASSistant Examiner-Rachel M. Bennett (22) Filed: Jul. 27, 2000 (74) Attorney, Agent, or Firm-Dianne E. Reed; Reed & Related U.S. Application Data ASSciates (62) Division of application No. 09/237,713, filed on Jan. 26, (57) ABSTRACT 1999, now Pat. No. 6,117,446. A buccal dosage unit is provided for administering a com (51) Int. Cl. ............................. A61F 13/02; A61 K9/20; bination of Steroidal active agents to a female individual. A61K 47/30 The novel buccal drug delivery Systems may be used in (52) U.S. Cl. .......................... 424/435; 424/434; 424/464; female hormone replacement therapy, in female 514/772.3 contraception, to treat female Sexual dysfunction, and to treat or prevent a variety of conditions and disorders which (58) Field of Search .................................... -

Pharmaceutical Appendix to the Tariff Schedule 2
Harmonized Tariff Schedule of the United States (2007) (Rev. 2) Annotated for Statistical Reporting Purposes PHARMACEUTICAL APPENDIX TO THE HARMONIZED TARIFF SCHEDULE Harmonized Tariff Schedule of the United States (2007) (Rev. 2) Annotated for Statistical Reporting Purposes PHARMACEUTICAL APPENDIX TO THE TARIFF SCHEDULE 2 Table 1. This table enumerates products described by International Non-proprietary Names (INN) which shall be entered free of duty under general note 13 to the tariff schedule. The Chemical Abstracts Service (CAS) registry numbers also set forth in this table are included to assist in the identification of the products concerned. For purposes of the tariff schedule, any references to a product enumerated in this table includes such product by whatever name known. ABACAVIR 136470-78-5 ACIDUM LIDADRONICUM 63132-38-7 ABAFUNGIN 129639-79-8 ACIDUM SALCAPROZICUM 183990-46-7 ABAMECTIN 65195-55-3 ACIDUM SALCLOBUZICUM 387825-03-8 ABANOQUIL 90402-40-7 ACIFRAN 72420-38-3 ABAPERIDONUM 183849-43-6 ACIPIMOX 51037-30-0 ABARELIX 183552-38-7 ACITAZANOLAST 114607-46-4 ABATACEPTUM 332348-12-6 ACITEMATE 101197-99-3 ABCIXIMAB 143653-53-6 ACITRETIN 55079-83-9 ABECARNIL 111841-85-1 ACIVICIN 42228-92-2 ABETIMUSUM 167362-48-3 ACLANTATE 39633-62-0 ABIRATERONE 154229-19-3 ACLARUBICIN 57576-44-0 ABITESARTAN 137882-98-5 ACLATONIUM NAPADISILATE 55077-30-0 ABLUKAST 96566-25-5 ACODAZOLE 79152-85-5 ABRINEURINUM 178535-93-8 ACOLBIFENUM 182167-02-8 ABUNIDAZOLE 91017-58-2 ACONIAZIDE 13410-86-1 ACADESINE 2627-69-2 ACOTIAMIDUM 185106-16-5 ACAMPROSATE 77337-76-9 -

Polycystic Ovarian Syndrome
Polycystic Ovarian Syndrome What we understand and how we can help October 2017 Presentation Title | 27 January 2014 History Stein and Leventhal 1935 Stein IF, Leventhal ML. Amenorrhoea associated with bilateral polycystic ovaries. Am J Obstet Gynaecol 1935; 29:181-191 Presentation Title | 7 January, 2019 Presentation Title | 7 January, 2019 Diagnosis Rotterdam criteria – Two of the three criteria 1. PCOS on USS 2. Oligo or anovulation (less than 6 periods each year) 3. Hyperandrogenism Presentation Title | 7 January, 2019 Presentation Title | 7 January, 2019 Diagnosis – ovarian morphology PCO ultrasound appearance in 22% of normal population PCOS is present in • 7% of women • 32% of women with amenorrhoea • 87% of women with hirsuitism/ acne • 73% of women with anovulatory infertility Presentation Title | 7 January, 2019 Diagnostic tests The biochemical tests are to identify hyperandrogenism… Testosterone Can be measured at any time during the cycle. Consider testosterone secreting tumour if rapid virilisation. Consider High total testosterone or normal total testosterone with low SHBG and high bio-testosterone (measure the free androgen index) GTT All PCOS women who are obese and all women PCOS women over the age of 40. LH and FSH AMH Ovarian reserve and number of antral follicles. – may be raised in PCOS, however not currently used in diagnsois. Presentation Title | 7 January, 2019 Presentation Title | 7 January, 2019 Managing Symptoms Presentation Title | 7 January, 2019 Obesity Supportive strategies for weight loss and diet. Consider Metformin Bariatric surgery Presentation Title | 7 January, 2019 Hirsuitism and Acne Weight loss Cosmetic methods Oral contraceptive pill consider Yasmin as it has an antiandrogenic action. -

The Combined Cardiac Effect of the Anabolic Steroid, Nandrolone And
ù1. v -¿. rlc) 77.- *n*hi.rnool oowol,ù*o ffi"/fu -lo *rn*(o fii'o fio¿o¿¿, /v&"ùún lonno **al cooaiæe';¿vfl"- oã. Benjamin D. Phillis, B.Sc. (Hons) Phatmacology Depattment of Clinical & Experimental Pharmacology Ftome Rd. , Medical School Noth Adelaide Univetsity ADEIAIDE SA 5OOO û.)r.'-*hr/7enveltîù Foremost, I would like to thank my two supervisors for the direction that they have given this ptojecr. To Rod, for his unfailing troubleshooting abiJity and to Jenny fot her advice and ability to add scientific rigour' Many thanks to Michael Adams for his technical assistance and especially fot performing the surgery for the ischaemia-reperfusion projects and for his willingness to work late nights and public holidays. Lastly I would like to thank my v¡ife for her extreme patience during the tumult of the last 5 years. Her love, suppoït, patience and undetstanding have been invaluable in this endeavout. Beniamin D. Phillis Octobet,2005 ADE,I-AIDE ii T*(¿t of Ao,t",tù DECI.ARATION I ACKNOWLEDGEMENTS il TABLE OF CONTENTS UI ABBREVIATIONS x ABSTRACT )ilr CÉIAPTER t-l Inttoduction 1-1 1.1 Background 1,-1, 1.2What ate anabolic stetoids? 7-1 1,3 General pharmacology of Anabolic steroids t-2 '1,-2 1.3.1 Genomic effects of anabolic steroids 1.3.2 Non-genomic effects of anabolic steroids 1-3 1.4 Clinical use of AS 1.-4 1.5 Patterns of AS abuse 1.-4 1.5.1 Steroid abuse by athletes 1.-+ 1.5.2 Stetoid abuse by sedentary teenagers r-6 1.5.3 Prevalence of abuse 1-6 1.5.4 Abuse ptevalence in Australia 1.-9 1.6 Cardiotoxicity of anabolic steroids r-9 1.6.1 Reduced cotonary flow 1.-1.1, 1,.6.2 Dtect myocatdial eff ects 1-1 5 1.6.3 Hypertension 1-21 1.7 Difficulties associated with anabolic steroid research 1.-24 1-25 1.8 The polydrug abuse Phenomenon 1.9 The pharmacology of cocaine 1-26 1.10 Pteparations 1-28 1-29 1.11 Metabolism lll 1-30 1. -

Study on Sperm Suppression Using Norethisterone Enanthate and Testosterone Undecanoate
Study on sperm suppression using Norethisterone enanthate and testosterone undecanoate Objectives Overall goal: and The study was designed to address the following primary objectives: Background 1. The rate of suppression of spermatogenesis induced by a regimen of NET-EN and TU administered every 8 weeks for up to 4 injection visits; and 2. The level of contraceptive protection provided by the continued administration of NET-EN and TU every 8 weeks for an efficacy period of up to 56 weeks. Background: The study was designed to evaluate whether the combination of a progestin, norethisterone enantate (NET-EN), and an androgen, testosterone undecanoate (TU), represents a safe and effective method of male fertility regulation. The study had 3 phases. The suppression phase was to initiate a status of decreased sperm count and activity to a level which would be considered as contraceptive. When this was reached it was sustained with subsequent injections in the efficacy phase, which would end after 56 weeks, or if a pregnancy occurs. After these, the participant was then placed in the recovery phase, and was observed until normal sperm counts and activity returns to normal. 487 participants were screened for eligibility, of which 167 were excluded. The remaining 320 were enrolled into the study, into the suppression phase. A total of 274 completed the suppression phase. Of these 8 discontinued before transitioning to the Efficacy phase, and were moved to recovery phase. A total of 266 transitioned to the efficacy phase, among which 111 completed 56 weeks follow up or until a pregnancy occurred. The remaining 155 were discontinued, either because of the stopping of the study by the sponsor (96), death (1, unrelated to the study), or for other reasons (58).