North Dakota Medicaid Expansion Program Member Handbook Welcome
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Sanford Directory
HealthPartners® Sanford Basic (Cost) HealthPartners® Sanford Active (Cost) HealthPartners® Sanford Vital (Cost) HealthPartners® Sanford Ultimate (Cost) This directory addenda provides a list of HealthPartners® Sanford network providers and pharmacies. This directory is current as of December 2020. Some network providers may have been added or removed from our network after this directory was printed. We do not guarantee that each network provider is still accepting new members. 2020 NORTH DAKOTA/SOUTH DAKOTA PROVIDER DIRECTORY - ADDENDA H2462_119077_C IR 11/2019 This document is a list of changes to the HealthPartners® Sanford network providers. Use this list to find the network providers that have had changes. Providers are organized first by the network change. The network change categories are New to the Network, No longer in the Network, Accepting New Patients, Address Changes and Phone Number Changes. After category, it is organized by provider type, then alphabetically by facility name. If you have any questions, please call Member Services at 800-233-9645 (TTY 711). Facility Name Address City, State, Zip Phone Number NEW TO THE NETWORK Primary care physicians and specialists – New to the Network Accelerate Therapy 1908 W 42nd St Ste B Sioux Falls, SD 57105 (605) 212-3446 Advanced Physical 1000 Tacoma Ave Ste Bismarck, ND 58504 (701) 751-3001 Therapy 500 Advanced Physical 4535 Northern Sky Dr Bismarck, ND 58503 (701) 354-1200 Therapy Ste 2 Advanced Physical 112 W Broadway Ave Steele, ND 58482 (701) 475-2911 Therapy Anderson-Smith -

Important Information for Providers About Sanford Health Plan
PO Box 91110 Sioux Falls, SD 57109-1110 Important Information for Phone: (877) 305-5463 Fax: (605) 328-6811 Providers about Sanford Health Plan TTY: (877) 652-1844 sanfordhealthplan.com Sanford Health Plan (Plan) asks you to take some time and review this information. The following annual notices are required to keep you informed of Sanford Health Plan operations and outcomes. Where can I find important plan information? If you have any questions…. Provider Relations Phone: (605) 328-6877 or toll free at (800) 601-5086 Email: [email protected] Care Management Phone: (888) 315-0884 Email: [email protected] Utilization Management Phone: (800) 805-7938 | TTY/TDD: (877) 652-1844 (toll-free) Fax: (605) 328-6813 NDPERS Members: Phone: (888) 315-0885 | TTY/TDD: (877) 652-1844 (toll-free) Fax: (701) 234-4547 North Dakota Medicaid Expansion Phone: (855) 276-7214 Members: Pharmacy Management Phone: (855) 305-5062 Fax: (701) 234-4568 NDPERS Members: Phone: (877) 658-9194 North Dakota Medicaid Expansion Phone: (855) 263-3547 Members: Compliance / Privacy Email: [email protected] The Utilization and Pharmacy Management Departments are available between the business hours of 8 a.m. to 5 p.m., CT, Monday through Friday (excluding holidays). For North Dakota Public Employees Retirement System (NDPERS), the Utilization and Pharmacy Management Departments are available between the business hours of 8 a.m. to 5:30 p.m. CT, Monday through Friday (excluding holidays). After business hours, you may leave a confidential -

Behavioral Health Quick Reference Please Call an In-Network Provider List Below for Behavioral Health Needs Assessment Services
Iowa Behavioral Health Quick Reference Please call an In-Network provider list below for behavioral health needs assessment services. LOCATION PHONE All Things New Therapy Services Inc 111 Arizona Ave NW Orange City, IA 51041 (712) 737-9444 Jeremy Koerselman, LISW Rachel Valentine, LMHC Associates for Psychiatric Services, PC 600 4th St Ste 501 Sioux City, IA 51101 (712) 234-0220 Beth Harms, LISW Patricia Whalen, LISW Collette McCullough, ARNP Philip Muller, DO Glenda DenHerder, ARNP Susan Richards, LISW Jeannie Franklin, ARNP Associates for Psychological & Therapy Services 1106 4th St Ste 205 Sioux City, IA 51101 (712) 252-1473 Aaron Baker, LMHC Melissa Schuldt, LMSW Michael Baker, PhD Avera Medical Group Spencer A Department of Spencer 116 E 11th St Ste 101 Spencer, IA 51301 (712) 264-3500 Hugh Starks, MD Kimberly Whisenant, ARNP Behavior Care Specialists, Inc. 745 10th St Ste C Rock Valley, IA 51247 (712) 454-3484 Tracy Stephens, BCBA,PhD Bethany Christian Services of the Heartland 123 Albany Ave SE Orange City, IA 51041 (712) 737-4831 Rachel Valentine, LMHC Bethesda Christian Counseling Midwest, Inc. 400 Central Ave NW Ste 300 Orange City, IA 51041 (712) 737-2635 Deon Wynia, LMHC,MA Stephanie Adams, LISW Mandi Dolieslager, LMSW,MSW William Fuller, MD Melody Becker Pullman, LMHC,MS William Huisken, LISW,MSW Sanford Health Plan Participating Providers as of June 8, 2020 1 Iowa Behavioral Health Quick Reference Please call an In-Network provider list below for behavioral health needs assessment services. LOCATION PHONE Catholic Charities -
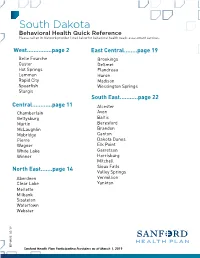
South Dakota Behavioral Health Quick Reference Please Call an In-Network Provider Listed Below for Behavioral Health Needs Assessment Services
South Dakota Behavioral Health Quick Reference Please call an In-Network provider listed below for behavioral health needs assessment services. West...............page 2 East Central........page 19 Belle Fourche Brookings Custer DeSmet Hot Springs Flandreau Lemmon Huron Rapid City Madison Spearfish Wessington Springs Sturgis South East...........page 22 Central............page 11 Alcester Chamberlain Avon Gettysburg Baltic Martin Beresford McLaughlin Brandon Mobridge Canton Pierre Dakota Dunes Wagner Elk Point White Lake Garretson Winner Harrisburg Mitchell Sioux Falls North East.......page 14 Valley Springs Aberdeen Vermillion Clear Lake Yankton Mellette Milbank Sissteton Watertown Webster 9 /1 3 HP-0985 0 Sanford Health Plan Participating Providers as of March 1, 2019 South Dakota - West Behavioral Health Quick Reference Please call an In-Network provider listed below for behavioral health needs assessment services. Abourezk Counseling Services 2020 W Omaha St Rapid City, SD 57702 Phone: (605) 863-2881 Illyani Abourezk, CAC,LLPC-MH,MS,QMHP Ardith Sand, MSW, LCSW-PIP 5202 Pinedale Circle Rapid City, SD 57702 Phone: (605) 391-3456 Ardith Sand, LCSW-PIP,MSW Awareness Counseling LLC 809 South St Ste 201 Rapid City, SD 57701 Phone: (605) 391-3482 Pamela Barickman, LPC-MH,MS,QMHP,RN Bach Counseling Services LLC 2218 Jackson Blvd Ste 13 Rapid City, SD 57702 Phone: (605) 431-4106 Mahala Bach, LPC,NCC,QMHP Behavior Care Specialists, Inc. 3820 Jackson Blvd Ste 2 Rapid City, SD 57702 Phone: (605) 791-3373 Tracy Stephens, BCBA,PhD Behavior Management -

North Dakota HEALTH INSURANCE by the NUMBERS
North Dakota HEALTH INSURANCE BY THE NUMBERS ACCESS TO INSURANCE COVERED LIVES Large Group1A 149,111 Small Group1A 60,381 Individual1A 47,190 HSA/HDHP2B 19,350 Medigap3C 52,163 Medicare Advantage4 3,659 Medicaid5D 20,334 0 25,000 50,000 75,000 100,000 125,000 150,000 175,000 200,000 Health Insurance Employment Health Insurance Coverage in North Dakota of North Dakota Residents8G 2% EMPLOYEES Health Plan Employees6 3,759 8% Insurance-Related Employees7 2,156 13% PAYROLL 67% Health Plan Employees6E Not Reported 11% Insurance-Related Employees7F $114,720,000 AVERAGE WAGE Health Plan Employees6E Not Reported Private Uninsured Medicaid Other Insurance-Related Employees7F $53,210 Medicare Data compiled by America’s Health Insurance Plans (AHIP), Center for Policy and Research, March 2019. NORTH DAKOTA Largest Health Plans by Number of Covered LivesH Blue Cross and Sanford Health 9I Aetna Blue Shield of Medica US Life Commercial Plan North Dakota Blue Cross and American 10 Aetna Blue Shield of Mutual Of Omaha UnitedHealthcare Medigap Republic North Dakota Medicare Great Plains Health Care 11 Aetna Medicare Service Corporation Humana UnitedHealthcare Advantage Advantage (HCSC) Medicaid12 Sanford Health Plan State Premium Tax Collected13J $63,558,000 Sources All data sources, labeled 1 - 13, are referenced in detail on the “Sources” page at the end of the full report, or at this link: http://www.ahip.org/2019-State-Data Notes A. Access to Insurance – Large Group, Small Group and Individual Covered Lives The U.S. Census Bureau does not report data for those states having a limited number Large group covered lives were calculated as domestic comprehensive health coverage of employers in order to maintain anonymity. -

2018 Sanford Provider Directory | Healthpartners
HealthPartners® Sanford Basic (Cost) HealthPartners® Sanford Active (Cost) HealthPartners® Sanford Vital (Cost) HealthPartners® Sanford Ultimate (Cost) 2018 NORTH DAKOTA/SOUTH DAKOTA PROVIDER DIRECTORY - ADDENDA This directory addenda provides a list of HealthPartners® Sanford network providers and pharmacies. This directory is current as of December 2018. Some network providers may have been added or removed from our network after this directory was printed. We do not guarantee that each network provider is still accepting new members. H2462_107343 NM 11/2017 Sanford Directory Addenda This document is a list of changes to the HealthPartners® Sanford network providers. Use this list to find the network providers that have had changes. Providers are organized first by the network change. The network change categories are New to the Network, No longer in the Network, Address Changes and Phone Number Changes. After category, it is organized by provider type, then alphabetically by facility name. If you have any questions, please call Member Services at 800-233-9645 (TTY 711). Facility Name Address City, State, Zip Phone Number NEW TO THE NETWORK Primary care physicians and specialists – New to the Network Caring Edge OP LLC 1810 S Dorothy Ave Sioux Falls, SD 57106 (605) 356-8888 Caring Edge OP, LLC 3124 Colorado Ln Bismarck, ND 58503- (701) 751-5325 5447 Caring Edge OP, LLC 3406 Dominion St Bismarck, ND 58503- (701) 258-7489 5577 Caring Edge OP, LLC 4420 37th Ave S Fargo, ND 58104 (701) 365-4771 Davis Independent OBGYN Care 414 W 18th St -

Susan Berry, Director, Sanford Telemedicine, Enterprise Director of Telehealth Services, Sanford Health
BIOS Susan Berry, Director, Sanford Telemedicine, Enterprise Director of Telehealth Services, Sanford Health. In her role as Telehealth Director, Susan has responsibility for all telehealth activities for Sanford Health. She has 25 years of experience in various roles in the healthcare IT field. Susan started her career in cardiovascular services for a tertiary medical center. From there she transitioned into healthcare IT and has held roles in product development, education and training, Six Sigma and Global Product Management for GE Healthcare IT, FUJIFILM Medical Systems and now Sanford Health. Susan is a member of the American Telemedicine Association (ATA), Center for Telehealth and e-Health Law (CTeL) and sits on the Great Plains Telehealth Resource and Assistance Center Program Advisory Council (gpTRAC PAC). Susan holds a MBA degree from Colorado Technical University, a Bachelor’s degree from the University of Sioux Falls and is a registered Cardiovascular Invasive Specialist. Susan is a native of South Dakota. She enjoys spending time with family and friends at her lake cabin, reading and cooking. She currently resides in Sioux Falls, SD with her husband Christopher. Jeffrey Leichter Ph.D., L.P., born and raised in Long Beach, CA., received an undergraduate degree in biological sciences from the University of California, Irvine and a doctorate in clinical psychology from Alliant University in Los Angeles. He completed a two-year fellowship in health psychology at Michigan State University. He was director of behavioral medicine at National Rehabilitation Hospital in Washington D.C. before joining Sanford Health in 1990. He has worked for the past 27 years in a rural primary care clinic in Detroit Lakes, Minnesota where he has collaborated closely in integrated practice with family medicine, internal medicine, and OB-GYN physicians and advanced practice providers. -

Sanford Health
Adult Immunization (AI) Best Practices Learning Collaborative, Group 2: Case Study Sanford Health Sioux Falls, SD Organizational Profile Acronym Legend Sanford Health, one of the largest health systems in the United AI Collaborative: AMGA’s Adult Immunization Best States, is dedicated to the integrated delivery of health care, Practices Collaborative genomic medicine, senior care and services, global clinics, CDC: Centers for Disease Control and Prevention research and affordable insurance. Headquartered in Sioux EMR: Electronic medical record Falls, South Dakota, the organization includes 44 hospitals, HM: Health Maintenance 1,400 physicians and more than 200 Good Samaritan PCV13: Pneumococcal Conjugate Vaccine Society senior care locations in 26 states and nine countries. PPSV23: Pneumococcal Polysaccharide Vaccine Nearly $1 billion in gifts from philanthropist Denny Sanford QA: Quality assurance have transformed how Sanford Health improves the human condition. the two types of pneumococcal vaccines, and the adult Executive Summary vaccination schedule. Staff were also educated on the Every year, many people are affected by influenza and transition to a “no missed opportunities” culture. A “no missed pneumococcal disease. Although vaccines are available opportunities” culture means that vaccines are administered at to prevent these diseases, many individuals have not been all visit types—not just complete physical exams. The second vaccinated and are left unprotected. Sanford Health has been intervention utilized was distribution of reminder letters to working hard to make improvements in vaccination rates patients overdue for pneumococcal vaccination. Lastly, an for all patients. AMGA’s Adult Immunization Best Practices incentive program was instituted to provide compensation Learning Collaborative (AI Collaborative) provided an to the clinic that saw the greatest increase in pneumococcal opportunity to focus on better protecting adult patients. -

DLT Awards - South Dakota
DLT Awards - South Dakota 2012 Grant Awards Avera Health (1) $401,636 South Dakota, Iowa, Minnesota, Nebraska, and Wyoming Areas Served: Bon Homme, Charles Mix, Gregory, Grant, Hutchinson, Kingsbury, Marshall, Moody, Yankton, Emmet, Sioux, Lincoln, Marshall, Holt, and Knox, and Hot Springs Counties Contact: Ms. Rachael Sherard Telephone: (605) 322-4725 Congressional District: Noem, At-Large (SD); Latham, 4th Dist. (IA); King, 5th Dist. (IA); Peterson, 7th Dist. (MN); Smith, 3rd Dist. (NE); and Lummis, At-Large (WY) Rural Development funds will be used to purchase and install telemedicine equipment for 17 participating hospitals, clinics and long term care facilities in a 63-end user telemedicine network that covers the multi-state frontier and rural territory of the Northern Great Plains. As one of two separate proposals by Avera Health, the Avera TeleCare Project provides a range of services with a breadth of scope that matches the size of the service territory, including emergency services, teleradiology, pharmacy services, intensive care, oncology, hepatology, pediatrics, endocrinology, gastroenterology, internal medicine, maternal/fetal medicine, women’s health and many more specialties. Avera McKennan Hospital in Sioux Falls, S.D., provides the medical specialists through its eCare Service lines, while other specialty clinics in Sioux Falls serve as specialist hub sites providing physicians for Avera’s eConsult services. Avera Health (2) $448,053 South Dakota, Iowa, Minnesota, and North Dakota Areas Served: Bon Homme, Brookings, Brule, Charles Mix, Davison, Hand, Hutchinson, Kingsbury, McPherson, Minnehaha and Yankton, Emmet, Dickinson, Osceola, Sioux, Pipestone, Lincoln, Lyon, Bottineau, McIntosh, McKenzie, and Rolette Counties Contact: Ms. Rachael Sherard Telephone: (605) 322-4725 Congressional District: SD: Noem, At-Large (SD); Latham, 4th Dist. -

North Dakota Department of Health ASPEN: Facility Directory (FD)
North Dakota Department of Health ASPEN: Facility Directory (FD) Printed 03/17/2020 Sorted By: City Page 1 of 7 Facility Legal Name ( Facility ID ) Administrator Type Working Name Phone Medicare ID Title Emergency Contact Team Operating Status Address Fax Medicaid ID County Emergency Phone Mgmt Certified/Total Beds City, State, Zip Email Ashley Medical Center (5001A) ERIC HEUPEL HOSP-CAH ASHLEY MEDICAL CENTER (701) 288-3433 351322 01-ACTIVE 612 CENTER AVENUE N (701) 288-3938 1000 MCINTOSH 20/20 ASHLEY, ND 58413 Quentin N. Burdick Memorial Health Care Facility (350063) SHELLY HARRIS HOSP-ACU P H S INDIAN HOSP AT BELCOURT-QUENTIN(701) 477-6 N BURDICK111 350063 Shelly Harris 01-ACTIVE PO BOX 160 (701) 477-8410 ROLETTE 0/0 BELCOURT, ND 58316 Sanford Bismarck (5003A) MICHAEL LEBEAU HOSP-ACU SANFORD MEDICAL CENTER BISMARCK(701) 323-6000 350015 01-ACTIVE 300 N 7TH ST (701) 323-5221 1002 BURLEIGH 223/223 BISMARCK, ND 58506 Sanford Bismarck Transplant Center (NDTH00147) MICHAEL LEBEAU TH SANFORD BISMARCK TRANSPLANT CENTER(701) 323-2828 359810 01-ACTIVE 300 N 7TH ST (701) 323-2801 BURLEIGH 0/0 BISMARCK, ND 58501 St. Alexius Medical Center (5004A) KURT SCHLEY HOSP-ACU CHI ST ALEXIUS HEALTH (701) 530-7000 350002 Kurt Schley 01-ACTIVE 900 E BROADWAY (701) 530-7612 1003 BURLEIGH 287/287 BISMARCK, ND 58501 [email protected] St. Andrew's Hospital (5005P) ALFRED SAMS HOSP-CAH ST ANDREWS HEALTH CENTER - CAH (701) 228-9300 351307 Alfred Sams 01-ACTIVE 316 OHMER STREET (701) 228-9384 1004 BOTTINEAU 25/25 BOTTINEAU, ND 58318 [email protected] Southwest -

Sanford Health Offering No-Appointment-Necessary Sports Physical Blitzes
July 26, 2021 Erin Johnson Sanford Health Media Relations 701-516-4903 [email protected] Sanford Health offering no-appointment-necessary sports physical blitzes BISMARCK, N.D. — Sanford Health will hold no-appointment-necessary sports physical blitzes for student athletes at select clinics in the Bismarck-Mandan area. These blitzes will be held from 5:30 p.m. to 8 p.m. on July 28, August 4, and August 11 at the following clinics: • Sanford North Mandan Clinic • Sanford Northern Sky Clinic • Sanford South Clinic Walk in during a blitz or call your child’s primary care physician to schedule an appointment. The North Dakota High School Activities Association requires annual sports physicals for all athletes participating in school-sanctioned sports. Athletes must have their physicals completed before the first day of practice for their sport. For more information, visit sanfordhealth.org. The Sanford Bismarck region provides health care to central and western North Dakota, eastern Montana and northern South Dakota. It includes 21 clinics in Bismarck, Mandan, Minot, Dickinson and Watford City, as well as a Level II trauma center located in Bismarck. About Sanford Health Sanford Health, one of the largest health systems in the United States, is dedicated to the integrated delivery of health care, genomic medicine, senior care and services, global clinics, research and affordable insurance. Headquartered in Sioux Falls, South Dakota, the organization includes 46 hospitals, 1,500 physicians and more than 200 Good Samaritan Society senior care locations in 26 states and 10 countries. Learn more about Sanford Health's transformative work to improve the human condition at sanfordhealth.org or Sanford Health News. -

Health IT Partner Organizations As of 11-16-20
Social Security, paving the way for national interoperability… Current status (as of 11/16/20) – 200 organizations representing 26,728 participating providers Partner Organization States With Participating Facilities Advocate Aurora Health IL, WI Alameda Health System CA Allegheny Health Network OH, PA, WV Allina Health MN, WI Altru Health System MN, ND Anne Arundel Medical Center MD Asante Health System OR Aspirus System MI, WI Atlantic Health NJ, PA Baptist Health Arkansas AR Baptist Memorial Healthcare AR, MS, TN Bayhealth Medical Center DE Beth Israel Deaconess Medical Center MA Bronson Healthcare MI Bryan Health NE Buffalo Medical Group NY Cape Fear Valley Health System NC Carilion Clinic VA Carle Foundation Hospital IL CaroMont Health NC, SC Cedars-Sinai Health System CA Centura Health CO, KS, MT, NM Cheyenne Regional Medical Center WY Children's Healthcare of Atlanta GA Children's Hospital Colorado CO, MT, WY Children’s Hospital of Philadelphia NJ, PA Children's Medical Center of Dallas TX CHRISTUS Trinity Mother Frances Health System TX Page 1 of 7 Partner Organization States With Participating Facilities Cincinnati Children’s Hospital Medical Center IN, KY, OH City of Hope CA Cleveland Clinic FL, NV, OH Columbus Regional Health IN Community Medical Centers CA Conemaugh Health System PA Confluence Health WA Contra Costa Health Services CA Cottage Health CA Covenant HealthCare MI Dartmouth-Hitchcock NH, VT Dayton Children’s Hospital OH Denver Health Hospital Authority CO Department of Defense National/International Department of