Maryland Ambulance Information System User's Manual 7
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Wellspan Health Financial Assistance Policy
WellSpan Health Manual of Administrative Policy Page 1 of 18 Policy #118 - WellSpan Health Financial Assistance WellSpan Health adopts the following policy and procedure for the following specifically named entities ☒ Apple Hill Surgical Center ☒ VNA Home Health and Services ☒ WellSpan Medical Equipment ☒ WellSpan Medical Group ☒ WellSpan Pharmacy ☒ WellSpan Philhaven ☒ WellSpan Surgery and Rehabilitation Hospital ☒ WellSpan Ephrata Community Hospital ☒ WellSpan Gettysburg Hospital ☒ WellSpan Good Samaritan Hospital ☒ WellSpan York Hospital ☒ Good Samaritan Physician Services ☒ WellSpan Health System Corporate Locations ☒ Chambersburg Hospital ☒ Waynesboro Hospital ☒ WellSpan Summit Physician Services ☒ Summit Himelfarb Surgery Center ☒ WellSpan Radiation Oncology ☒ WellSpan Medical Oncology and Hematology NOTE: This policy applies to the above-named entities and all providers employed by WellSpan. Independent providers and entities providing services within WellSpan Hospitals are not required to adopt this policy. All providers of medically necessary care in WellSpan facilities who are not employed by such facilities are listed on Attachment B. None of the providers listed in Attachment B are covered by the FAP and do not apply the same discounts for services provided. PURPOSE Consistent with its charitable mission of “working as one to improve health through exceptional care for all, lifelong wellness and healthy communities,” WellSpan Health provides financial assistance to eligible patients who are in need. The Financial Assistance Policy will be fair, efficient and accessible to all patients and will be consistently applied across all WellSpan Health entities. POLICY AND PROCEDURE I. SCOPE AND GUIDING PRINCIPLES A. WellSpan Health will provide essential care to patients regardless of their ability to pay. B. WellSpan Health will provide discounts to patients according to the patient’s financial status. -

CURRICULUM VITAE Deborah J. Baker, DNP, ACNP, NEA-BC PERSONAL DATA
CURRICULUM VITAE Deborah J. Baker, DNP, ACNP, NEA-BC PERSONAL DATA Work Address: The Johns Hopkins Hospital Billings Administration 107 600 N Wolfe St Baltimore, MD 21287-1607 Phone: 410-955-4222 Fax: 410-614-0694 EMPLOYMENT HISTORY Years Position Institution/Location 2016- Present Sr. Vice President for Nursing Johns Hopkins Health System Vice President for Nursing & Patient Care Services and The Johns Hopkins Hospital Chief Nursing Officer Baltimore, MD 2017-Present Associate Dean for Health Systems Johns Hopkins University Partnership and Innovation School of Nursing Faculty Joint Appointment 2015-2016 Interim Vice President for Nursing The Johns Hopkins Hospital & Patient Care Services and Baltimore, MD Chief Nursing Officer 2008 – 2015 Director of Nursing The Johns Hopkins Hospital Department of Surgery Baltimore, MD 2006 – 2009 Co-Director, Postgraduate Surgical The Johns Hopkins Hospital Physician Assistant Residency Program Department of Surgery Baltimore, MD 2005 – 2008 Assistant Director of Nursing The Johns Hopkins Hospital Department of Surgery Baltimore, MD 2003 – 2006 Advanced Practice Manager The Johns Hopkins Hospital Department of Surgery Baltimore, MD 1999 – 2007 Clinical Instructor, Acute and Primary Johns Hopkins University Care Nurse Practitioner Programs School of Nursing Baltimore, MD 1997 – 2014 Acute Care Nurse Practitioner The Johns Hopkins Hospital Department of Surgery Baltimore, MD 1997 – 2014 Nurse Practitioner General Surgery and Surgical Oncology Service 1997 – 2004 Acute Care Nurse Practitioner The Johns -

Maryland State Trauma Registry Data Dictionary for Adult Patients April 21
Maryland State Trauma Registry Data Dictionary for Adult Patients April 21, 2017 Maryland Institute for Emergency Medical Services Systems Richard Alcorta, M.D. F.A.C.E.P. Acting Co-Executive Director Patricia Gainer, J.D., M.P.A. Acting Co-Executive Director Melanie Gertner, B.S. Data Services Carole Mays, R.N., M.S., C.E.N. Trauma and Injury Specialty Care Program Cynthia Wright-Johnson, R.N., M.S.N. EMSC Program Maryland Designated Trauma Centers Trauma Program Managers Susie Burleson, R.N., B.S.N., M.S.N., M.B.A Meritus Medical Center Kari Cheezum, R.N., B.S.N., C.E.N. Peninsula Regional Medical Center Diana Clapp, R.N., C.C.R.N., B.S.N., N.R.P. R Adams Cowley Shock Trauma Center Marie Dieter, M.S.N., M.B.A., R.N., C.E.N. Johns Hopkins Bayview Medical Center Jen Fritzeen, M.S.N., R.N. Children's National Medical Center Melissa Meyers, R.N., B.S.N., C.E.N. Suburban Hospital - Johns Hopkins Medicine Dawn Moreland, B.S.N., R.N. Prince George’s Hospital Center Kathy Noll, M.S.N., R.N. Johns Hopkins Hospital Lauren Heinrich Smith, M.S., A.C.N.P. Sinai Hospital Sandy Waak, R.N., C.E.N., T.C.R.N. R Adams Cowley Shock Trauma Center Elizabeth Wooster, R.N., B.S.N., M.S., Ms.E.M. Western Maryland Regional Medical Center Susan Ziegfeld, C.C.R.N., M.S.N., C.P.N.P. Johns Hopkins Hospital Special Acknowledgements ` Daniel A. -
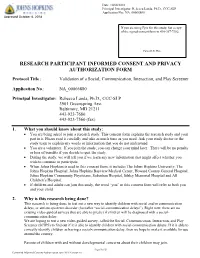
Research Participant Informed Consent and Privacy Authorization Form
Do not use this form for consenting research Date: 10/08/2018 participants unless the Johns Hopkins Medicine Principal Investigator: Rebecca Landa, Ph.D., CCC-SLP Logo appears here. Application No.: NA_00066880 Approved October 8, 2018 If you are using Epic for this study, fax a copy of the signed consent form to 410-367-7382. Patient I.D. Plate RESEARCH PARTICIPANT INFORMED CONSENT AND PRIVACY AUTHORIZATION FORM Protocol Title: Validation of a Social, Communication, Interaction, and Play Screener Application No.: NA_00066880 Principal Investigator: Rebecca Landa, Ph.D., CCC-SLP 3901 Greenspring Ave. Baltimore, MD 21211 443-923-7680 443-923-7560 (fax) 1. What you should know about this study: You are being asked to join a research study. This consent form explains the research study and your part in it. Please read it carefully and take as much time as you need. Ask your study doctor or the study team to explain any words or information that you do not understand. You are a volunteer. If you join the study, you can change your mind later. There will be no penalty or loss of benefits if you decide to quit the study. During the study, we will tell you if we learn any new information that might affect whether you wish to continue to participate. When Johns Hopkins is used in this consent form, it includes The Johns Hopkins University, The Johns Hopkins Hospital, Johns Hopkins Bayview Medical Center, Howard County General Hospital, Johns Hopkins Community Physicians, Suburban Hospital, Sibley Memorial Hospital and All Children’s Hospital. If children and adults can join this study, the word “you” in this consent form will refer to both you and your child. -

Blue Medicare Advantage HMO Contracted Providers
Appendix D Blue Medicare Advantage HMO Contracted Providers Ambulatory Surgicenters ………………………………………………………... 2 Durable Medical Equipment ……………………………………………………... 3 Home Health Care ………………………………………………………………... 4 Home Infusion ……………………………………………………………………. 6 Hospice …………………………………………………………………………… 7 Inpatient – Metro Hospitals ………………………………………………………. 8 Long Term Acute Care ………………………………………………………….. 12 Mental Health IP/OP …………………………………………………………….. 13 Orthotic & Prosthetic …………………………………………………………….. 14 Hospital Based Outpatient Surgery ………………………………………………. 17 Renal Dialysis ……………………………………………………………………. 20 Skilled Nursing Facilities ………………………………………………………… 27 Substance Use Disorder ………………………………………………………… 32 A Division of Healthcare Service Corporation, a Mutual Legal Reserve Company, an Independent Licensee of the Blue Cross and Blue Shield Association 2 Appendix D MEDICARE ADVANTAGE CONTRACTED PROVIDER NETWORK Change Provider Type Effective Date Cancel Date Provider Name Address City State Zip Telephone Code Change Date Surgicenter 01/01/2013 Center for Reconstructive Surgery 6309 W 95th St Oak Lawn IL 60453 (708) 499-3355 Surgicenter 01/01/2013 DMG Pain Management Surgery Ct 2940 Rolling Ridge Rd. Naperville IL 60564 (630) 303-5304 A 11/26/12 Surgicenter 01/01/2013 DMG Surgical Center, LLC 2725 S. Technology Drive Lombard IL 60148 (630) 942-7998 60126- Surgicenter 01/01/2013 Elmhurst Outpatient Surgery 1200 S. York Road Elmhurst IL 5626 (630) 758-8457 Novamed Surgery Ct of Chicago Northshore Surgicenter 01/01/2013 LLG 3034 W. Peterson Ave. Chicago IL -

COURT of CLAIMS of THE
REPORTS OF Cases Argued and Determined IN THE COURT of CLAIMS OF THE STATE OF ILLINOIS VOLUME 39 Containing cases in which opinions were filed and orders of dismissal entered, without opinion for: Fiscal Year 1987 - July 1, 1986-June 30, 1987 SPRINGFIELD, ILLINOIS 1988 (Printed by authority of the State of Illinois) (65655--300-7/88) PREFACE The opinions of the Court of Claims reported herein are published by authority of the provisions of Section 18 of the Court of Claims Act, Ill. Rev. Stat. 1987, ch. 37, par. 439.1 et seq. The Court of Claims has exclusive jurisdiction to hear and determine the following matters: (a) all claims against the State of Illinois founded upon any law of the State, or upon an regulation thereunder by an executive or administrative ofgcer or agency, other than claims arising under the Workers’ Compensation Act or the Workers’ Occupational Diseases Act, or claims for certain expenses in civil litigation, (b) all claims against the State founded upon any contract entered into with the State, (c) all claims against the State for time unjustly served in prisons of this State where the persons imprisoned shall receive a pardon from the Governor stating that such pardon is issued on the grounds of innocence of the crime for which they were imprisoned, (d) all claims against the State in cases sounding in tort, (e) all claims for recoupment made by the State against any Claimant, (f) certain claims to compel replacement of a lost or destroyed State warrant, (g) certain claims based on torts by escaped inmates of State institutions, (h) certain representation and indemnification cases, (i) all claims pursuant to the Law Enforcement Officers, Civil Defense Workers, Civil Air Patrol Members, Paramedics and Firemen Compensation Act, (j) all claims pursuant to the Illinois National Guardsman’s and Naval Militiaman’s Compensation Act, and (k) all claims pursuant to the Crime Victims Compensation Act. -

Johns Hopkins University Style Guide Contents Introduction Names
JHU Office of Communications Style Guide page 1 Johns Hopkins University Style Guide Contents • Introduction • Names: Johns Hopkins University and its divisions • Style guidelines Introduction These guidelines were compiled by editors in the Office of Communications to encourage consistency and correct usage of terms across the many publications produced by JHU offices. The guidelines draw from The Associated Press Stylebook 2019 and the 17th edition of The Chicago Manual of Style. Written from a Johns Hopkins point of view, the guidelines are intended to complement AP and CMOS and, when those sources disagree, to choose between them. For points not addressed in the university guidelines, AP is the preferred source. For points not listed in AP, use the dictionary it recommends: Webster’s New World College Dictionary. When the dictionary gives two spellings, use the first one; when the dictionary and AP give different spellings, use AP’s. A number of individual JHU publications have their own style sheets, more detailed and directed to handling specialized content. Johns Hopkins Medicine, for example, has posted its Branding and Use of Name Toolkit http://brand.hopkinsmedicine.org/gui/content.asp. The guidelines below will supplement those already existing and will contribute to the effort to bring overall consistency to university publications. Names: Johns Hopkins University and its divisions The Johns Hopkins University/The Johns Hopkins Hospital: The preferred shortened name for Johns Hopkins University is Johns Hopkins, not Hopkins. The acronym JHU can be used as a shortened form in informal or internal communications and to avoid repetition of the Hopkins name. -

Peninsula Regional Medical Center, Is a 266-Bed General Hospital Located in Salisbury (Wicomico County)
IN THE MATTER OF * BEFORE THE TIDALHEALTH PENINSULA * MARYLAND REGIONAL * HEALTH CARE * COMMISSION Docket No.: 19-22-CP019 * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * STAFF REPORT AND RECOMMENDATION CERTIFICATE OF ONGOING PERFORMANCE FOR PRIMARY & ELECTIVE PERCUTANEOUS CORONARY INTERVENTION SERVICES November 19, 2020 I. INTRODUCTION A. Background Percutaneous coronary intervention (PCI), commonly known as coronary angioplasty, is a non-surgical procedure whereby a catheter is inserted in a blood vessel and guided to the site of the narrowing of a coronary artery to relieve coronary narrowing. Primary (or emergency) PCI programs provide emergency PCI intervention in the event of a heart attack shortly after it begins. Elective (or non-primary) PCI programs provide interventions that revascularize coronary arteries that are substantially blocked but have not yet resulted in an immediate cardiac event. For many years, only Maryland hospitals with on-site cardiac surgery services could provide PCI. However, in the 1990s, Maryland began allowing some hospitals to perform primary PCI services without cardiac surgery on-site, first as part of research trials evaluating the safety of providing primary PCI at such hospitals and, later, as a regular clinical service, based on the research findings. The Commission issued waivers to hospitals in order to exempt these hospitals from the requirement for co-location of PCI services with cardiac surgery. In the following decade, similar research evaluated the safety of providing elective PCI services at hospitals without on-site cardiac surgery. The nine Maryland hospitals that obtained waivers to provide elective PCI services participated in a multi-site clinical trial, C-PORT E, a study that was approved by the Commission upon the recommendation of its Research Proposal Review Committee. -

Emergency Room Listing
MARYLAND DEPARTMENT OF NATURAL RESOURCES ONLINE LICENSING AND REGISTRATION SYSTEM EMERGENCY ROOM LISTING Allegany County • Western Maryland Regional Medical Center, 12500 Willowbrook Rd., Cumberland, MD 21502; 240-964-1200 Anne Arundel County • Anne Arundel Medical Center, 2001 Medical Parkway, Annapolis, MD 21401; 443-481-1200 • Baltimore Washington Medical Center, 301 Hospital Dr., Glen Burnie, MD 21061; 410-787-4565 Baltimore City • Bon Secours Hospital, 2000 West Baltimore St., Baltimore, MD 21223; 410-362-3075 • Good Samaritan Hospital, 5601 Loch Raven Blvd., Baltimore, MD 21239; 410-532-4040 • Harbor Hospital, 3001 S. Hanover St., Baltimore, MD 21225; 410-350-3510 • Johns Hopkins Bayview Medical Center, 4940 Eastern Ave., Baltimore, MD 21224; 410-550-0350 • The Johns Hopkins Hospital, 600 North Wolfe St., Baltimore, MD 21287; 410-955-2280 • Maryland General Hospital, 827 Linden Ave., Baltimore, MD 21201; 410-225-8100 • Mercy Medical Center, 301 St. Paul Place, Baltimore, MD 21202; 410-332-9477 • Saint Agnes Hospital, 900 Caton Ave., Baltimore, MD 21229; 410-368-2000 • Sinai Hospital of Baltimore, 2401 West Belvedere Ave., Baltimore, MD 21215; 410-601-8800 • University of Maryland Medical Center, 22 South Green St., Baltimore, MD 21201; 410-328-9595 • Union Memorial Hospital, 201 East University Pkwy., Baltimore, MD 21218; 410-554-2600 Baltimore County • Northwest Hospital Center, 5401 Old Court Rd., Randallstown, MD 21133; 410-521-2200 • Franklin Square Hospital Center, 9000 Franklin Square Dr., Baltimore, MD 21237; 443-777-7046 -

When Delivery Time Comes Stuart M
2017 FALL When Delivery Time Comes Ensuring Moms-to-Be Get the Care They Need Novel Treatments for Complex Conditions Patients With Advanced Liver Cancer Among Those Benefitting Keeping Athletes in the Game Athletic Trainers Play a Key Role in Preventing and Managing Injuries [CONTENTS] FALL 2017 INTRODUCING OUR NEW PRESIDENT AND CHIEF MEDICAL OFFICER FEATURES Stuart M. Levine, MD, FACP, was recently named president and Novel Treatments for chief medical officer of MedStar 4 Complex Conditions Harbor Hospital and a senior vice Patients With Advanced Liver Cancer president of MedStar Health. He succeeds Dennis W. Pullin, Among Those Benefitting FACHE, the former president, who left MedStar Harbor after When Delivery Time Comes Stuart M. Levine, eight years of strong leadership. 8 Ensuring Moms-to-Be Get the MD, FACP Care They Need “My excitement at being appointed to this new role is beyond words,” says Dr. Levine. “What a privilege Keeping Athletes in the Game and responsibility it is to lead a phenomenal 10 Athletic Trainers Play a Key Role in organization committed to being on the forefront Preventing and Managing Injuries of healthcare delivery. I am overjoyed to continue working with all of the talented and dedicated Seasonal Depression individuals who make MedStar Harbor the vibrant 14 It’s Not Just in Your Head ... place that it is today. Together, we are one big Treatment Can Help family collectively focused on providing the highest quality and safest care possible. I am grateful for this opportunity to help write the next chapter of MedStar Harbor’s history as we move full steam DEPARTMENTS ahead on our journey of continued success.” 3 WHAT’S NEW Most recently, Dr. -

Suburban Hospital, Inc. and Controlled Entities Consolidated Financial Statements June 30, 2013 and 2012 Suburban Hospital, Inc
Suburban Hospital, Inc. and Controlled Entities Consolidated Financial Statements June 30, 2013 and 2012 Suburban Hospital, Inc. and Controlled Entities Index June 30, 2013 and 2012 Page(s) Independent Auditor’s Report .................................................................................................................. 1 Consolidated Financial Statements Balance Sheets ........................................................................................................................................ 2–3 Statements of Operations and Other Changes in Unrestricted Net Assets ................................................. 4 Statements of Changes in Net Assets ......................................................................................................... 5 Statements of Cash Flows ........................................................................................................................... 6 Notes to Financial Statements ............................................................................................................... 7–34 Supplemental Information Independent Auditor’s Report on Supplemental Information ..................................................................... 35 Consolidating Statement of Operations and Other Changes in Unrestricted Net Assets .......................... 36 Independent Auditor's Report To the Board of Trustees of Suburban Hospital, Inc. and Control Entities We have audited the accompanying consolidated financial statements of Suburban Hospital, Inc. and Controlled -
User's Manual
MIEMSS Commercial Ambulance Licensing and Regulation COMMERCIAL—MAIS USER’S MANUAL July 2000 REV. 07/05/00 Table of Contents Page General Form Identification 1 Sample Commercial MAIS form. 2 Section 1 Location, Patient, and Provider Information 3 Section 2 Unit, Crew, Date, Origen and Destination Information 4 Section 3 Documentation of Response Times and Facility Codes 5 Section 4 Vital Signs, Transport Reason, Signs and Symptoms 6 Section 5 Airway/Ventilation, Circulation, and Other 7 Section 6 Care, Skills, Medications and Special Items 9 Section 7 Narrative 10 Appendix A Receiving Facility Codes 11 b GENERAL: FORM IDENTIFICATION MIEMSS RECORD—the TOP COPY is the SCANNABLE document to be submitted to MIEMSS. OFFICIAL COPY–is the legal copy of the record and should be retained at the company level. HOSPITAL COPY–is the copy to be left at the reciving facility. PLEASE DO NOT: Staple, tape, bend, or otherwise mutilate the top copy. This copy is fed through a scanner, stapling, taping, or attaching items such as ECG strips creates a significant problem. 1 2 SECTION 1: LOCATION, PATIENT, AND PROVIDER INFORMATION Response Location Record the location where you picked up the patient. Be as specific as possible. Ex. St. Joseph Hospital, Room 712B or 125 Smith Street, Bowie, MD Destination Record the location where you delivered the patient. Be as specific as possible. Ex. Garrett Memorial Hosp., Room 301 or 765 North Prospect Avenue, Cumberland, MD Patient Name Print the patient’s last name, first name, middle initial. Patient Address Print the patient’s residential address—include street address, city, and zip code.