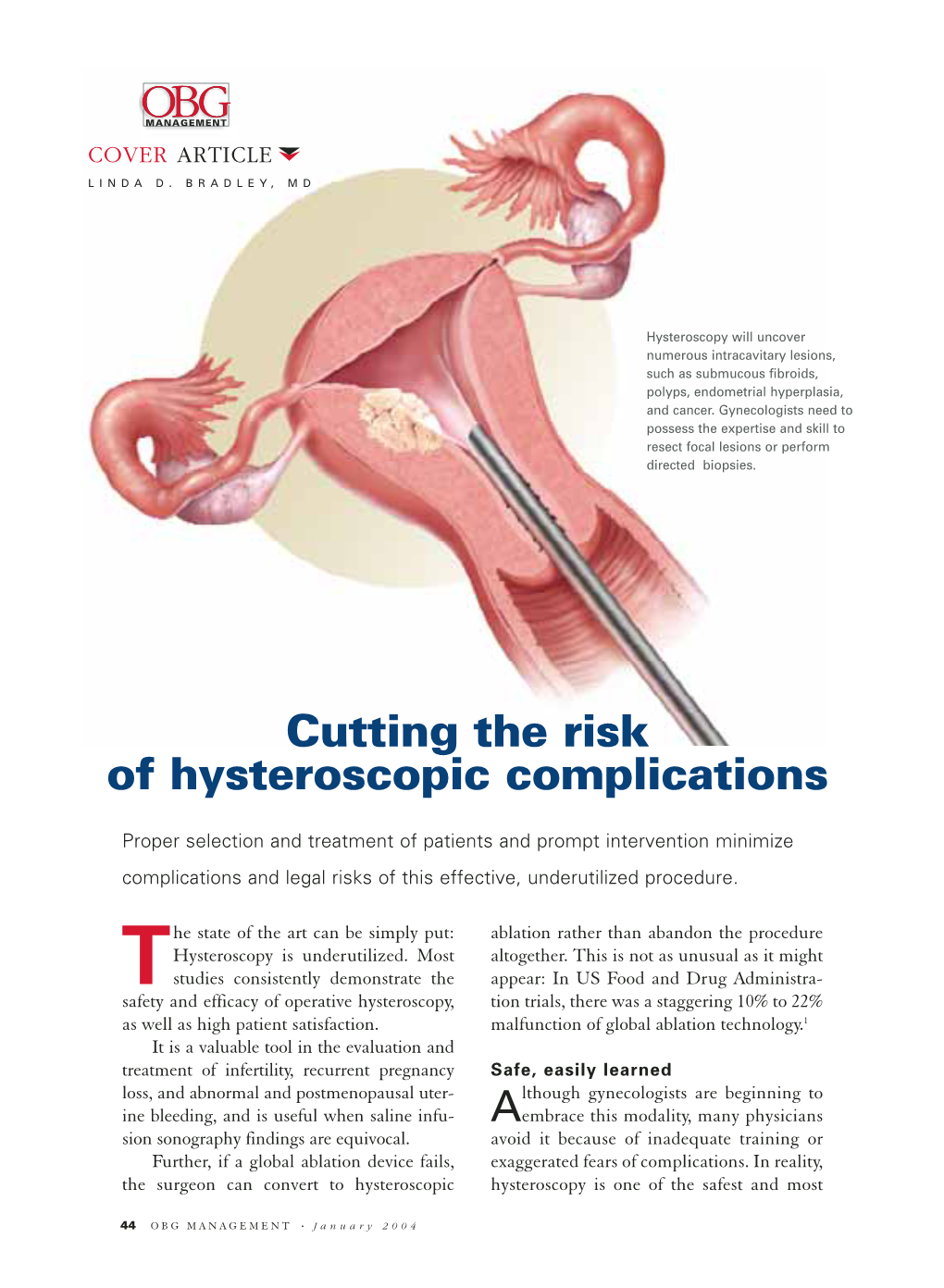
Cutting the Risk of Hysteroscopic Complications
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Hysteroscopy with Dilation and Curretage (D & C)
501 19th Street, Trustees Tower FORT SANDERS WOMEN’S SPECIALISTS 1924 Pinnacle Point Way Suite 401, Knoxville Tn 37916 P# 865-331-1122 F# 865-331-1976 Suite 200, Knoxville Tn 37922 Dr. Curtis Elam, M.D., FACOG, AIMIS, Dr. David Owen, M.D., FACOG, Dr. Brooke Foulk, M.D., FACOG Dr. Dean Turner M.D., FACOG, ASCCP, Dr. F. Robert McKeown III, M.D., FACOG, AIMIS, Dr. Steven Pierce M.D., Dr. G. Walton Smith, M.D., FACOG, Dr. Susan Robertson, M.D., FACOG HYSTEROSCOPY WITH DILATION AND CURRETAGE (D & C) Please read and sign the following consent form when you feel that you completely understand the surgical procedure that is to be performed and after you have asked all of your questions. If you have any further questions or concerns, please contact our office prior to your procedure so that we may clarify any pertinent issues. Definition: HysterosCopy is an outpatient procedure that allows your doctor direct visualization of the inside of the uterine cavity (womb) by inserting a thin lighted telescope (hysteroscope) through the vagina (birth canal) and cervix, without making an abdominal incision. This procedure enables your doctor to examine the lining of the uterus, look for polyps, fibroids, scar tissue, blockages of the fallopian tubes, and abnormal partitions. In addition, this procedure allows your doctor to remove or surgically treat many of the abnormalities seen. Dilation and Curettage (D&C) allows your doctor to take a sample of the tissue that lines your uterus (endometrium) and/or to remove polyps, fibroid tumors, or hyperplasia. Suction D&C is used in cases of miscarriage. -

Ovarian Cancer and Cervical Cancer
What Every Woman Should Know About Gynecologic Cancer R. Kevin Reynolds, MD The George W. Morley Professor & Chief, Division of Gyn Oncology University of Michigan Ann Arbor, MI What is gynecologic cancer? Cancer is a disease where cells grow and spread without control. Gynecologic cancers begin in the female reproductive organs. The most common gynecologic cancers are endometrial cancer, ovarian cancer and cervical cancer. Less common gynecologic cancers involve vulva, Fallopian tube, uterine wall (sarcoma), vagina, and placenta (pregnancy tissue: molar pregnancy). Ovary Uterus Endometrium Cervix Vagina Vulva What causes endometrial cancer? Endometrial cancer is the most common gynecologic cancer: one out of every 40 women will develop endometrial cancer. It is caused by too much estrogen, a hormone normally present in women. The most common cause of the excess estrogen is being overweight: fat cells actually produce estrogen. Another cause of excess estrogen is medication such as tamoxifen (often prescribed for breast cancer treatment) or some forms of prescribed estrogen hormone therapy (unopposed estrogen). How is endometrial cancer detected? Almost all endometrial cancer is detected when a woman notices vaginal bleeding after her menopause or irregular bleeding before her menopause. If bleeding occurs, a woman should contact her doctor so that appropriate testing can be performed. This usually includes an endometrial biopsy, a brief, slightly crampy test, performed in the office. Fortunately, most endometrial cancers are detected before spread to other parts of the body occurs Is endometrial cancer treatable? Yes! Most women with endometrial cancer will undergo surgery including hysterectomy (removal of the uterus) in addition to removal of ovaries and lymph nodes. -

Adenomyosis in Infertile Women: Prevalence and the Role of 3D Ultrasound As a Marker of Severity of the Disease J
Puente et al. Reproductive Biology and Endocrinology (2016) 14:60 DOI 10.1186/s12958-016-0185-6 RESEARCH Open Access Adenomyosis in infertile women: prevalence and the role of 3D ultrasound as a marker of severity of the disease J. M. Puente1*, A. Fabris1, J. Patel1, A. Patel1, M. Cerrillo1, A. Requena1 and J. A. Garcia-Velasco2* Abstract Background: Adenomyosis is linked to infertility, but the mechanisms behind this relationship are not clearly established. Similarly, the impact of adenomyosis on ART outcome is not fully understood. Our main objective was to use ultrasound imaging to investigate adenomyosis prevalence and severity in a population of infertile women, as well as specifically among women experiencing recurrent miscarriages (RM) or repeated implantation failure (RIF) in ART. Methods: Cross-sectional study conducted in 1015 patients undergoing ART from January 2009 to December 2013 and referred for 3D ultrasound to complete study prior to initiating an ART cycle, or after ≥3 IVF failures or ≥2 miscarriages at diagnostic imaging unit at university-affiliated private IVF unit. Adenomyosis was diagnosed in presence of globular uterine configuration, myometrial anterior-posterior asymmetry, heterogeneous myometrial echotexture, poor definition of the endometrial-myometrial interface (junction zone) or subendometrial cysts. Shape of endometrial cavity was classified in three categories: 1.-normal (triangular morphology); 2.- moderate distortion of the triangular aspect and 3.- “pseudo T-shaped” morphology. Results: The prevalence of adenomyosis was 24.4 % (n =248)[29.7%(94/316)inwomenaged≥40 y.o and 22 % (154/ 699) in women aged <40 y.o., p = 0.003)]. Its prevalence was higher in those cases of recurrent pregnancy loss [38.2 % (26/68) vs 22.3 % (172/769), p < 0.005] and previous ART failure [34.7 % (107/308) vs 24.4 % (248/1015), p < 0.0001]. -

Dysmenorrhoea
[ Color index: Important | Notes| Extra | Video Case ] Editing file link Dysmenorrhoea Objectives: ➢ Define dysmenorrhea and distinguish primary from secondary dysmenorrhea ➢ • Describe the pathophysiology and identify the etiology ➢ • Discuss the steps in the evaluation and management options References : Hacker and moore, Kaplan 2018, 428 boklet ,433 , video case Done by: Omar Alqahtani Revised by: Khaled Al Jedia DYSMENORRHEA Definition: dysmenorrhea is a painful menstruation it could be primary or secondary Primary dysmenorrhea Definition: Primary dysmenorrhea refers to recurrent, crampy lower abdominal pain, along with nausea, vomiting, and diarrhea, that occurs during menstruation in the absence of pelvic pathology. It is the most common gynecologic complaint among adolescent girls. Characteristic: The onset of pain generally does not occur until ovulatory menstrual cycles are established. Maturation of the hypothalamic-pituitary-gonadal axis leading to ovulation occurs in half of the teenagers within 2 years post-menarche, and the majority of the remainder by 5 years post-menarche. (so mostly it’s occur 2-5 years after first menstrual period) • The symptoms typically begin several hours prior to the onset of menstruation and continue for 1 to 3 days. • The severity of the disorder can be categorized by a grading system based on the degree of menstrual pain, the presence of systemic symptoms, and impact on daily activities Pathophysiology Symptoms appear to be caused by excess production of endometrial prostaglandin F2α resulting from the spiral arteriolar constriction and necrosis that follow progesterone withdrawal as the corpus luteum involutes. The prostaglandins cause dysrhythmic uterine contractions, hypercontractility, and increased uterine muscle tone, leading to uterine ischemia. -

0637-129-01 G Ultrapulse CO2 Laser Op Manual English.Book
UltraPulse® Carbon Dioxide Laser Operator Manual for EncoreTM and SurgiTouchTM Models This manual is copyrighted with all rights reserved. Under copyright laws, this manual may not be copied in whole or in part or reproduced in any other media without the express written permission of Lumenis. Permitted copies must carry the same proprietary and copyright notices as were affixed to the original. Under the law, copying includes translation into another language. Please note that while every effort has been made to ensure that the data given in this document is accurate, the information, figures, illustrations, tables, specifications, and schematics contained herein are subject to change without notice. Lumenis, the Lumenis logo, UltraPulse, UltraPulse SurgiTouch, SurgiTouch+, Encore, UltraScan CPG, PigmentFX, ActiveFX, ActiveFX gentle, MaxFX, DeepFX, SCAAR FX, PreciseFX, IncisionFX, BrowFX, CoolScan, CO2 Lite, TrueSpot, ClearSpot, UltraFlex, Lumenis/Nezhat, AcuSpot, OtoScan, OtoLAM, AcuBlade, BeamAlign, MicroSlad, and FiberLase are trademarks or registered trademarks of Lumenis. Retin-A and Renova are registered trademarks of Ortho Pharmaceuticals Corporation, Dermatological Division. Melanex is a registered trademark of Neutrogena Dermatologics. Valtrex is a registered trademark of Glaxo Wellcome, Inc. Famvir is a registered trademark of SmithKline Beecham Pharmaceuticals. Cipro is a registered trademark of Bayer Corporation. Coppertone and Shade are trademarks, distributed by Schering-Plough HealthCare Products, Inc. Vaseline is a registered trademark of Chesebrough-Pond’s USA, Co. Acutane is a registered trademark of Roche Laboratories, Inc. Copyright© Lumenis Ltd. Authorized Representative: May 2012 Lumenis GmbH Germany 0637-129-01 Heinrich-Hertz-Strasse 3 Revision G D-63303 Dreieich-Dreieichenhain Germany Manufactured by Lumenis Ltd. P. -

2021 – the Following CPT Codes Are Approved for Billing Through Women’S Way
WHAT’S COVERED – 2021 Women’s Way CPT Code Medicare Part B Rate List Effective January 1, 2021 For questions, call the Women’s Way State Office 800-280-5512 or 701-328-2389 • CPT codes that are specifically not covered are 77061, 77062 and 87623 • Reimbursement for treatment services is not allowed. (See note on page 8). • CPT code 99201 has been removed from What’s Covered List • New CPT codes are in bold font. 2021 – The following CPT codes are approved for billing through Women’s Way. Description of Services CPT $ Rate Office Visits New patient; medically appropriate history/exam; straightforward decision making; 15-29 minutes 99202 72.19 New patient; medically appropriate history/exam; low level decision making; 30-44 minutes 99203 110.77 New patient; medically appropriate history/exam; moderate level decision making; 45-59 minutes 99204 165.36 New patient; medically appropriate history/exam; high level decision making; 60-74 minutes. 99205 218.21 Established patient; evaluation and management, may not require presence of physician; 99211 22.83 presenting problems are minimal Established patient; medically appropriate history/exam, straightforward decision making; 10-19 99212 55.88 minutes Established patient; medically appropriate history/exam, low level decision making; 20-29 minutes 99213 90.48 Established patient; medically appropriate history/exam, moderate level decision making; 30-39 99214 128.42 minutes Established patient; comprehensive history exam, high complex decision making; 40-54 minutes 99215 128.42 Initial comprehensive -

National Institute for Health and Care Excellence
IP1242 [IPG509] NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE INTERVENTIONAL PROCEDURES PROGRAMME Interventional procedure overview of hysteroscopic metroplasty of a uterine septum for primary infertility or recurrent miscarriage In some women the uterus (womb) is divided into 2 halves by a thin wall of tissue, called a septum. This may affect fertility and increase the risk of miscarriage. In hysteroscopic metroplasty a thin tube with a camera on the end (a hysteroscope) is inserted into the vagina, through the cervix and into the womb. Instruments are passed through the hysteroscope into the womb and the septum is removed. Introduction The National Institute for Health and Care Excellence (NICE) has prepared this interventional procedure (IP) overview to help members of the Interventional Procedures Advisory Committee (IPAC) make recommendations about the safety and efficacy of an interventional procedure. It is based on a rapid review of the medical literature and specialist opinion. It should not be regarded as a definitive assessment of the procedure. Date prepared This IP overview was prepared in April 2014 and updated in November 2014. Procedure name Hysteroscopic metroplasty of uterine septum in women with primary infertility or recurrent miscarriage Specialist societies Royal College of Obstetricians and Gynaecologists (RCOG) British Fertility Society. IP overview: hysteroscopic metroplasty of uterine septum in women with primary infertility or recurrent miscarriage 1 of 44 IP1242 [IPG509] Description Indications and current treatment A septate uterus is a type of congenital uterine anomaly, in which the inside of the uterus is divided by a muscular or fibrous wall, called the septum. The septum may be partial or complete, extending as far as the cervix. -

Dysmenorrhea Due to a Rare Müllerian Anomaly
CASE REPORT Dysmenorrhea due to a rare müllerian anomaly M Agarwal, A Das, AS Singh Department of Obstetrics and Gynecology, North Eastern Indira Gandhi Regional Institute of Health and Medical Sciences Shillong, India Abstract Müllerian duct anomalies may produce reproductive failure like abortion and preterm birth, or obstetric problems like malpresentation, retained placenta, etc., or they may be asymptomatic. Unicornuate uterus with a noncommunicating functional rudimentary horn is a type of müllerian anomaly that results in obstruction to menstrual blood flow, leading to endometriosis and dysmenorrhea. Though the majority of cases of dysmenorrhea in adolescents are primary in nature and require only reassurance and symptomatic management, it is important to be aware of rare causes such as müllerian anomalies so that these cases can be properly managed. Hence, we present this case report, with interesting illustrations, so as to increase awareness regarding these anomalies. Key words: Dysmenorrhea, müllerian anomaly, unicornuate uterus Date of Acceptance: 13-Feb-2011 Introduction department with complaints of severe pain in the lower abdomen during her menses for the last 6 months. Apart Unicornuate uterus with a rudimentary horn is a rare type from severe dysmenorrhea there was no other menstrual of müllerian duct malformation and is the result of defective abnormality. Her vitals and per abdominal examination fusion of the malformed duct with the contralateral duct.[1] findings were normal. Ultrasonography of the abdomen The incidence of unicornuate uterus, although not precisely suggested the possibility of unicornuate uterus with right- known, is estimated at 1/1000 women.[2] A noncommunicating sided hematosalpinx and hematometra; also, the right rudimentary horn with a functional endometrial cavity is rare kidney was not visualized. -

Endometrial Biopsy | Memorial Sloan Kettering Cancer Center
PATIENT & CAREGIVER EDUCATION Endometrial Biopsy This information describes what to expect during and after your endometrial biopsy. About Your Endometrial Biopsy During your endometrial biopsy, your doctor will remove a small piece of tissue from the lining of your uterus. The lining of your uterus is called your endometrium. This tissue is sent to the pathology department to be examined under a microscope. The pathologist will look for abnormal cells or signs of cancer. Before Your Procedure Tell your doctor or nurse if: You’re allergic to iodine. You’re allergic to latex. There’s a chance that you’re pregnant. If you still get your period and are between ages 11 and 50, you will need to take a urine pregnancy test to make sure you’re not pregnant. You won’t need to do anything to get ready for this procedure. During Your Procedure You will have your endometrial biopsy done in an exam room. You will lie on your back as you would for a routine pelvic exam. You will be awake during the procedure. Endometrial Biopsy 1/3 First, your doctor will put a speculum into your vagina. A speculum is a tool that will gently spread apart your vaginal walls, so your doctor can see your cervix (the bottom part of your uterus). Next, your doctor will clean your cervix with a cool, brown solution of povidone- iodine (Betadine® ). Then, they will put a thin, flexible tool, called a pipelle, through your cervix and into your uterus to take a small amount of tissue from your endometrium. -

N35.12 Postinfective Urethral Stricture, NEC, Female N35.811 Other
N35.12 Postinfective urethral stricture, NEC, female N35.811 Other urethral stricture, male, meatal N35.812 Other urethral bulbous stricture, male N35.813 Other membranous urethral stricture, male N35.814 Other anterior urethral stricture, male, anterior N35.816 Other urethral stricture, male, overlapping sites N35.819 Other urethral stricture, male, unspecified site N35.82 Other urethral stricture, female N35.911 Unspecified urethral stricture, male, meatal N35.912 Unspecified bulbous urethral stricture, male N35.913 Unspecified membranous urethral stricture, male N35.914 Unspecified anterior urethral stricture, male N35.916 Unspecified urethral stricture, male, overlapping sites N35.919 Unspecified urethral stricture, male, unspecified site N35.92 Unspecified urethral stricture, female N36.0 Urethral fistula N36.1 Urethral diverticulum N36.2 Urethral caruncle N36.41 Hypermobility of urethra N36.42 Intrinsic sphincter deficiency (ISD) N36.43 Combined hypermobility of urethra and intrns sphincter defic N36.44 Muscular disorders of urethra N36.5 Urethral false passage N36.8 Other specified disorders of urethra N36.9 Urethral disorder, unspecified N37 Urethral disorders in diseases classified elsewhere N39.0 Urinary tract infection, site not specified N39.3 Stress incontinence (female) (male) N39.41 Urge incontinence N39.42 Incontinence without sensory awareness N39.43 Post-void dribbling N39.44 Nocturnal enuresis N39.45 Continuous leakage N39.46 Mixed incontinence N39.490 Overflow incontinence N39.491 Coital incontinence N39.492 Postural -

Sexual Dysfunction in Gynecologic Cancer Patients
WCRJ 2017; 4 (1): e835 SEXUAL DYSFUNCTION IN GYNECOLOGIC CANCER PATIENTS L. DEL PUP Division of Gynecological Oncology, CRO Aviano, National Cancer Institute, Aviano (PN), Italy. Abstract – Objective: Sexual dysfunction is prevalent among gynecologic cancer survivors and strongly impacts on the quality of life (QoL), but the subject is poorly diagnosed and treated. Materials and Methods: A comprehensive literature search of English language studies on sex- ual dysfunctions due to gynecologic cancer treatment has been conducted on MEDLINE databases. Results: Surgery, radiation, and chemotherapy can cause any kind of sexual dysfunction with different mechanisms: psychological and relational, hormonal and pharmacological, neurological and vascular, side effects of chemo and radiation therapies, and direct effects of surgery on sexually involved pelvic organs. Many patients expect their healthcare providers to address sexual health concerns, but most have never discussed sex-related issues with their physician, or they do not re- ceive a proper treatment or referral. This can have medical legal consequences, because it must be discussed and documented before starting treatment. Conclusions: Oncology providers can make a significant impact on the QoL of gynecologic cancer sur- vivors by informing patients and by asking them for sexual health concerns. Counseling is per se beneficial, as it improves QoL. Furthermore, it permits a proper referral and resolution of most symptoms. KEYWORDS: Gynecologic cancer, Sexual dysfunction, Vulvar cancer, Vaginal cancer, Cervical cancer, Endometrial cancer, Ovarian cancer, Ospemifene. INTRODUCTION ly ask about sexual issues, but 64% state that phy- sicians never initiates the conversation during their The proportion of people living with and surviv- care3. ing gynecologic cancer is growing. -

An Unusual Cause of Chronic Low Back Pain
Yunus Durmaz et al. / International Journal Of Advances In Case Reports, 2015;2(23):1425-1426. e - ISSN - 2349 - 8005 INTERNATIONAL JOURNAL OF ADVANCES IN CASE REPORTS Journal homepage: www.mcmed.us/journal/ijacr RETROVERTED UTERUS: AN UNUSUAL CAUSE OF CHRONIC LOW BACK PAIN Yunus Durmaz1, Ilker Ilhanli2*, Kıvanc Cengiz3 1Department of Physical Medicine and Rehabilitation, Division of Rheumatology, Mehmet Akif Inan Training and Research Hospital, Sanlıurfa, Turkey. 2Department of Physical Medicine and Rehabilitation, School of Medicine, University of Giresun, Giresun, Turkey. 3Department of Physical Medicine and Rehabilitation, Division of Rheumatology, Sivas Numune Hospital, Sivas, Turkey. Corresponding Author:- Ilker ILHANLI E-mail: [email protected] Article Info ABSTRACT Received 15/09/2015 Retroverted uterus can be associated with chronic low back pain. Physicians should keep in mind this Revised 27/10/2015 cause of chronic low back pain for the premenopausal women. Here we presented two female patients Accepted 2/11/2015 at the ages of 21 and 28; they were diagnosed as retroverted uterus by Magnetic Resonance Imaging with any other cause of chronic low back pain. Key words: Retroverted uterus; Low back pain; Magnetic resonance imaging. INTRODUCTION Retrovertion is an anatomical variation of the too. She reported any trauma or family history of uterus which can be associated with low back pain, as well spondyloarthropathy. There was no radiculopathy sign or as the chronic pelvic pain. Also it can cause congestive muscle spasm. She didn’t meet the criteria of fibromyalgia. dysmenorrhea, deep dyspareunia, and bladder and bowel Lomber Schober test was normal. Straight leg raising, symptoms [1].