Vaginal and Cesarean Birth: How Do the Risks Compare?
Total Page:16
File Type:pdf, Size:1020Kb

Load more
Recommended publications
-
Rapid Reduction of Maternal Mortality in Uganda and Zambia
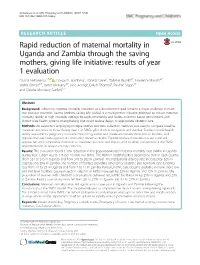
Serbanescu et al. BMC Pregnancy and Childbirth (2017) 17:42 DOI 10.1186/s12884-017-1222-y RESEARCHARTICLE Open Access Rapid reduction of maternal mortality in Uganda and Zambia through the saving mothers, giving life initiative: results of year 1 evaluation Florina Serbanescu1,7,8* , Howard I. Goldberg1, Isabella Danel1, Tadesse Wuhib2,7, Lawrence Marum3,7, Walter Obiero2,7, James McAuley3,7, Jane Aceng4, Ewlyn Chomba5, Paul W. Stupp1,7 and Claudia Morrissey Conlon6,7 Abstract Background: Achieving maternal mortality reduction as a development goal remains a major challenge in most low-resource countries. Saving Mothers, Giving Life (SMGL) is a multi-partner initiative designed to reduce maternal mortality rapidly in high mortality settings through community and facility evidence-based interventions and district-wide health systems strengthening that could reduce delays to appropriate obstetric care. Methods: An evaluation employing multiple studies and data collection methods was used to compare baseline maternal outcomes to those during Year 1 in SMGL pilot districts in Uganda and Zambia. Studies include health facility assessments, pregnancy outcome monitoring, enhanced maternal mortality detection in facilities, and population-based investigation of community maternal deaths. Population-based evaluation used standard approaches and comparable indicators to measure outcome and impact, and to allow comparison of the SMGL implementation in unique country contexts. Results: The evaluation found a 30% reduction in the population-based maternal mortality ratio (MMR) in Uganda during Year 1, from 452 to 316 per 100,000 live births. The MMR in health facilities declined by 35% in each country (from 534 to 345 in Uganda and from 310 to 202 in Zambia). -

Central African Republic
CENTRAL AFRICAN REPUBLIC DEMOGRAPHICS AND BACKGROUND INFORMATION Total population (000) 4,487 (2011) Causes of under-five deaths, 2010 Under-five mortality rate Globally, undernutrition contributes to more than Deaths per 1,000 live births Total under-five population (000) 659 (2011) one third of child deaths 200 Total number of births (000) 156 (2011) Others 15% 169 Under-five mortality rate (per 1,000 live births) 164 (2011) 164 Measles 0% 160 Total number of under-five deaths (000) 25 (2011) Meningitis 2% Neonatal 28% HIV/AIDS 3% 120 Infant mortality rate (per 1,000 live births) 108 (2011) Injuries 3% Neonatal mortality rate (per 1,000 live births) 46 (2011) 80 HIV prevalence rate (15–49 years old, %) 4.6 (2011) 56 Population below international 63 (2008) Malaria 26% 40 MDG 4 poverty line of US$1.25 per day (%) Pneumonia 13% target GNI per capita (US$) 470 (2011) Diarrhoea 10% 0 1990 1995 2000 2005 2010 2015 Primary school net attendance ratio 47, 56 (2006) (% female, % male) Source: WHO/CHERG, 2012. Source: IGME, 2012. NUTRITIONAL STATUS Burden of malnutrition (2011) Stunted (under-fives, 000) 270 MDG 1 progress No progress Stunting country rank 50 Wasted (under-fives, 000) 46 Underweight (under-fives, 000) 158 Share of world stunting burden (%) <1% Severely wasted (under-fives, 000) 13 Overweight (under-fives, 000) 12 Stunting trends Stunting disparities Underweight trends Percentage of children <5 years old stunted Percentage of children <5 years old stunted, Percentage of children <5 years old underweight by selected background characteristics 100% 100% Boys 44 MDG 1: NO PROGRESS Girls 38 80% 80% Urban 38 60% Rural 42 60% 40% 45 Poorest 20% 45 40% 42 43 41 Second 20% 45 Middle 20% 41 20% 20% 26 Fourth 20% 39 24 22 24 Richest 20% 30 0% 0% 1994–1995 2000 2006 2010 0% 20% 40% 60% 80% 100% 1994–1995 2000 2006 2010 DHS MICS MICS MICS DHS MICS MICS MICS Source: MICS, 2010. -

Caesarean Section Or Vaginal Delivery in the 21St Century
CAESAREAN SECTION OR VAGINAL DELIVERY IN THE 21ST CENTURY ntil the 20th Century, caesarean fluid embolism. The absolute risk of trans-placentally to the foetus, prepar- section (C/S) was a feared op- death with C/S in high and middle- ing the foetus to adopt its mother’s Ueration. The ubiquitous classical resource settings is between 1/2000 and microbiome. C/S interferes with neonatal uterine incision meant high maternal 1/4000 (2, 3). In subsequent pregnancies, exposure to maternal vaginal and skin mortality from bleeding and future the risk of placenta previa, placenta flora, leading to colonization with other uterine rupture. Even with aseptic surgi- accreta and uterine rupture is increased. environmental microbes and an altered cal technique, sepsis was common and These conditions increase maternal microbiome. Routine antibiotic exposure lethal without antibiotics. The operation mortality and severe maternal morbid- with C/S likely alters this further. was used almost solely to save the life of ity cumulatively with each subsequent Microbial exposure and the stress of a mother in whom vaginal delivery was C/S. This is of particular importance to labour also lead to marked activation extremely dangerous, such as one with women having large families. of immune system markers in the cord placenta previa. Foetal death and the use blood of neonates born vaginally or by of intrauterine foetal destructive proce- Maternal Benefits C/S after labour. These changes are absent dures, which carry their own morbidity, C/S has a modest protective effect against in the cord blood of neonates born by were often preferable to C/S. -

Maternal Mortality in the United States, 1935 to 2007
Maternal Mortality in the United States, 1935-2007: Substantial Racial/Ethnic, Socioeconomic, and Geographic Disparities Persist Gopal K. Singh, PhD U.S. Department of Health and Human Services Health Resources and Services Administration Maternal and Child Health Bureau Figure 1: Maternal Mortality by Race, United States, Figure 2: Maternal Mortality Rate by Race/Ethnicity, 1935–2007 United States, 2005-2007 Trends in Maternal Mortality by Race Maternal mortality in the United States has declined Maternal deaths are those related to or aggravated by dramatically over the past century (1-4). The rate declined pregnancy or pregnancy management and which occur from 607.9 maternal deaths per 100,000 live births in 1915 during or within 42 days after the end of pregnancy (3). to 12.7 in 2007 (1-3). However, maternal mortality in the Although mortality trend data extend farther back in time United States has changed very little in the past 25 years for the entire United States and the birth registration area (1, 3). Achieving further reductions in the maternal mortality (1, 2), we chose 1935 as the start of the time trend analysis rate is an important public health priority for the nation as since it coincided with the inception of Title V of the Social the rates for certain ethnic minority and socioeconomic Security Act, a national public health legislation aimed at groups remain relatively high (3, 4, 5). A cross-national promoting and improving the health and welfare services comparison of the 2005 statistics by the World Health for all mothers and children. The maternal mortality rates in Organization (WHO) reveals that the U.S. -

Study Guide Medical Terminology by Thea Liza Batan About the Author
Study Guide Medical Terminology By Thea Liza Batan About the Author Thea Liza Batan earned a Master of Science in Nursing Administration in 2007 from Xavier University in Cincinnati, Ohio. She has worked as a staff nurse, nurse instructor, and level department head. She currently works as a simulation coordinator and a free- lance writer specializing in nursing and healthcare. All terms mentioned in this text that are known to be trademarks or service marks have been appropriately capitalized. Use of a term in this text shouldn’t be regarded as affecting the validity of any trademark or service mark. Copyright © 2017 by Penn Foster, Inc. All rights reserved. No part of the material protected by this copyright may be reproduced or utilized in any form or by any means, electronic or mechanical, including photocopying, recording, or by any information storage and retrieval system, without permission in writing from the copyright owner. Requests for permission to make copies of any part of the work should be mailed to Copyright Permissions, Penn Foster, 925 Oak Street, Scranton, Pennsylvania 18515. Printed in the United States of America CONTENTS INSTRUCTIONS 1 READING ASSIGNMENTS 3 LESSON 1: THE FUNDAMENTALS OF MEDICAL TERMINOLOGY 5 LESSON 2: DIAGNOSIS, INTERVENTION, AND HUMAN BODY TERMS 28 LESSON 3: MUSCULOSKELETAL, CIRCULATORY, AND RESPIRATORY SYSTEM TERMS 44 LESSON 4: DIGESTIVE, URINARY, AND REPRODUCTIVE SYSTEM TERMS 69 LESSON 5: INTEGUMENTARY, NERVOUS, AND ENDOCRINE S YSTEM TERMS 96 SELF-CHECK ANSWERS 134 © PENN FOSTER, INC. 2017 MEDICAL TERMINOLOGY PAGE III Contents INSTRUCTIONS INTRODUCTION Welcome to your course on medical terminology. You’re taking this course because you’re most likely interested in pursuing a health and science career, which entails proficiencyincommunicatingwithhealthcareprofessionalssuchasphysicians,nurses, or dentists. -
Maternal Mortality and Morbidity Task Force and DSHS Joint Biennial
Maternal Mortality and Morbidity Task Force and Department of State Health Services Joint Biennial Report As Required by Chapter 34, Texas Health and Safety Code, Section 34.015 Maternal Mortality and Morbidity Task Force September 2018 Table of Contents Executive Summary ............................................................................... 1 1. Introduction ...................................................................................... 2 2. Background ....................................................................................... 3 3. Findings ............................................................................................. 4 I. Findings from Task Force Maternal Death Case Review ........................... 4 II. Findings from Statewide Maternal Death Trend Analysis ......................... 8 Statewide Maternal Death Trends among the Most At-Risk Populations ...... 11 Statewide Trends of Severe Maternal Morbidity ....................................... 12 4. Best Practices and Programs from Other States that Reduced Rates of Pregnancy-Related Deaths .............................................................. 14 5. Recommendations ........................................................................... 15 Conclusion ........................................................................................... 22 List of Acronyms .................................................................................. 23 Appendix A. Task Force Members ........................................................ -
Costing the Three Transformative Results
COSTING THE THREE TRANSFORMATIVE RESULTS Produced by United Nations Population Fund November 2019 The cost of the transformative results UNFPA is committed to achieving by 2030 Ending preventable maternal deaths Ending the unmet need for family planning Ending gender-based violence and all harmful practices, including child marriage and female genital mutilation COSTING THE THREE TRANSFORMATIVE RESULTS COSTING THE THREE TRANSFORMATIVE RESULTS The cost of the transformative results that UNFPA is committed to achieving by 2030 This publication focuses on new research to estimate the costs associated with a programmatic approach and the global cost of achieving these three transformative results by 2030. The costing analysis pertains to the global effort led by UNFPA towards: (a) ending preventable maternal deaths, (b) ending the unmet need for family planning, (c) ending gender-based violence and all harmful practices, including child marriage and female genital mutilation. UNFPA wishes to thank the following researchers who have contributed to this work: Victoria Chou, Johns Hopkins University Neff Walker, Johns Hopkins University John Stover, Avenir Health Rachel Sanders, Avenir Health Nadia Carvalho, Avenir Health William Winfrey, Avenir Health Michelle Weinberger, Avenir Health Bruce Rasmussen, Victoria University Angela Micah, Institute for Health Metrics and Evaluation, University of Washington Joseph L Dieleman, Institute for Health Metrics and Evaluation, University of Washington UNFPA recognizes the contributions of Robert Gustafson of Gustafson Associates in preparing this publication. UNFPA further recognizes the efforts of the following UNFPA colleagues for their inputs in this publication: Howard Friedman, Tharanga Godallage, Charles Katende, Itamar Katz, Marie Anne Luron, and Helena Carvalho Schmidt. The views and opinions in the research articles included within this publication are those of their respective authors and do not necessarily reflect the official policy or position of the United Nations Population Fund. -

Vocabulary: Sharks
Grades 11-12 - Vocabulary: Sharks Dermal Denticles – Tiny tooth-shaped scales that cover a shark’s body. Dermal Denticles have the same structure as teeth - enamel, dentine, pulp, epidermis, and dermis. Counter Shading - Having a dark dorsal or upper side and a lighter colored underside. Lateral Line – A row of sensors used by sharks and other fish, which detect vibrations. Cartilage – The material that makes up a shark’s skeleton (not bone), and is also found in our ears and nose. Basihyal - A sharks tongue, composed of a small piece of cartilage on the bottom of a sharks’ mouth. Carnivore - An animal that eats meat. Megalodon - An ancient shark that lived between 5 and 1.6 million years ago. Serrated Tooth - A tooth with a jagged edge that is used for sawing. Dorsal Fin - Primary fin located on the back of fishes and certain marine mammals. Pectoral Fins - Either of the anterior pairs of fins. Barbels - Sensory projections near the nostrils and mouth of some sharks, i.e. nurse sharks. They are whisker-like feelers used to taste and feel. Gills - Respiratory organs that fish use to absorb oxygen from the water in order to breathe. Snout - The tip of a shark’s head. Pup - A newly born or hatched shark. Claspers - Two finger like projections on the rear underside of male sharks. Ampullae of Lorenzini - Pores scattered about the head of sharks that are filled with a jellylike substance that can sense temperature change and weak electrical impulses given off by sick prey. Fusiform – A streamlined, oval shape body. -

Glossary of Common MCH Terms and Acronyms
Glossary of Common MCH Terms and Acronyms General Terms and Definitions Term/Acronym Definition Accountable Care Organizations that coordinate and provide the full range of health care services for Organization individuals. The ACA provides incentives for providers who join together to form such ACO organizations and who agree to be accountable for the quality, cost, and overall care of their patients. Adolescence Stage of physical and psychological development that occurs between puberty and adulthood. The age range associated with adolescence includes the teen age years but sometimes includes ages younger than 13 or older than 19 years of age. Antepartum fetal Fetal death occurring before the initiation of labor. death Authorization An act of a legislative body that establishes government programs, defines the scope of programs, and sets a ceiling for how much can be spent on them. Birth defect A structural abnormality present at birth, irrespective of whether the defect is caused by a genetic factor or by prenatal events that are not genetic. Cost Sharing The amount an individual pays for health services above and beyond the cost of the insurance coverage premium. This includes co-pays, co-insurance, and deductibles. Crude birth rate Number of live births per 1000 population in a given year. Birth spacing The time interval from one child’s birth until the next child’s birth. It is generally recommended that at least a two-year interval between births is important for maternal and child health and survival. BMI Body mass index (BMI) is a measure of body weight that takes into account height. -

Onychophorology, the Study of Velvet Worms
Uniciencia Vol. 35(1), pp. 210-230, January-June, 2021 DOI: http://dx.doi.org/10.15359/ru.35-1.13 www.revistas.una.ac.cr/uniciencia E-ISSN: 2215-3470 [email protected] CC: BY-NC-ND Onychophorology, the study of velvet worms, historical trends, landmarks, and researchers from 1826 to 2020 (a literature review) Onicoforología, el estudio de los gusanos de terciopelo, tendencias históricas, hitos e investigadores de 1826 a 2020 (Revisión de la Literatura) Onicoforologia, o estudo dos vermes aveludados, tendências históricas, marcos e pesquisadores de 1826 a 2020 (Revisão da Literatura) Julián Monge-Nájera1 Received: Mar/25/2020 • Accepted: May/18/2020 • Published: Jan/31/2021 Abstract Velvet worms, also known as peripatus or onychophorans, are a phylum of evolutionary importance that has survived all mass extinctions since the Cambrian period. They capture prey with an adhesive net that is formed in a fraction of a second. The first naturalist to formally describe them was Lansdown Guilding (1797-1831), a British priest from the Caribbean island of Saint Vincent. His life is as little known as the history of the field he initiated, Onychophorology. This is the first general history of Onychophorology, which has been divided into half-century periods. The beginning, 1826-1879, was characterized by studies from former students of famous naturalists like Cuvier and von Baer. This generation included Milne-Edwards and Blanchard, and studies were done mostly in France, Britain, and Germany. In the 1880-1929 period, research was concentrated on anatomy, behavior, biogeography, and ecology; and it is in this period when Bouvier published his mammoth monograph. -

A B C Pregnancy Terms and Definitions
Pregnancy Terms and Definitions Obstetrics & Gynecology A After pains or afterbirth pains: Contractions of the uterus that occur after your baby is born, as the uterus returns to its normal size. This may cause cramping for a few days, especially if this is not your first baby or if you are nursing. Amniocentesis: the removal of a sample of amniotic fluid by means of a needle inserted through the mother’s abdominal wall; used for genetic and biochemical analysis of the baby. Amniotic fluid: the liquid surrounding and protecting the baby within the amniotic sac throughout pregnancy. Amniotic sac: the membrane within the uterus that contains the baby and the amniotic fluid. Analgesic: Medication that relieves or reduces pain. Anesthesia: Loss of feeling. There are three ways of doing this: general, local and epidural. Anesthesiologist: A doctor who specializes in the use of anesthesia. Anesthetist: A registered nurse who has special training in anesthesia. Apgar score rating: A system to evaluate the health of your baby immediately after birth. The score can be zero to 10, based on appearance and color, pulse, reflexes, activity and respiration. B Baby blues: A mild depression many women feel in the first few weeks after birth. Braxton-Hicks contractions: Mild, usually painless contractions that occur during the entire pregnancy, but are only felt from the 5th month on. Breech birth: Baby is born feet or buttocks first. C Cephalopelvic disproprition (CPD): Baby’s head is too large for the mother’s pelvic bones. Cervix: the neck of the uterus; Pap smears are taken from the cervix. -

Post-Partum Hysterectomy (Removal of the Uterus/Womb After Giving Birth)
Post-partum hysterectomy (removal of the uterus/womb after giving birth) This leaflet explains what happens when a woman needs a post-partum hysterectomy following complications during giving birth. It explains why and how it is done, and what to expect afterwards. If there is anything you do not understand or if you have any questions, please speak to your midwife or doctor. What is post-partum hysterectomy? This is an operation that involves removal of the uterus (womb). This is an uncommon situation in the UK, with around 1 in 1000 women having this procedure done shortly after childbirth in this hospital, as there is a range of treatments used before such surgery which can save both future fertility and the mother’s life. It may be performed in an emergency to save the life of a woman with persistent bleeding after childbirth. Less frequently, it can be a planned procedure, often at the same time as Caesarean birth. Why is it performed? The most common reason is severe bleeding from the uterus that cannot be controlled by other measures. There is a link to Caesarean birth, particularly if the placenta for the most recent baby is both low in the uterus (placenta praevia), and deeply adherent (placenta grows too deeply into the uterine wall, known as placenta percreta or increta), so not separating fully after the birth of the baby. A more common cause of heavy bleeding is ‘uterine atony’, which is the inability of a womb to contract after the birth, as well as large or multiple fibroids and blood clotting problems.