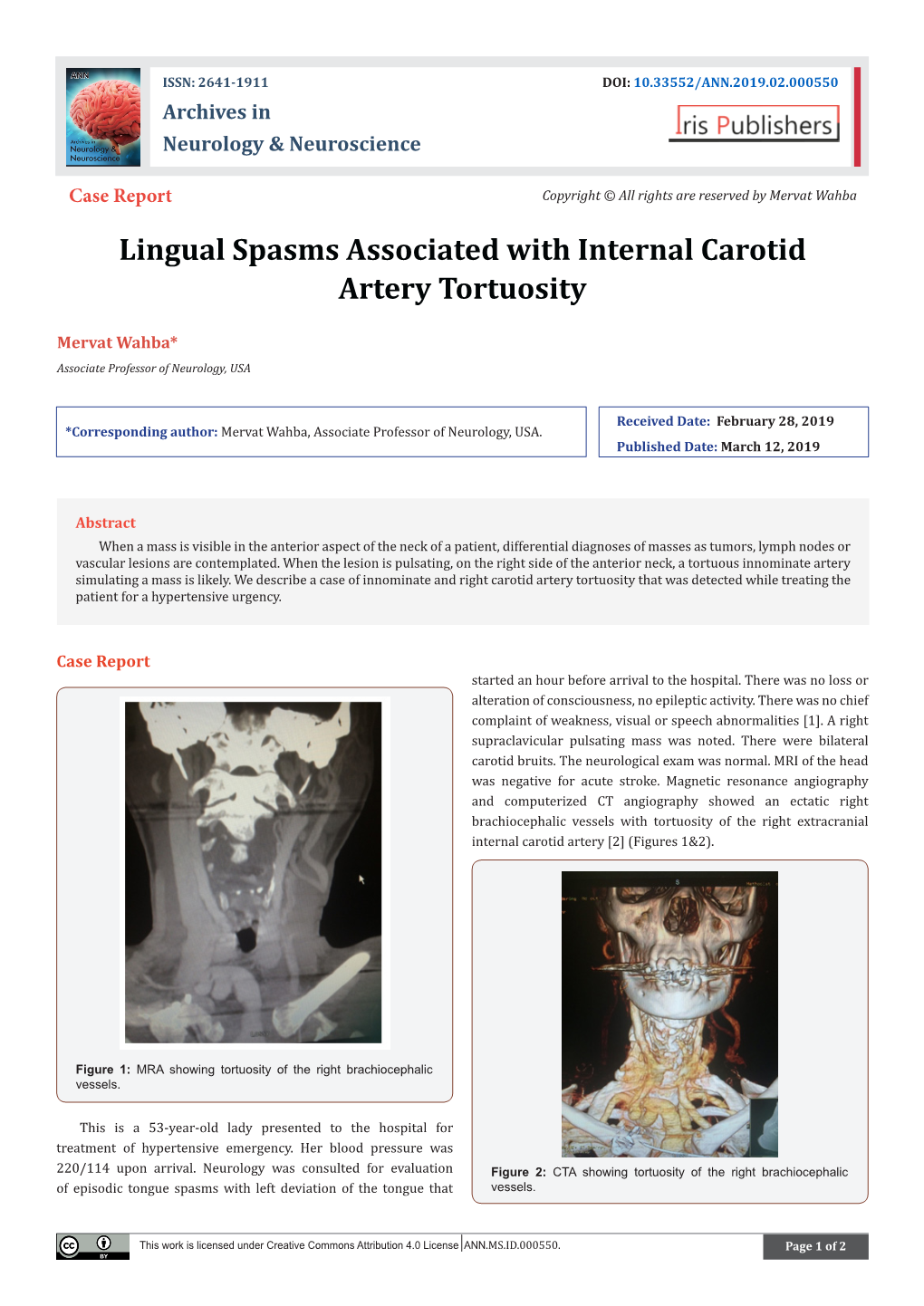
Lingual Spasms Associated with Internal Carotid Artery Tortuosity
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Ascending Pharyngeal Artery Arising from a Hypoplastic Internal Carotid Artery
Published online: 2021-08-09 CASE REPORT Ascending pharyngeal artery arising from a hypoplastic internal carotid artery Charif A. Sidani, Rami Sulaiman1, Amr Rahal2, Danea J. Campbell Department of Radiology, University of Miami Miller School of Medicine, Jackson Memorial Hospital, Miami, Fl 33136, USA, 1 Department of Radiology, Cairo University Faculty of Medicine, Cairo, Egypt, 2 School of Medicine, Saba University School of Medicine, Saba, Dutch Caribbean, Netherlands Access this article online ABSTRACT Website: www.avicennajmed.com DOI: 10.4103/2231-0770.160251 Normal vascular variants often have clinical/surgical significance and can be misinterpreted for Quick Response Code: pathology. We report a case ascending pharyngeal artery arising from a hypoplastic internal carotid artery. We provide clues to differentiate between dysgenesis and disease/thrombosis of the internal carotid artery. Key words: Carotid canal, dysgenesis of internal carotid artery, hypopharyngeal artery, vascular variants INTRODUCTION carotid artery (ECA) as well as the proximal 1 cm of the right ICA. After the normal first centimeter, the ICA became of Dysgenesis of the ICA is a rare developmental anomaly seen in narrow caliber, without evidence of thrombus or dissection, <0.01% of the population.[1,2] The term incorporates agenesis and remained of homogeneous small caliber all the way (no carotid canal or vascular remnant), aplasia (vascular into a hypoplastic carotid canal. Findings confirmed the remnant and hypoplastic carotid canal), or hypoplasia congenital nature of the small ICA [Figure 2]. (small caliber, patent lumen). These abnormalities often have clinical/surgical significance and can be misinterpreted for Arising from the medial aspect of the proximal ICA was pathology. -

Anomalous Origin of the Middle Meningeal Artery
The Internet Journal of Radiology ISPUB.COM Volume 4 Number 2 Anomalous Origin of the Middle Meningeal Artery from the Petrous Segment of the Internal Carotid Artery Associated with Multiple Cerebrovascular Abnormalities I Omeis, M Crupain, M Tenner, R Murali Citation I Omeis, M Crupain, M Tenner, R Murali. Anomalous Origin of the Middle Meningeal Artery from the Petrous Segment of the Internal Carotid Artery Associated with Multiple Cerebrovascular Abnormalities. The Internet Journal of Radiology. 2005 Volume 4 Number 2. Abstract A 25-year-old male with a history of seizure disorder was found incidentally on cerebral angiography to have numerous congenital anomalies of the cerebral vascular system. Among these anomalies were the derivation of the left middle meningeal artery from the petrous portion of the internal carotid artery, the presence of a left cavernous angioma, cavernous origin of the left ophthalmic artery, and an accessory middle cerebral artery. Awareness of cerebral circulatory anatomical anomalies of this nature is of importance to all physicians who plan surgical and endovascular interventions. INTRODUCTION resonance imaging (MRI) with and without gadolinium The middle meningeal artery in most individuals arises from revealed a left temporal lobe cavernoma and associated the maxillary branch of the external carotid artery and enters developmental venous anomaly in the region of the collateral the skull through the foramen spinosum. It then divides into gyrus that were unchanged from of first diagnosis (Fig. 2). anterior and posterior branches to supply the dura and An electroencephalogram (EEG) showed some mild cerebral adjacent calvarium. A few instances have been reported of dysfunction over the left temporal region with no the aberrant origin of the middle meningeal artery from epileptiform abnormality. -

Clinical Importance of the Middle Meningeal Artery
View metadata, citation and similar papers at core.ac.uk brought to you by CORE provided by Jagiellonian Univeristy Repository FOLIA MEDICA CRACOVIENSIA 41 Vol. LIII, 1, 2013: 41–46 PL ISSN 0015-5616 Przemysław Chmielewski1, Janusz skrzat1, Jerzy waloCha1 CLINICAL IMPORTANCE OF THE MIDDLE MENINGEAL ARTERY Abstract: Middle meningeal artery (MMA)is an important branch which supplies among others cranial dura mater. It directly attaches to the cranial bones (is incorporated into periosteal layer of dura mater), favors common injuries in course of head trauma. This review describes available data on the MMA considering its varability, or treats specific diseases or injuries where the course of MMA may have clinical impact. Key words: Middle meningeal artery (MMA), aneurysm of the middle meningeal artery, epidural he- matoma, anatomical variation of MMA. TOPOGRAPHY OF THE MIDDLE MENINGEAL ARTERY AND ITS BRANCHES Middle meningeal artery (MMA) [1] is most commonly the strongest branch of maxillary artery (from external carotid artery) [2]. It supplies blood to cranial dura mater, and through the numerous perforating branches it nourishes also periosteum of the inner aspect of cranial bones. It enters the middle cranial fossa through the foramen spinosum, and courses between the dura mater and the inner aspect of the vault of the skull. Next it divides into two terminal branches — frontal (anterior) which supplies blood to bones forming anterior cranial fossa and the anterior part of the middle cranial fossa; parietal branch (posterior), which runs more horizontally toward the back and supplies posterior part of the middle cranial fossa and supratentorial part of the posterior cranial fossa. -

Venous Arrangement of the Head and Neck in Humans – Anatomic Variability and Its Clinical Inferences
Original article http://dx.doi.org/10.4322/jms.093815 Venous arrangement of the head and neck in humans – anatomic variability and its clinical inferences SILVA, M. R. M. A.1*, HENRIQUES, J. G. B.1, SILVA, J. H.1, CAMARGOS, V. R.2 and MOREIRA, P. R.1 1Department of Morphology, Institute of Biological Sciences, Universidade Federal de Minas Gerais – UFMG, Av. Antonio Carlos, 6627, CEP 31920-000, Belo Horizonte, MG, Brazil 2Centro Universitário de Belo Horizonte – UniBH, Rua Diamantina, 567, Lagoinha, CEP 31110-320, Belo Horizonte, MG, Brazil *E-mail: [email protected] Abstract Introduction: The knowledge of morphological variations of the veins of the head and neck is essential for health professionals, both for diagnostic procedures as for clinical and surgical planning. This study described changes in the following structures: retromandibular vein and its divisions, including the relationship with the facial nerve, facial vein, common facial vein and jugular veins. Material and Methods: The variations of the veins were analyzed in three heads, five hemi-heads (right side) and two hemi-heads (left side) of unknown age and sex. Results: The changes only on the right side of the face were: union between the superficial temporal and maxillary veins at a lower level; absence of the common facial vein and facial vein draining into the external jugular vein. While on the left, only, it was noted: posterior division of retromandibular, after unite with the common facial vein, led to the internal jugular vein; union between the posterior auricular and common facial veins to form the external jugular and union between posterior auricular and common facial veins to terminate into internal jugular. -

A Rare Case of Collett–Sicard Syndrome After Blunt Head Trauma
Case Report Dysphagia and Tongue Deviation: A Rare Case of Collett–Sicard Syndrome after Blunt Head Trauma Eric Tamrazian 1,2 and Bijal Mehta 1,2,* 1 Department of Neurology, David Geffen School of Medicine, Harbor-UCLA Medical Center, Torrance, CA 90502, USA; [email protected] 2 Los Angeles Biomedical Institute, Los Angeles, CA 90095, USA * Correspondence: [email protected] Received: 28 October 2019; Accepted: 14 November 2019; Published: 21 December 2020 Abstract: The jugular foramen and the hypoglossal canal are both apertures located at the base of the skull. Multiple lower cranial nerve palsies tend to occur with injuries to these structures. The pattern of injuries tend to correlate with the combination of nerves damaged. Case Report: A 28-year-old male was involved in an AVP injury while crossing the highway. Exam showed a GCS of 15 AAOx3, with dysphagia, tongue deviation to the right, uvula deviation to the left and a depressed palate. Initial imaging showed B/L frontal traumatic Sub-Arachnoid Hemorrhages (tSAH), Left Frontal Epidural Hematoma and a Basilar Skull Fracture. On second look by a trained Neuroradiologist c At 3 month follow up, patient’s tongue normalized to midline and his dysphagia resolved. Discussion: Collette-Sicard syndrome is a rare condition/syndrome characterized by unilateral palsy of CN: IX, X, XII. This condition has been rarely described as a consequence of blunt head trauma. In most cases, the condition is self-limiting with patients regaining most to all of their neurological functions within 6 months. Nerve traction injuries and soft tissue edema compressing the cranial nerves are the leading two hypothesis. -

The Hemodynamic Effect of Unilateral Carotid Ligation on the Cerebral Circulation of Man*
THE HEMODYNAMIC EFFECT OF UNILATERAL CAROTID LIGATION ON THE CEREBRAL CIRCULATION OF MAN* HENRY A. SHENKIN, M.D., FERNANDO CABIESES, M.D., GORDON VAN DEN NOORDT, M.D., PETER SAYERS, M.D., AND REUBEN COPPERMAN, M.A. Neurosurgical Service, Graduate Hospital, and Harrison Department of Surgical Re- search, Schools of Medicine, University of Pennsylvania, Philadelphia (Received for publication July ~5, 1950) HE increasing incidence of surgical attack upon vascular anomalies of the brain has renewed interest in the physiological responses of the T cerebral circulation to occlusion of a carotid vessel. This question has been studied in lower animals by Rein, 5 the Schneiders, 6 Bouckaert and Heymans 1 and by the late Cobb Pilcher. 4 However, because of the lack of an adequate technique for measuring the cerebral blood flow and because of the fact that lower animals have a rich intercommunication between the intracerebral and extracerebral circulations, very few data pertinent to human physiology have been accumulated. There are two important points to be established concerning carotid ligation: firstly, its therapeutic effect, that is the degree of fall of pressure in the vessels distal to the ligation, and secondly, its safety, determined by its effect on the cerebral blood flow. Sweet and Bennett, 8 by careful measurement of pressure changes distal to ligation, have provided informa- tion on the former point. It is the latter problem that is the subject of this paper. METHODS The subjects of this study were 4 patients with intracranial arterial aneurysms subjected to unilateral common carotid artery ligation. They ranged in age from 15 to 53 years (Table 1). -

Axis Scientific Human Circulatory System 1/2 Life Size A-105864
Axis Scientific Human Circulatory System 1/2 Life Size A-105864 05. Superior Vena Cava 13. Ascending Aorta 21. Hepatic Vein 28. Celiac Trunk II. Lung 09. Pulmonary Trunk 19. Common III. Spleen Hepatic Artery 10. Pulmonary 15. Pulmonary Artery 17. Splenic Artery (Semilunar) Valve 20. Portal Vein 03. Left Atrium 18. Splenic Vein 01. Right Atrium 16. Pulmonary Vein 26. Superior 24. Superior 02. Right Ventricle Mesenteric Vein Mesenteric Artery 11. Supraventricular Crest 07. Interatrial Septum 22. Renal Artery 27. Inferior 14. Aortic (Semilunar) Valve Mesenteric Vein 08. Tricuspid (Right 23. Renal Vein 12. Mitral (Left Atrioventricular) Valve VI. Large Intestine Atrioventricular) Valve 29. Testicular / 30. Common Iliac Artery Ovarian Artery 32. Internal Iliac Artery 25. Inferior 31. External Iliac Artery Mesenteric Artery 33. Median Sacral Artery 41. Posterior Auricular Artery 57. Deep Palmar Arch 40. Occipital Artery 43. Superficial Temporal Artery 58. Dorsal Venous Arch 36. External Carotid Artery 42. Maxillary Artery 56. Superficial Palmar Arch 35. Internal Carotid Artery 44. Internal Jugular Vein 39. Facial Artery 45. External Jugular Vein 38. Lingual Artery and Vein 63. Deep Femoral Artery 34. Common Carotid Artery 37. Superior Thyroid Artery 62. Femoral Artery 48. Thyrocervical Trunk 49. Inferior Thyroid Artery 47. Subclavian Artery 69. Great Saphenous Vein 46. Subclavian Vein I. Heart 51. Thoracoacromial II. Lung Artery 64. Popliteal Artery 50. Axillary Artery 03. Left Atrium 01. Right Atrium 04. Left Ventricle 02. Right Ventricle 65. Posterior Tibial Artery 52. Brachial Artery 66. Anterior Tibial Artery 53. Deep Brachial VII. Descending Artery Aorta 70. Small Saphenous Vein IV. Liver 59. -

Papillary Thyroid Carcinoma
CASE REPORT Papillary Thyroid Carcinoma: The First Case of Direct Tumor Extension into the Left Innominate Vein Managed with a Single Operative Approach Douglas J Chung1, Diane Krieger2, Niberto Moreno3, Andrew Renshaw4, Rafael Alonso5, Robert Cava6, Mark Witkind7, Robert Udelsman8 ABSTRACT Aim: The aim of this study is to report a case of papillary thyroid carcinoma (PTC) with direct intravascular extension into the left internal jugular vein, resulting in tumor thrombus into the left innominate vein. Background: PTC is the most common of the four histological subtypes of thyroid malignancies,1 but PTC with vascular invasion into major blood vessels is rare.2 The incidence of PTC tumor thrombi was found to be 0.116% in one study investigating 7,754 thyroid surgical patients, and, of these patients with tumor thrombus, none extended more distal than the internal jugular vein.3 Koike et al.4 described a case of PTC invasion into the left innominate vein that was managed by a two-stage operative approach. Case description: A 58-year-old male presented with a rapidly growing left thyroid mass. Fine needle aspiration cytology (FNAC) suggested PTC and surgical exploration confirmed tumor extension into the left internal jugular vein. Continued dissection revealed a large palpable intraluminal tumor thrombus extending below the clavicle into the mediastinum, necessitating median sternotomy. Conclusion: Aggressive one-stage surgical resection resulted in successful en bloc extirpation of the tumor, with negative margins. Follow-up at 22 months postoperatively demonstrated no evidence of recurrence. Clinical significance: This is the first case of PTC extension into the left innominate vein managed with one-stage surgical intervention with curative intent. -

The Ascending Pharyngeal Artery: a Collateral Pathway in Complete
AJNR :8, January/February 1987 CORRESPONDENCE 177 cavernous sinuses acute inflammation, granulation tissue, and throm which it partiCipates. This report describes two cases in which bus surrounded the nerves and internal carotid arteries. The left common carotid angiography showed complete occlu sion of the carotid artery was intact, but focally inflammed. The right internal internal carotid artery at its origin. Subsequent vertebral angiography carotid artery was focally necrotic, acutely inflammed and ruptured, in both cases showed reconstitution of thi s vessel several millimeters with hemorrhage emanating from the defect. above the origin by the ascending ph aryngeal artery , which had an unusual origin from the internal carotid artery [2]. Endarterectomy as a technical option was feasible in both cases becau se the occluded Discussion segments were only millimeters in length . The first patient, a 59-year-old man , presented 5 days before We are not aware of any instances of air within the cavernous admission with a sudden pareS is of the right arm and leg. Angiograph y sinus in a normal patient or after trauma. Our case demonstrates revealed complete occlusion of the left internal carotid artery with a several of the reported findings in cavernous sinus thrombosis includ small , smooth stump (Fig. 1 A) . A left vertebral arteriogram demon ing bulging of the lateral walls , irregular low-attenuation filling defects strated reconstitution of the left internal carotid artery just above the within the cavernous sinus, and proptosis (Fig . 1). occlusion (Fig . 1 B). Collateral supply was from mu scular branches of It is unclear whether the air within the sinus originated from a gas the vertebral artery, which anastomosed with muscular branches of forming organism or via direct extension from one of the sinuses via the ascending pharyngeal artery. -
Anatomical Considerations of the Superior Thyroid Artery: Its Origins, Variations, and Position Relative to the Hyoid Bone and Thyroid Cartilage
Original Article http://dx.doi.org/10.5115/acb.2016.49.2.138 pISSN 2093-3665 eISSN 2093-3673 Anatomical considerations of the superior thyroid artery: its origins, variations, and position relative to the hyoid bone and thyroid cartilage Sung-Yoon Won Department of Occupational Therapy, Semyung University, Jecheon, Korea Abstract: The aim of this study was to provide accurate anatomical descriptions of the overall anatomy of the superior thyroid artery (STA), its relationship to other structures, and its driving patterns. Detailed dissection was performed on thirty specimens of adult’s cadaveric neck specimens and each dissected specimen was carefully measured the following patterns and distances using digital and ruler. The superior thyroid, lingual, and facial arteries arise independently from the external carotid artery (ECA), but can also arise together, as the thyrolingual or linguofacial trunk. We observed that 83.3% of STAs arose independently from the major artery, while 16.7% of the cases arose from thyrolingual or linguofacial trunk. We also measured the distance of STA from its major artery. The origin of the STA from the ECA was 0.9±0.4 mm below the hyoid bone. The STA was 4.4±0.5 mm distal to the midline at the level of the laryngeal prominence and 3.1±0.6 mm distal to the midline at the level of the inferior border of thyroid cartilage. The distance between STA and the midline was similar at the level of the hyoid bone and the thyroid cartilage. Also, when the STA is near the inferior border of the thyroid cartilage, it travels at a steep angle to the midline. -

Lingual Perimandibular Vessels Associated with Life-Threatening Bleeding: an Anatomic Study
Mardinger.qxd 1/25/07 2:55 PM Page 127 Lingual Perimandibular Vessels Associated with Life-Threatening Bleeding: An Anatomic Study Ofer Mardinger, DMD1/Yifat Manor, DMD2/Eitan Mijiritsky, DMD3/Abraham Hirshberg, MD, DMD4 Purpose: To describe the anatomy of the lingual perimandibular vessels and emphasize the distance to the bone. Materials and Methods: The hemifacial lower third was dissected in 12 human cadavers. The blood vessels in the floor of the mouth were exposed using sagittal incisions at the canine, mental foramen, and second molar areas. Results: The diameter of the dissected vessels ranged from 0.5 to 3 mm (mean, 1.5 mm). Most vessels were found superior to the mylohyoid muscle in the canine area and beneath the muscle in the mental and second molar areas. The smallest median vertical distance from blood vessel to bone was in the canine area (14.5 mm), followed by the mental foramen area (15.5 mm) and the second premolar area (19 mm). The median horizontal distance of the vessels from the lingual plate was 2 mm at the canine and second molar areas and 4 mm at the mental area. Discussion: Lingual plate perforation, especially anterior to the canine area, can easily injure blood vessels in the floor of the mouth and cause life-threatening hemorrhage following implant placement. Bleeding can occur when the mandibular lingual plate is perforated. Care should be taken to recognize situations where this complication may occur. Conclusions: Based on the study of human cadavers, it appears that vessels in the floor of the mouth are sometimes in close proximity to the site of implant placement. -

Branches of the External Carotid Artery of the Dromedary, Camelus Dromedarius Artery Origin Course Distribution
Table 3.4: Branches of the External Carotid Artery of the Dromedary, Camelus dromedarius Artery Origin Course Distribution Originates at the bifurcatio of the occipital artery from the common carotid artery. Superficial Occipital region, lateral face, pharynx, Common Carotid External Carotid course is throughout occipital and posteroinferior tongue, hyoid musculature, and Artery facial regions; deeper course is throughout sublingual glands. pharyngeal, lingual, and hyoid regions. The proper occipital artery is the first dorsal branch of the ECA. It arises near the caudal border of the wing of the atlas, traverses the atlantal fossa, and then splits into: 1. Multitude External Carotid of muscular branches; 2. Anastomosis with Collateral circulation with vertebral Occipital Artery vertebral artery (through alar foramen); 3. arteries; neck and occipital muscles Superior termination continues to course toward the external occipital protuberance, supplying the parenchyma of the occipital region inferior to and surrounding the foramen magnum. Variable origin: from the ECA or the "ascending pharyngeal." Condylar and ascending pharyngeal External Carotid may share a short common trunk. An anterior Artery (var: branch of the condylar artery follows the Inferior meninges and inferolateral Condylar Ascending hypoglossal nerve into the hypoglossal canal to occipital region. Pharyngeal) supply the inferior meninges. A posterior branch of the condylar provides collateral circulation to the occipital region. External Carotid Small, tortuous division from medial wall of Cranial Thyroid Thyroid Artery ECA From posteromedial surface of ECA Descending External Carotid immediately posterior to the jugular process. Extensive distribution throughout the Pharyngeal Artery Convoluted and highly dendritic throughout the pharynx lateral and posterior wall of the pharynx.