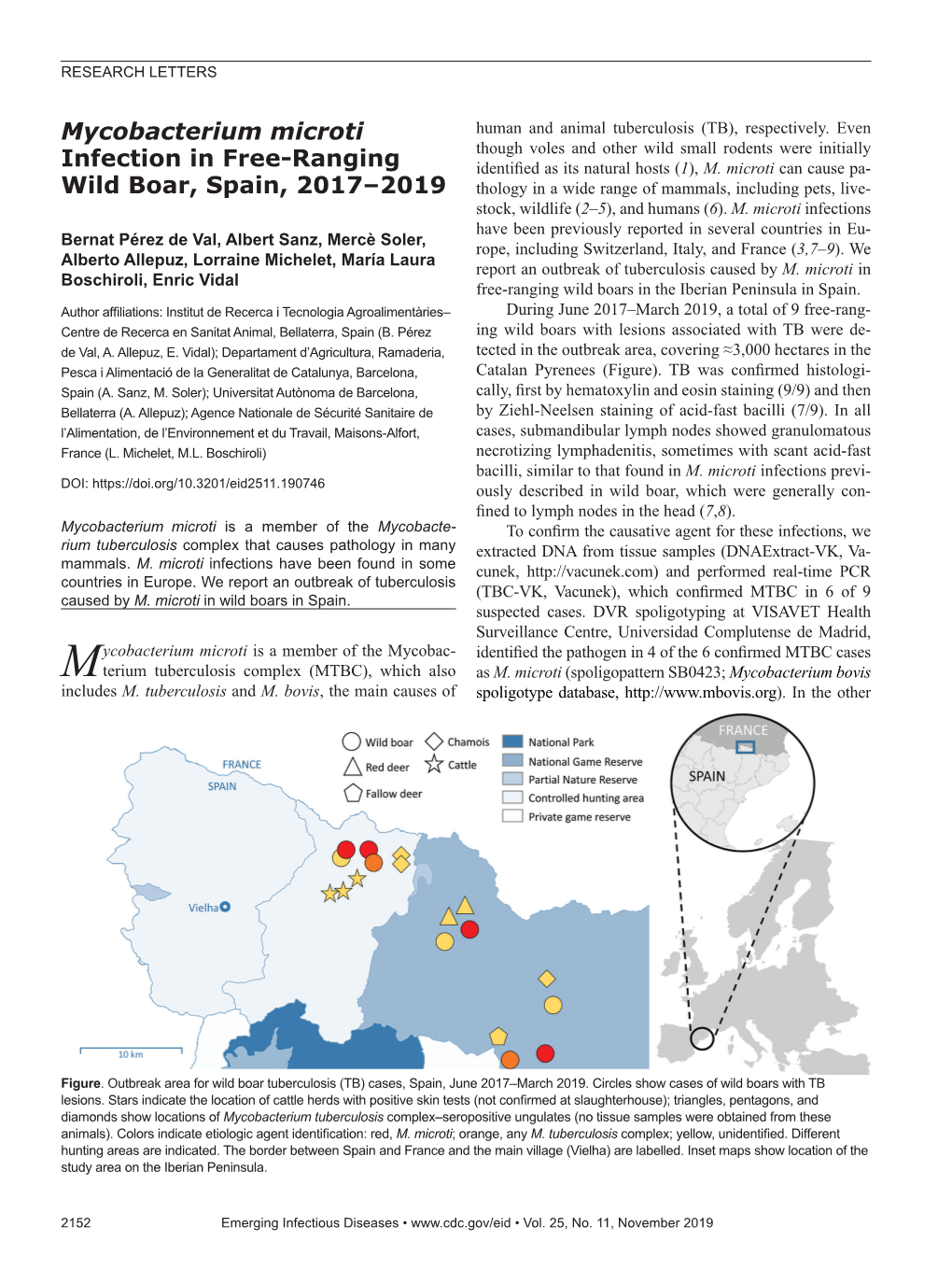
Mycobacterium Microti Human and Animal Tuberculosis (TB), Respectively
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Basic Biology and Applications of Actinobacteria
Edited by Shymaa Enany Basic Biology and Applications of ActinobacteriaBasic of Biology and Applications Actinobacteria have an extensive bioactive secondary metabolism and produce a huge Basic Biology and amount of naturally derived antibiotics, as well as many anticancer, anthelmintic, and antifungal compounds. These bacteria are of major importance for biotechnology, medicine, and agriculture. In this book, we present the experience of worldwide Applications of Actinobacteria specialists in the field of Actinobacteria, exploring their current knowledge and future prospects. Edited by Shymaa Enany ISBN 978-1-78984-614-0 Published in London, UK © 2018 IntechOpen © PhonlamaiPhoto / iStock BASIC BIOLOGY AND APPLICATIONS OF ACTINOBACTERIA Edited by Shymaa Enany BASIC BIOLOGY AND APPLICATIONS OF ACTINOBACTERIA Edited by Shymaa Enany Basic Biology and Applications of Actinobacteria http://dx.doi.org/10.5772/intechopen.72033 Edited by Shymaa Enany Contributors Thet Tun Aung, Roger Beuerman, Oleg Reva, Karen Van Niekerk, Rian Pierneef, Ilya Korostetskiy, Alexander Ilin, Gulshara Akhmetova, Sandeep Chaudhari, Athumani Msalale Lupindu, Erasto Mbugi, Abubakar Hoza, Jahash Nzalawahe, Adriana Ribeiro Carneiro Folador, Artur Silva, Vasco Azevedo, Carlos Leonardo De Aragão Araújo, Patricia Nascimento Da Silva, Jorianne Thyeska Castro Alves, Larissa Maranhão Dias, Joana Montezano Marques, Alyne Cristina Lima, Mohamed Harir © The Editor(s) and the Author(s) 2018 The rights of the editor(s) and the author(s) have been asserted in accordance with the Copyright, Designs and Patents Act 1988. All rights to the book as a whole are reserved by INTECHOPEN LIMITED. The book as a whole (compilation) cannot be reproduced, distributed or used for commercial or non-commercial purposes without INTECHOPEN LIMITED’s written permission. -

Phylogenomic Analysis of the Species of the Mycobacterium Tuberculosis
Phylogenomic analysis of the species of the Mycobacterium tuberculosis complex demonstrates that Mycobacterium africanum, Mycobacterium bovis, Mycobacterium caprae, Mycobacterium microti and Mycobacterium pinnipedii are later heterotypic synonyms of Mycobacterium tuberculosis Marco Riojas, Katya Mcgough, Cristin Rider-Riojas, Nalin Rastogi, Manzour Hernando Hazbón To cite this version: Marco Riojas, Katya Mcgough, Cristin Rider-Riojas, Nalin Rastogi, Manzour Hernando Hazbón. Phy- logenomic analysis of the species of the Mycobacterium tuberculosis complex demonstrates that My- cobacterium africanum, Mycobacterium bovis, Mycobacterium caprae, Mycobacterium microti and Mycobacterium pinnipedii are later heterotypic synonyms of Mycobacterium tuberculosis. Inter- national Journal of Systematic and Evolutionary Microbiology, Microbiology Society, 2018, 68 (1), pp.324-332. 10.1099/ijsem.0.002507. pasteur-01986654 HAL Id: pasteur-01986654 https://hal-riip.archives-ouvertes.fr/pasteur-01986654 Submitted on 18 Jan 2019 HAL is a multi-disciplinary open access L’archive ouverte pluridisciplinaire HAL, est archive for the deposit and dissemination of sci- destinée au dépôt et à la diffusion de documents entific research documents, whether they are pub- scientifiques de niveau recherche, publiés ou non, lished or not. The documents may come from émanant des établissements d’enseignement et de teaching and research institutions in France or recherche français ou étrangers, des laboratoires abroad, or from public or private research centers. publics ou privés. RESEARCH ARTICLE Riojas et al., Int J Syst Evol Microbiol 2018;68:324–332 DOI 10.1099/ijsem.0.002507 Phylogenomic analysis of the species of the Mycobacterium tuberculosis complex demonstrates that Mycobacterium africanum, Mycobacterium bovis, Mycobacterium caprae, Mycobacterium microti and Mycobacterium pinnipedii are later heterotypic synonyms of Mycobacterium tuberculosis Marco A. -

Mycobacterium Microti Interferes with Bovine Tuberculosis Surveillance
microorganisms Communication Mycobacterium microti Interferes with Bovine Tuberculosis Surveillance Lorraine Michelet , Krystel de Cruz, Jennifer Tambosco, Sylvie Hénault and Maria Laura Boschiroli * Laboratory for Animal Health, University Paris-Est, Tuberculosis National Reference Laboratory, ANSES, 94701 Maisons-Alfort, France; [email protected] (L.M.); [email protected] (K.d.C.); [email protected] (J.T.); [email protected] (S.H.) * Correspondence: [email protected] Received: 2 November 2020; Accepted: 23 November 2020; Published: 24 November 2020 Abstract: Mycobacterium microti, a member of the Mycobacterium tuberculosis complex, was originally described as the cause of tuberculosis in wild rodents. However, in the last few years, an increasing number of cases have been reported in wildlife (wild boars and badgers) and livestock (goat and cattle) in the frame of bovine tuberculosis (bTB) surveillance program, demonstrating the risk of interference with bTB diagnosis in France. In 2019, we detected four cattle infected with M. microti, from three different herds in three different distant regions. For all these cases, ante-mortem diagnosis by the skin test (single intradermal comparative cervical tuberculin (SICCT)) was positive. Confirmation of M. microti infection was based on molecular tests, i.e., specific real-time PCR and spoligotyping. These results highlight a non-negligible risk of interference in the bTB diagnosis system and raise concern about the reliability of diagnostic tests used for bTB surveillance. The use of highly specific tests, like the interferon gamma test (IFN-γ) employed in France or new synthetic specific tuberculins for skin testing could alternatively be used to accurately identify M. -

Ecotypes of the Mycobacterium Tuberculosis Complex
Journal of Theoretical Biology Volume 239, Issue 2 , 21 March 2006, Pages 220-225 Special Issue in Memory of John Maynard Smith doi:10.1016/j.jtbi.2005.08.036 Crown copyright © 2005 Published by Elsevier Ltd. Ecotypes of the Mycobacterium tuberculosis complex Noel H. Smitha,* , Kristin Kremerb, Jacqueline Inwalda, James Dalea, Jeffrey R. Driscollc, Stephen V. Gordona, Dick van Soolingenb, R. Glyn Hewinsona and John Maynard Smith aTB Research Group, Veterinary Laboratories Agency (VLA), Weybridge, New Haw, Addlestone, Surrey KT15 3NB, UK bNational Institute of Public Health and the Environment (RIVM), P.O. Box 1, 3720 BA, Bilthoven, The Netherlands cWadsworth Center, New York State Department of Health, P.O. Box 22002, New Scotland Avenue, Albany, NY 12201-2002, USA * Corresponding author. Tel.: +44 1273 873502; fax: +44 1273 678433. Deceased. Abstract A phylogeny of the Mycobacterium tuberculosis complex has recently shown that the animal-adapted strains are found in a single lineage marked by the deletion of chromosomal region 9 (RD9) [Brosch et al., 2002. A new evolutionary scenario for the Mycobacterium tuberculosis complex. Proc. Natl Acad. Sci. USA 99 (6), 3684œ3689]. We have obtained the spoligotype patterns of the RD9 deleted strains used to generate this new evolutionary scenario and we show that the presence of spoligotype spacers 3, 9, 16, 39, and 40œ43 is phylogenetically informative in this lineage. We have used the phylogenetically informative spoligotype spacers to screen a database of spoligotype patterns and have identified further members of a group of strains apparently host-adapted to antelopes. The presence of the spoligotype spacers is congruent with the phylogeny generated by chromosomal deletions, suggesting that recombination is rare or absent between strains of this lineage. -

Zoonotic Tuberculosis in Mammals, Including Bovine and Caprine
Zoonotic Importance Several closely related bacteria in the Mycobacterium tuberculosis complex Tuberculosis in cause tuberculosis in mammals. Each organism is adapted to one or more hosts, but can also cause disease in other species. The two agents usually found in domestic Mammals, animals are M. bovis, which causes bovine tuberculosis, and M. caprae, which is adapted to goats but also circulates in some cattle herds. Both cause economic losses including in livestock from deaths, disease, lost productivity and trade restrictions. They can also affect other animals including pets, zoo animals and free-living wildlife. M. bovis Bovine and is reported to cause serious issues in some wildlife, such as lions (Panthera leo) in Caprine Africa or endangered Iberian lynx (Lynx pardinus). Three organisms that circulate in wildlife, M. pinnipedii, M. orygis and M. microti, are found occasionally in livestock, Tuberculosis pets and people. In the past, M. bovis was an important cause of tuberculosis in humans worldwide. It was especially common in children who drank unpasteurized milk. The Infections caused by advent of pasteurization, followed by the establishment of control programs in cattle, Mycobacterium bovis, have made clinical cases uncommon in many countries. Nevertheless, this disease is M. caprae, M. pinnipedii, still a concern: it remains an important zoonosis in some impoverished nations, while wildlife reservoirs can prevent complete eradication in developed countries. M. M. orygis and M. microti caprae has also emerged as an issue in some areas. This organism is now responsible for a significant percentage of the human tuberculosis cases in some European countries where M. bovis has been controlled. -

Glossery of Tb Terms Acid-Fast Bacilli- (Afb)
GLOSSERY OF TB TERMS ACID-FAST BACILLI - (AFB) Bacteria which retain certain dyes even when washed with an acid solution. Only rarely are acid-fast bacteria which are seen on smear not mycobacteria. A presumptive diagnosis of tuberculosis is often made on the basis of a positive “AFB smear;” however, the diagnosis is not confirmed until a culture is grown and identified as M. tuberculosis . ACQUIRED DRUG RESISTANCE - Resistance to one or more antituberculous drugs which develops while a patient is on therapy, usually the result of erratic compliance on the part of the patient. ADVERSE REACTIONS - Any undesirable effect of a medication. All drugs may cause such reactions, so that periodic monitoring of tuberculous patients under treatment is necessary to detect any that do occur, even though their occurrence may be common. ALVEOLI - The small air sacs in the lungs which lie at the end of the bronchial tree. The site of gas exchange in the lungs, and the site where tuberculous infection usually begins. ANEMIA - A condition in which there is a decreased volume of red cells in the blood. There are many causes for anemia, including chronic infections such as untreated tuberculosis. ANOREXIA - Loss of appetite. Symptom frequently seen in many illnesses, including tuberculosis. ATTENUATED - Refers to the weakened ability of an infectious agent to cause disease . For example, BCG is an attenuated strain of Mycobacterium bovis . BACTERICIDAL - Capable of killing bacteria. Isoniazid and rifampin are the two most potent bactericidal antituberculous drugs. BACTERIOLOGICAL SPECIMEN - Refers to any body fluid, secretion, or tissue sent to the laboratory where smears and cultures for tubercle bacilli will be performed. -

Mycobacterium Microti Infections in Free-Ranging Red Deer (Cervus Elaphus) Giovanni Ghielmetti, Anne M
SYNOPSIS Mycobacterium microti Infections in Free-Ranging Red Deer (Cervus elaphus) Giovanni Ghielmetti, Anne M. Kupca, Matthias Hanczaruk, Ute Friedel, Hubert Weinberger, Sandra Revilla-Fernández, Erwin Hofer, Julia M. Riehm, Roger Stephan, Walter Glawischnig (Sorex araneus), are considered to be primary reservoirs Infections with Mycobacterium microti, a member of the M. tuberculosis complex, have been increasingly reported in for M. microti, several other hosts have been identifi ed, humans and in domestic and free-ranging wild animals. At including domestic and wild animals (3,4). Overall, cats postmortem examination, infected animals may display his- (5,6), New World camelids (7), and free-ranging wild topathologic lesions indistinguishable from those caused by boar (8–10) seem to be prone to M. microti infections; hu- M. bovis or M. caprae, potentially leading to misidentifi ca- mans (11–14) and other animal species, including pigs tion of bovine tuberculosis. We report 3 cases of M. microti (15), goats (16), cattle (17,18), dogs (19), captive meerkats infections in free-ranging red deer (Cervus elaphus) from (20), squirrel monkeys (21), and ferrets (14), are most western Austria and southern Germany. One diseased ani- likely incidental hosts. mal displayed severe pyogranulomatous pleuropneumonia This broad host range, however, highlights the and multifocal granulomas on the surface of the pericardi- pathogenic potential of M. microti and the need to um. Two other animals showed alterations of the lungs and reveal its virulence mechanisms. Comparative ge- associated lymph nodes compatible with parasitic infesta- tion. Results of the phylogenetic analysis including multiple nomics studies have identifi ed >100 genes whose animal strains from the study area showed independent presence are facultative and differ among members infection events, but no host-adapted genotype. -

Mycobacterial Panniculitis Caused by Mycobacterium Thermoresistibile In
JOR0010.1177/2055116916672786Journal of Feline Medicine and Surgery Open ReportsVishkautsan et al 672786research-article2016 Case Report Journal of Feline Medicine and Surgery Open Reports Mycobacterial panniculitis caused 1 –7 © The Author(s) 2016 Reprints and permissions: by Mycobacterium thermoresistibile sagepub.co.uk/journalsPermissions.nav DOI: 10.1177/2055116916672786 in a cat jfmsopenreports.com This paper was handled and processed by the American Editorial Office (AAFP) for publication in JFMS Open Reports Polina Vishkautsan1, Krystle L Reagan1, M Kevin Keel2 and Jane E Sykes3 Abstract Case summary A domestic shorthair cat was evaluated for chronic, bilateral, ulcerative dermatitis affecting the inguinal region and lateral aspects of both pelvic limbs. Histopathologic examination of skin biopsies collected throughout the course of disease revealed chronic pyogranulomatous ulcerative dermatitis. Aerobic bacterial skin cultures yielded growth of a methicillin-resistant Staphylococcus aureus and Corynebacterium amycolatum. Upon referral the clinical findings were suggestive of a non-tuberculous Mycobacterium species infection. Previously obtained skin cultures failed to yield growth of mycobacterial organisms. A deep skin biopsy was collected and submitted for mycobacterial culture. At 5 weeks of incubation Mycobacterium thermoresistibile was isolated. In previous reports, M thermoresistibile has been isolated after 2–4 days of incubation, suggesting that this strain may have been a slower growing variant, or other factors (such as prior antimicrobial therapy) inhibited rapid growth of this isolate. The cat was hospitalized for intravenous antibiotic therapy, surgical debridement of wounds, vacuum-assisted wound closure therapy and reconstruction procedures. The wounds were ultimately primarily closed and the cat was discharged to the owner after 50 days of hospitalization. -

Mycobacterial Genomes 151
Mycobacterial Genomes 151 9 Mycobacterial Genomes David C. Alexander and Jun Liu Summary Tuberculosis (TB), caused by Mycobacterium tuberculosis, remains a major cause of death around the world. Diseases caused by nontuberculous mycobacteria are increasingly associated with immuno- compromised individuals. The availability of whole-genome sequences of mycobacterial species in the past several years has revolutionized TB research. This chapter provides an overview of the biol- ogy of mycobacteria and the diseases that they cause, with emphasis on how recent advances in geno- mics have improved our knowledge of the lifestyle and phylogeny of these organisms. Key Words: Mycobacterial genomes; Mycobacterium tuberculosis; Mycobacteria. “If one judges of the importance of a disease according to its distribution, and accord- ing to the degree in which it menaces health and induces death prematurely, tuberculosis assumes the first rank in human pathology...it has been known as far back as the memory of man extends, and has unceasingly decimated the race for hundreds and thousands of years,” (1) Prof. Dr. Georg Cornet, 1904 (19th century Bacteriologist) 1. Introduction One hundred years later, mycobacterial diseases retain their first rank as menaces to human and animal health. Despite global initiatives and five decades of chemothera- peutics, tuberculosis (TB) caused by Mycobacterium tuberculosis remains a common bacterial disease. An estimated 2 billion people are infected with M. tuberculosis and 2 million succumb to TB each year (2). Leprosy, caused by Mycobacterium leprae, inflicts disfigurement and untold human suffering. Effective treatments for leprosy are avail- able, but attempts at eradication have failed, and more than 600,000 new cases are reported each year (3). -
The Impact of Chlorine and Chloramine on the Detection and Quantification of Legionella Pneumophila and Mycobacterium Spp
The impact of chlorine and chloramine on the detection and quantification of Legionella pneumophila and Mycobacterium spp. Maura J. Donohue Ph.D. Office of Research and Development Center of Environmental Response and Emergency Response (CESER): Water Infrastructure Division (WID) Small Systems Webinar January 28, 2020 Disclaimer: The views expressed in this presentation are those of the author and do not necessarily reflect the views or policies of the U.S. Environmental Protection Agency. A Tale of Two Bacterium… Legionellaceae Mycobacteriaceae • Legionella (Genus) • Mycobacterium (Genus) • Gram negative bacteria • Nontuberculous Mycobacterium (NTM) (Gammaproteobacteria) • M. avium-intracellulare complex (MAC) • Flagella rod (2-20 µm) • Slow grower (3 to 10 days) • Gram positive bacteria • Majority of species will grow in free-living • Rod shape(1-10 µm) amoebae • Non-motile, spore-forming, aerobic • Aerobic, L-cysteine and iron salts are required • Rapid to Slow grower (1 week to 8 weeks) for in vitro growth, pH: 6.8 to 7, T: 25 to 43 °C • ~156 species • ~65 species • Some species capable of causing disease • Pathogenic or potentially pathogenic for human 3 NTM from Environmental Microorganism to Opportunistic Opponent Genus 156 Species Disease NTM =Nontuberculous Mycobacteria MAC = M. avium Complex Mycobacterium Mycobacterium duvalii Mycobacterium litorale Mycobacterium pulveris Clinically Relevant Species Mycobacterium abscessus Mycobacterium elephantis Mycobacterium llatzerense. Mycobacterium pyrenivorans, Mycobacterium africanum Mycobacterium europaeum Mycobacterium madagascariense Mycobacterium rhodesiae Mycobacterium agri Mycobacterium fallax Mycobacterium mageritense, Mycobacterium riyadhense Mycobacterium aichiense Mycobacterium farcinogenes Mycobacterium malmoense Mycobacterium rufum M. avium, M. intracellulare, Mycobacterium algericum Mycobacterium flavescens Mycobacterium mantenii Mycobacterium rutilum Mycobacterium alsense Mycobacterium florentinum. Mycobacterium marinum Mycobacterium salmoniphilum ( M. fortuitum, M. -
Mycobacterium Microti Infection in Red Foxes in France
microorganisms Article Mycobacterium microti Infection in Red Foxes in France Lorraine Michelet 1 ,Céline Richomme 2 , Edouard Réveillaud 3, Krystel De Cruz 1, Jean-Louis Moyen 4 and Maria Laura Boschiroli 1,* 1 Paris-Est University, National Reference Laboratory for Tuberculosis, Animal Health Laboratory, Anses, 94700 Maisons-Alfort, France; [email protected] (L.M.); [email protected] (K.D.C.) 2 Anses, Nancy Laboratory for Rabies and Wildlife, 54220 Malzéville, France; [email protected] 3 Regional Directorate for Food, Agriculture and Forest of Nouvelle-Aquitaine, 87000 Limoges, France; [email protected] 4 Laboratoire Départemental d’Analyse et de Recherche de la Dordogne, 24660 Coulounieix-Chamiers, France; [email protected] * Correspondence: [email protected] Abstract: Mycobacterium microti, member of the Mycobacterium tuberculosis, complex is known to interfere in the screening and diagnosis of bovine tuberculosis. This pathogen is increasingly detected in the frame of surveillance programs for tuberculosis in livestock and wildlife. Recently, red foxes (Vulpes vulpes) were found infected by Mycobacterium bovis in four French endemic areas. M. microti infection was concomitantly found during this investigation. Rates of infection by M. microti and M. bovis are not different except in one of the four areas (lower prevalence for M. microti in Charente). As for M. bovis infection, none of the infected foxes presented gross TB-like lesions. Infection of red foxes by M. microti seems to occur by ingestion of contaminated food, as mesenteric lymph nodes are mostly infected albeit no fecal excretion could be detected. Red foxes appear to be susceptible to Mycobacterium microti infection but seem to play a role of dead-end host for the transmission of Citation: Michelet, L.; Richomme, C.; this bacillus. -
The Evolution of Mycobacterial Pathogenicity: Clues from Comparative Genomics
452 Review TRENDS in Microbiology Vol.9 No.9 September 2001 The evolution of mycobacterial pathogenicity: clues from comparative genomics Roland Brosch, Alexander S. Pym, Stephen V.Gordon and Stewart T.Cole Comparative genomics, and related technologies, are helping to unravel the times (1–14 days) and include the principal human molecular basis of the pathogenesis, host range, evolution and phenotypic pathogens, the tubercle and leprosy bacilli. The differences of the slow-growing mycobacteria. In the highly conserved M. tuberculosis complex comprises M. tuberculosis Mycobacterium tuberculosis complex, where single-nucleotide together with Mycobacterium africanum, polymorphisms are rare, insertion and deletion events (InDels) are the principal Mycobacterium bovis, Mycobacterium canettii and source of genome plasticity. InDels result from recombinational or insertion Mycobacterium microti and is defined as a single sequence (IS)-mediated events, expansion of repetitive DNA sequences, or species by DNA–DNA hybridization studies3, with replication errors based on repetitive motifs that remove blocks of genes or exceptionally little sequence variation4,5 (Fig. 1). contract coding sequences. Comparative genomic analyses also suggest that The subspecies can only be distinguished by a loss of genes is part of the ongoing evolution of the slow-growing limited number of phenotypic or, more recently, mycobacterial pathogens and might also explain how the vaccine strain BCG genotypic characteristics, but differ remarkably became attenuated. with respect to their host range and pathogenicity. M. microti, for example, is almost exclusively a Genomics has the potential to provide a complete rodent pathogen and has been used successfully as understanding of the genetics, biochemistry, a live vaccine against TB, whereas M.