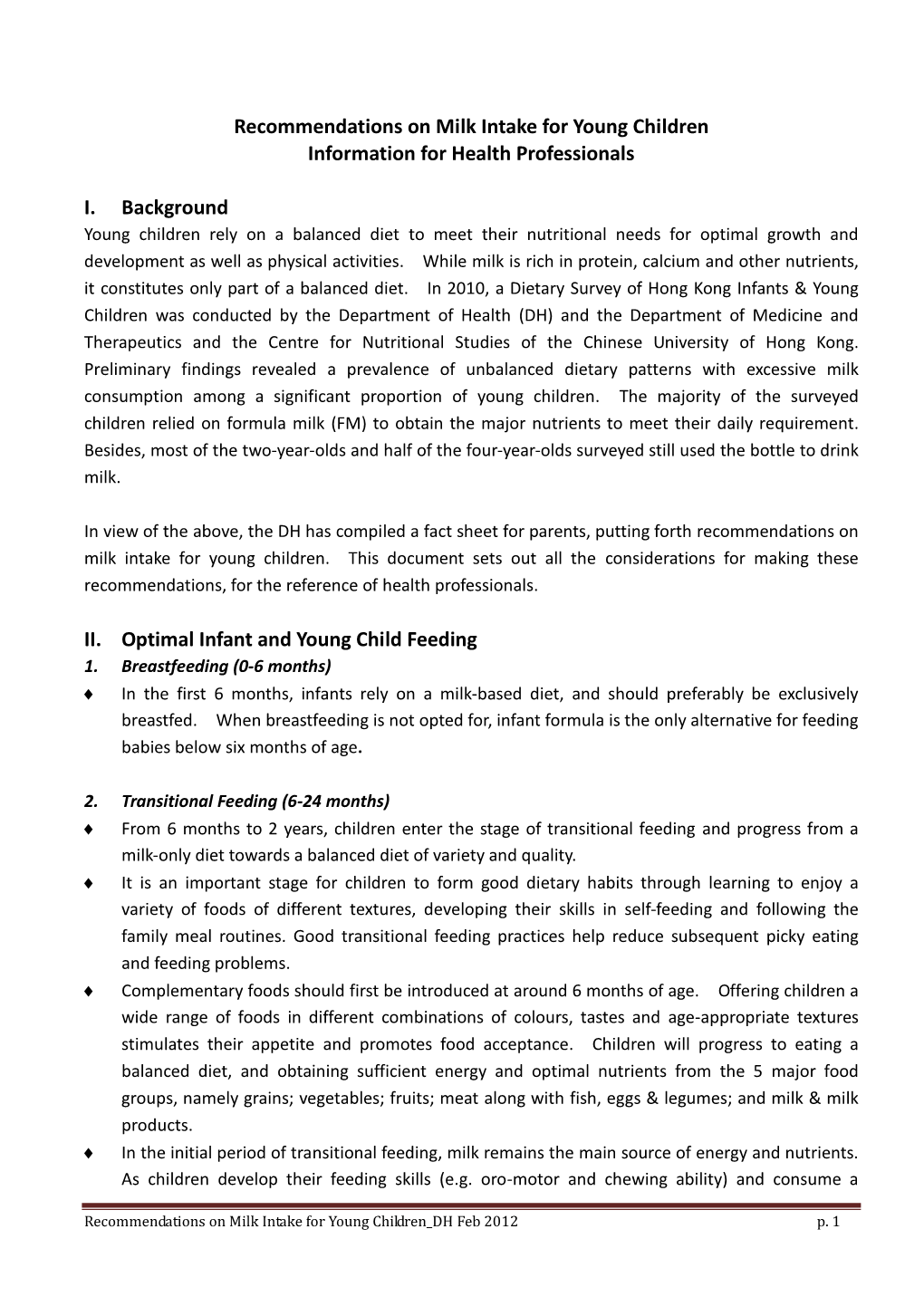
After 6 Months of Age, Is It Necessary to Switch to a High Protein Infant Or Toddler Formula
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Food Fortification
FOOD FORTIFICATION Fortifying foods Normal food can be fortified with: . Dried milk powder . Evaporated milk . Cream . Butter . Cheese . Jam . Sugar . Dried milk powder Weight Calories (kcals) Protein (g) 15g/ 1tablespoon 50 5.5 The easiest way of adding dried milk powder to milk is to mix up 2 - 4 tablespoons of dried milk powder to 1 pint of whole milk. Patients can start using 2 tablespoons and increase to 4 after a few days. Dried milk powders (own label, Marvel etc.) is recommended rather than ones with added vegetable fats. Weight Calories (kcals) Protein (g) I pt semi-skimmed milk 300 19.4 1 pt whole milk 396 19.2 1 pt whole milk + 4 570 37.2 tablespoons dried milk powder How to make fortified milk: Mix the dried milk powder with a little milk to form a paste and gradually whisk in the rest of the milk using a fork or a small whisk or in a liquidiser. This milk can then be used to make coffee, other milk based drinks, porridge and milk puddings etc. If 1 pint is used per day, then this goes a long way towards calorie requirements. It is not recommended that it is used in tea. Weight Calories (kcals) Protein (g) Porridge made with water 49 1.5 Porridge made with whole 116 4.8 milk Porridge made with 144 6.2 fortified milk Weight Calories (kcals) 200ml supplement e.g. Ensure/ Fresubin 300 Energy 260ml milkshake (fortified milk, 1 scoop ice- 300 cream & milkshake syrup) . Evaporated milk Evaporated milk can be poured over fresh, tinned and stewed fruit or added to other puddings. -
Growing, Moving, Learning – Infant Toddler Toolkit
Growing, Moving, Learning Infant Toddler Toolkit May 2011 NOTICE: The University of Delaware does not discriminate on the basis of race, color, national origin, sex, disability, or age in its programs and activities. The following person has been designated to handle inquiries regarding the non-discrimination policies and to serve as the overall campus coordinator for purposes of Title IX compliance: Name and Title: Becki Fogerty Director, Office of Equity and Inclusion Address: 305 Hullihen Hall University of Delaware Newark, DE 19716 Telephone No.: (302) 831-8063 The following person has been designed to handle inquiries regarding the non-discrimination policies as those policies apply to the University’s Division of Intercollegiate Athletics and Recreation Services: Name and Title: Jennifer W. Davis Vice President for Finance and Administration Address: 220 Hullihen Hall University of Delaware Newark, DE 19716 Telephone: (302) 831-2769 Inquiries concerning the application of Title IX may be referred to the appropriate Title IX coordinator or to the Office for Civil Rights, United States Department of Education. For further information on notice of non-discrimination, visit http://wdcrobcolp01.ed.gov/CFAPPS/OCR/contactus.cfm for the address and phone number of the U.S. Department of Education office that serves your areas, or call (800) 421-3481. Acknowledgements We would like to acknowledge Penny Deiner, Ph.D., Professor Emerita and past Chair of the Department of Human Development and Family Studies, at the University of Delaware as the original author of the Infant Toddler Toolkit for Healthy Eating and Physical Activity. Dr. Deiner developed and piloted the original activities jointly with Nemours Health and Prevention Services. -

Pediatric Respiratory Rates Age Rate (Breaths Per Minute)
Pediatric Respiratory Rates Age Rate (breaths per minute) Infant (birth–1 year) 30–60 Toddler (1–3 years) 24–40 Preschooler (3–6 years) 22–34 School-age (6–12 years) 18–30 Adolescent (12–18 years) 12–16 Pediatric Pulse Rates Age Low High Infant (birth–1 year) 100 160 Toddler (1–3 years) 90 150 Preschooler (3–6 years) 80 140 School-age (6–12 years) 70 120 Adolescent (12–18 years) 60 100 Pulse rates for a child who is sleeping may be 10 percent lower than the low rate listed. Low-Normal Pediatric Systolic Blood Pressure Age* Low Normal Infant (birth–1 year) greater than 60* Toddler (1–3 years) greater than 70* Preschooler (3–6 years) greater than 75 School-age (6–12 years) greater than 80 Adolescent (12–18 years) greater than 90 *Note: In infants and children aged three years or younger, the presence of a strong central pulse should be substituted for a blood pressure reading. Pediatric CUPS Assessment Category Assessment Actions Example Critical Absent airway, Perform rapid initial Severe traumatic injury breathing, or interventions and transport with respiratory arrest or circulation simultaneously cardiac arrest Unstable Compromised airway, Perform rapid initial Significant injury with breathing, or interventions and transport respiratory distress, circulation with simultaneously active bleeding, shock; altered mental status near-drowning; unresponsiveness Potentially Normal airway, Perform initial assessment Minor fractures; unstable breathing, circulation, with interventions; transport pedestrian struck by car and mental status BUT -

Journal of Milk Technology
'-/· .> Ί ' JOURNAL OF MILK TECHNOLOGY Volu 14 Number 2 MARCH-APRIL, 1941 Official Publication of International Association of Milk Sanitarians (Association Organized 1911) Alto designated publication of California Association of Dairy and Milk Inspectors Central States Milk Sanitarians Chicago Dairy Technology Society Connecticut Association of Dairy and Milk Inspectors Indianapolis Dairy Technology Club Massachusetts Milk Inspectors’ Association Metropolitan Dairy Technology Society Michigan Association of Dairy and Milk Inspectors Missouri Association of Milk Sanitarians New York State Association of Dairy and Milk Inspectors Pacific Northwest Association of Dairy and Milk Inspectors Pennsylvania Association of Dairy Sanitarians Philadelphia Dairy Technology Society Texas Association of Milk Sanitarians West Virginia Association of Milk Sanitarians II A dvertisements PERHAPS as a boy you took many a drink from it without a thought about how insanitary it might be. N ot so today. The patient work of sanitation and pub YOUR DAIRY CUSTOMERS can actually lic health officers has taught you to say see the safe protection of the Welded “nix” to the public drinking cup. And Wire Hood —and seeing is believing. their science, too, has solved many They recognize that you are safeguard problems of dairy sanitation—including ing their health when they see how you how to protect the pouring lip of your protect that pouring lip from contami sterilized milk and cream bottles. nation. Vet, even though the Hood is locked on with welded wire, it comes off HEALTH OFFICERS themselves say that quickly, without effort. they prefer the complete protection of the Welded Wire Hood Seal. It covers FREE INFORMATION-W rite for details the entire pouring lip and top against on Hood Capping and our interesting insanitary dust and filth. -

ACT Early Milestone Moments
Milestone Moments Learn the Signs. Act Early. Learn the Signs. Act Early. www.cdc.gov/milestones 1-800-CDC-INFO Adapted from CARING FOR YOUR BABY AND YOUNG CHILD: BIRTH TO AGE 5, Fifth Edition, edited by Steven Shelov and Tanya Remer Altmann © 1991, 1993, 1998, 2004, 2009 by the American Academy of Pediatrics and You can follow your child’s development by watching how he or BRIGHT FUTURES: GUIDELINES FOR HEALTH SUPERVISION OF INFANTS, CHILDREN, AND ADOLESCENTS, Third she plays, learns, speaks, and acts. Edition, edited by Joseph Hagan, Jr., Judith S. Shaw, and Paula M. Duncan, 2008, Elk Grove Village, IL: American Academy of Pediatrics. Special acknowledgements to Susan P. Berger, PhD; Jenny Burt, PhD; Margaret Greco, MD; Katie Green, MPH, Look inside for milestones to watch for in your child and how you CHES; Georgina Peacock, MD, MPH; Lara Robinson, PhD, MPH; Camille Smith, MS, EdS; Julia Whitney, BS; and can help your child learn and grow. Rebecca Wolf, MA. Centers for Disease Centers for Disease Control and Prevention Control and Prevention www.cdc.gov/milestones www.cdc.gov/milestones 1-800-CDC-INFO 1-800-CDC-INFO 220788 Milestone Moments How your child plays, learns, speaks, and acts offers important clues about your child’s development. Developmental milestones are things most children can do by a certain age. The lists that follow have milestones to look for when your child is: 2 Months ............................................................... page 3 – 6 Check the milestones your child has reached at each age. 4 Months ............................................................... page 7 –10 Take this with you and talk with your child’s doctor at every visit about the milestones your child has reached and what to 6 Months .............................................................. -

Transmembrane Pressure and Recovery of Serum Proteins During Microfiltration of Skimmed Milk Subjected to Different Storage and Treatment Conditions
foods Article Transmembrane Pressure and Recovery of Serum Proteins during Microfiltration of Skimmed Milk Subjected to Different Storage and Treatment Conditions Manon Granger-Delacroix 1,2 , Nadine Leconte 1, Fabienne Garnier-Lambrouin 1, Françoise Le Goff 2, Marieke Van Audenhaege 2 and Geneviève Gésan-Guiziou 1,* 1 INRAE, Agrocampus Ouest, STLO, F-35042 Rennes, France; [email protected] (M.G.-D.); [email protected] (N.L.); [email protected] (F.G.-L.) 2 Sodiaal International, Department of Research & Innovation, 75014 Paris, France; francoise.legoff@sodiaal.fr (F.L.G.); [email protected] (M.V.A.) * Correspondence: [email protected] Received: 3 March 2020; Accepted: 18 March 2020; Published: 27 March 2020 Abstract: Milk pre-processing steps-storage at 4 ◦C (with durations of 48, 72 or 96 h) and methods for microbiological stabilization of milk (1.4 µm microfiltration, thermization, thermization + bactofugation, pasteurization) are performed industrially before 0.1 µm-microfiltration (MF) of skimmed milk to ensure the microbiological quality of final fractions. The objective of this study was to better understand the influence of these pre-processing steps and their cumulative effects on MF performances (i.e., transmembrane pressure, and transmission and recovery of serum proteins (SP) in the permeate). Results showed that heat treatment of skimmed milk decreased ceramic MF performances, especially after a long 4 ◦C storage duration (96 h) of raw milk: when milk was heat treated by pasteurization after 96 h of storage at 4 ◦C, the transmembrane pressure increased by 25% over a MF run of 330 min with a permeation flux of 75 L h 1 m 2 and a volume reduction ratio of 3.0. -

Living with Infants, Toddlers, and Children Who Have Been Prenatally Exposed to Alcohol
Living with Infants, Toddlers, and Children who have been Prenatally Exposed to Alcohol This section includes practical information about what to look for and how to successfully deal with your infant, toddler, or child who has been affected by prenatal alcohol exposure. Much of the information comes directly from parent experiences. Also included is information that we encourage you to copy and share with your child's teachers and other caregivers. It is crucial for everyone involved in the care and education of a child with disabilities to remember that they are first a child and second, a child with a disability. Children with FAS or ARND, like all children, will move through various stages of normal development. They may not move as quickly or as distinctly, but they will move and grow. With growth come struggles and challenges. A typically developing child may demonstrate some of the behaviors described in this section, but because he or she does not present a disability, their behavior is dealt with and accepted as a normal part of growing up. Conversely, children with disabilities often display appropriate or typically challenging behaviors for a child at their developmental level, but because they have a disability, their behavior becomes amplified by those who are working with and caring for them. Because this happens so frequently and unconsciously, readers are urged to balance their perceptions of their child's behavior with their knowledge and experience of normal/typical child development and behavior. � How Parents Can Help -

Infant Formula Containing Full Cream Milk Fats: Latest Innovations
PAEDIATRIC SUPPLEMENT INFANT FORMULA CONTAINING FULL CREAM MILK FATS: LATEST INNOVATIONS Dr Emma Derbyshire The benefits of breastfeeding are well established, with exclusive Independent breastfeeding recommended for up to six months of age. Presently, in Great Consultant Britain, less than 17% of women comply with these guidelines and manage to breastfeed ‘exclusively’ for the full six months. Emma heads Nutritional Insight Ltd, an independent In circumstances where breastfeeding to breastfeed. There is evidence that consultancy to industry, may not be possible, solely adequate, long labours, maternal exhaustion and government, or suitable, closely matched alternatives stress due to traumatic deliveries can publishers and PR 3 agencies. She is are needed. This article aims to discuss all lead to delayed lactogenesis. Other an avid writer for the nutritional profile of infant formula work has shown that women delivering scientific journals and media. Her that uses full-cream milk fats (whole by emergency C-section have a higher specialist areas cows’ milk) and explains how these proportion of breastfeeding difficulties are public health products are evolving and integrating (41%) compared to those delivering nutrition, maternal 4 and child nutrition the latest science. vaginally (29%). Medical conditions, and functional foods. It is widely acknowledged that such as tongue tie (ankyloglossia), can www.nutritional- insight.co.uk breastfeeding is best, having many also affect an infant’s ability to latch 5 @DrDerbyshire short and long-term benefits for both on, leading to breastfeeding problems. mother and child.1 The World Health A summary of studies investigating Organisation (WHO) advises that obstacles to breastfeeding is shown in For full article ‘exclusive breastfeeding is recommended Table 1. -

Typical Child Development
TYPICAL CHILD DEVELOPMENT ADOLESCENTS Physical • Rapid growth, maturity of sexual organs, development of secondary sexual characteristics • Girls generally physically mature before boys • Learning to accept changes in their bodies and adapt their behavior based on these changes Cognitive • Begin to think hypothetically and see different points of view • During middle and late adolescents the ability to see multiple perspectives is refined Social • Group values guide individual behavior. In early adolescence most peer groups are still same sex • Become interested in sexual relationships but most contact is through groups. May begin to experiment in sexual behavior • In early adolescence social roles still largely defined by external sources • During middle and late adolescence • Choose friends based on personal characteristics and mutual interest. Peer group declines in interest. • Experiment with social roles and explore options for career choices Emotional • Depend upon peers for emotional stability, support and to help mold their emerging identities • Self-esteem greatly affected by acceptance of peers • Early adolescents are moody, dramatic and very vulnerable to emotional stress • Middle and late adolescence, identity is more individualized and a sense of self develops and stabilizes • Self- esteem in middle and late adolescence is influenced by his/her ability to live up to internalized standards for behavior SCHOOL AGE Physical • The ability to sit still and attend increases as they move through this stage • Practice, refine, and -

Child Development-Prenatal-Toddler
St. Michael-Albertville High School Child Development Prenatal Through Toddler Teacher: Christie Larson September 2021 Content Skills Learning Targets Assessment Resources & Technology CEQ: WHAT ARE THE BENEFITS OF STUDYING CHILD DEVELOPMENT? UEQ: Unit 1 Learning About Children • What are the three areas of child development? •What are the reasons for studying children? •What are the principles of growth and development? • Who are some leading child development theorists? National Standards: 13.5.1 13.5.2 Child and Human Development Framework MCHD 2.1 MCHD 3.4 www.curriculummapper.com 113 Larson Child Development Prenatal Through Toddler St. Michael-Albertville High School A: Learning About A: Learning About A: Learning About A: Learning About A: Learning About Children Children Children Children Children A1: 3 developmental areas A1: Identify the three areas LT1: I can describe reasons A1: Development Poster A2: Reasons for studying of Child Development for studying children. A1: Ch. 1 "The Subject "Children:The Early Years, children. A2. Describe reasons for Matter of Child 2011" Chapter 1: Learning A3: Influences on studying children LT2: I can describe the Development" About Children development A3: Identify and describe factors that promote or A2: Ch. 1 "Parent's Aid in A4: Leading child the factors that promote inhibit growth and Growth and Development" "Developmental Theorists" development theorists growth and development development. WS DVD A4: Identify the leading A2: Ch. 1, "Individual Life theorists of child LT3: I can explain how Cycle" WS Chapter 1 VOCAB: Development (Maslow, brain development occurs. A3: Ch. 1 "Principles of Child Development Piaget, Erickson, and other Growth and Development" Intellectual Development current theorists) LT4: I can explain the WS Social-Emotional major principles and A3: Ch. -

GRAS Notice 644: Non-Fat Dry Goat Milk and Goat Whey Protein
GRAS Notice (GRN) No. 644 http://www.fda.gov/Food/IngredientsPackagingLabeling/GRAS/NoticeInventory/default.htm ORIGINAL SUBMISSION GENERALLY RECOGNIZED,. AS SAFE GRAS Associates, LLC 27499 Riverview Center Blvd. GRAS Bonita Springs, FL 34134 ASSOCIATES , LLC T : 239.444.17241 F: 239.444.1723 www.gras-associates.com v G-R N ooo bY '1 3/15/2016 Food and Drug Administration Center for Food Safety & Applied Nutrition Office of Food Additive Safety (HFS-255) 5100 Paint Branch Parkway College Park, MD 20740-3835 Attention: Dr. Paulette Gaynor Re : GRAS Notification - Nonfat Dry Goats' Milk and Goat Whey Protein Dear Dr. Gaynor: On behalf of Ausnutria Hyproca B.V. of The Netherlands, we are submitting for FDA review Form 3667 and the enclosed CD, free of viruses , containing a GRAS notification for Nonfat Dry Goats' Milk and Goat Whey Protein Concentrate in Infant Formula . An Expert Panel of qualified persons was assembled to assess the composite safety information of the subject substance with the intended use in infant formula. The attached documentation contains the specific information that addresses the safe human food uses for the subject notified substance as discussed in the GRAS guidance document. If additional information or clarification is needed as you and your colleagues proceed with the review, please fe'el free to contact me via telephone or email. We look forward to your feedback. Sincerely, (b) (6) Cheryl R. Dicks, MS, RAC Director of Regulatory Affairs GRAS Associates, LLC t AR 2 1 2015 27499 Riverview Center Blvd ., Suite 212 Bonita Springs, FL 34134 OFFICE OF 540-272-3254 FOOD ADDITIVE SAFETY dicks@gras-associates. -

Health Care Provider Fact Sheet
Out of Harm’s Way: Preventing Toxic Threats to Child Development Health Care Provider Fact Sheet Your patients are exposed regularly to a wide .Inside: variety of household and environmental Taking an Environmental History chemicals - in the food they eat, the water Frequently Asked Questions they drink and the air they breathe. Many of from Providers these chemicals, such as lead, mercury, PCBs Suggested Routine Questions (polychlorinated biphenyls), dioxin, pesticides, to Ask Patients and solvents are known neurotoxicants. Exposures to these chemicals during critical Sample Advice periods of early brain development can have Preventing Harmful Chemical Exposures life-long adverse effects and contribute to Routine Advice for Patients learning, behavioral and developmental Products to Avoid disabilities. Health care providers can help Dietary Advice prevent unnecessary risks to child develop- ment by offering simple, common sense Habits guidelines for reducing potentially harmful Key Points exposures to known and suspected develop- mental neurotoxicants. This fact sheet provides busy clinicians with essential information on key toxicants and their effects. It also provides suggestions for routine patient advice and a strategy to help patients identify and reduce potentially harmful exposures. Greater Boston Physicians for Social Responsibility April 2001 Taking an Environmental History Suggested Routine Questions to Ask Patients Frequently Asked Questions from Providers linicians without expertise in environmental and occupational health Q: Do I need to be an expert in environmental health to Ccan screen for exposures of concern and provide common sense take an environmental history? responses to most identified exposures. Environmental questions are readily incorporated into a standard history. “CH2OP” provides a framework for A: No, many of the routine questions and advice regarding inquiring about potentially harmful exposures, (Community, Home/Hobbies, the environment and exposures to toxic chemicals are common Occupational, Personal.