The Development Of A Novel Chimeric Antigen Receptor Specific For Syndecan-1
by
Elliot Berinstein
A thesis submitted in conformity with the requirements for the degree of Master of Science Department of Medical Biophysics University of Toronto
© Copyright by Elliot Berinstein 2016
The Development Of A Novel Chimeric Antigen Receptor Specific For Syndecan-1
Elliot Berinstein
Master of Science
Department of Medical Biophysics University of Toronto
2016 Abstract
The adoptive transfer of T lymphocytes expressing chimeric antigen receptors (CARs) has become a promising treatment for various cancers. CARs have been shown to redirect the cytotoxicity of T lymphocytes towards cancerous cells independent of the interactions between T cell receptors and major histocompatibility complexes. Given that CARs tie together an extracellular recognition domain with intracellular signaling domains of immune cells, there exists flexibility in designing CARs specific for different antigens in order to target different malignancies.
Here, we established murine antibodies specific for CD138 with the goal of designing a novel CAR. We designed a 2nd generation CAR using a single chain variable fragment derived from the 3E9B6 monoclonal antibody as the extracellular recognition domain. The expression of the 3E9B6 HL CAR specifically enhanced the cytotoxicity of the NK-92 cell line against
CD138+ cells. Downstream activation of ZAP70 in NK-92 3E9B6 HL CAR cells was also dependent on the presence of CD138+ target cells. This work shows that the 3E9B6 HL CAR is functionally able to recognize CD138 and to initiate the CD3ζ activation pathway.
ii
Acknowledgments
Firstly, I would like to thank my supervisor, Dr. Medin, for the opportunity to work on this project and his mentorship. I would like to thank my supervisory committee of Drs. Spaner and Kerbel for their intellectual contributions and insight throughout my graduate studies.
I would like to thank the members of the Medin lab for their contributions, feedback and support. I would especially like to thank Robyn Oldham for working with me on this and all of the various Team Cancer projects.
I would like to thank the chair, Dr. Lilge, and examiners of my thesis, Drs. Minden and Chakrabartty for making my defense possible.
I would also like to thank the department of Medical Biophysics for their financial and administrative support.
Finally I would like to thank my father, Dr. Neil Berinstein, for sparking and inspiring my interest in cancer immunotherapy, sharing his clinical knowledge with me and helping me draft my thesis.
iii Table of Contents
Acknowledgments ...... iii
Table of Contents ...... iv
Abbreviations ...... vii
Chapter 1 Introduction ...... 1
1.1 Cancer ...... 1
1.1.1 The Hallmarks Of Cancer ...... 1
1.1.2 Cancer Immunoediting ...... 1
1.1.3 Mechanisms of Tumour Escape ...... 2
1.1.3.1 Downregulation of MHC ...... 2
1.1.3.2 Polarization of The Th Response ...... 3
1.1.3.3 Immunosuppressive molecules ...... 4
1.1.3.4 Immunosuppressive cells ...... 4
1.2 Cancer Immunotherapy ...... 5
1.2.1 The Development of Cancer Immunotherapies ...... 5
1.2.1.1 Hybridoma Technology ...... 6
1.2.1.2 Primary Cell Culture and Expansion ...... 7
1.2.1.3 Gene Transfer Technology ...... 8
1.2.2 Cancer Immunotherapies In the Clinic ...... 11
1.2.2.1 Antibody Therapies ...... 12
1.2.2.2 Targeting the Immune System with mAbs ...... 14
1.2.3 Adoptive Cellular Therapy ...... 18
1.2.3.1 Tumour Infiltrating Lymphocyte ...... 18
1.2.3.2 TCR modified T cells ...... 19
1.2.3.3 Chimeric Antigen Receptors ...... 21
iv 1.2.3.4 NK Adoptive Cellular Therapies ...... 28
1.3 Multiple Myeloma ...... 29
1.3.1 Biology Of Multiple Myeloma ...... 29
1.3.2 Standard Therapy For Multiple Myeloma ...... 30
1.3.3 Tumour Associated Antigens for immunotherapy in Multiple Myeloma ...... 31
1.3.3.1 Cyclic ADP Ribose Hydrolase (CD38) ...... 31
1.3.3.2 TNF Receptor Superfamily Member 5 (CD40) ...... 32
1.3.3.3 NCAM1 (CD56) ...... 32
1.3.3.4 HLA-DR Antigens-Associated Invariant Chain (CD74) ...... 33
1.3.3.5 Syndecan-1 (CD138) ...... 33
1.3.3.6 B Cell Maturation Antigen (CD269) ...... 34
1.3.3.7 SLAMF7 (CD319) ...... 34
1.4 Rationale ...... 35
1.5 Purpose and Specific Aims ...... 36
Chapter 2 Methods ...... 37
2 Methods ...... 37
2.1 Antibody Purification ...... 37
2.2 CD138 Overexpression Cell Lines ...... 37
2.3 Flow Cytometry ...... 38
2.4 Growth Assays ...... 38
2.5 Proteome Profiler Human Phospho-Kinase Array Kit ...... 38
2.6 Western blots ...... 39
2.7 Gene Sequencing ...... 39
2.8 Chimeric Antigen Receptor Lentiviral Design and Production ...... 40
2.9 NK-92 Transduction ...... 40
2.10 Protein L Binding ...... 41 v 2.11 Cytotoxicity Assay ...... 41
Chapter 3 Results ...... 42
3 Results ...... 42
3.1 CD138-positive hybridoma clones were identified by indirect ELISAs ...... 42
3.2 CD138 Positive Hybridoma clones ability to bind to CD138 was confirmed by western blot ...... 44
3.3 Purified mAb binds to CD138 positive cell lines ...... 46
3.4 3E9B6 stimulates growth of CD138 positive cells ...... 48
3.5 3E9B6 stimulation affects intracellular signaling pathways ...... 50
3.6 Phosphorylation of p53 is upregulated by 3E9B6 ...... 52
3.7 Sequencing mAb heavy and light chains ...... 54
3.8 The design of the 3E9B6 Chimeric Antigen Receptor ...... 56
3.9 The Generation of a Stable NK-92 Cell Line expressing the 3E9B6 CAR ...... 58
3.10 Protein L Direct Detection of CAR ...... 60
3.11 3E9B6 HL CAR enhances NK-92 cytotoxicity for CD138 positive Cells ...... 62
3.12 3E9B6 HL CAR Initiates Downstream ZAP70 signaling ...... 64
Chapter 4 Discussion ...... 66
4 Discussion ...... 66
4.1 The 3E9B6 HL CAR ...... 66
4.2 3E9B6 HL CAR NK Cells ...... 67
4.3 In Vivo Models of Multiple Myeloma to test 3E9B6 HL CAR ...... 68
4.4 CD138 as a Target For CAR Therapy ...... 69
4.5 3E9B6 mAb enhanced MM cell growth ...... 71
4.6 Other Potential Therapeutic uses of 3E9B6 ...... 74
4.7 Conclusions ...... 75
References ...... 77
vi Abbreviations
ADCC Antibody dependent cellular cytotoxicity ADCP Antibody dependent cellular phagocytosis ALL Acute lymphoblastic leukemia Allo-SCT Allogeneic stem cell transplant APC Antigen presenting cell AZT Azidothymidine BSA Bovine serum antigen CAR Chimeric antigen receptor CD Cluster of differentiation CDC Complement dependent cytotoxicity CDR Complimentary determining region CHK-2 CHK-2 CK-2 Casein kinase 2 CLL Chronic lymphocytic leukemia CR Complete response CRS Cytokine release syndrome CTL Cytotoxic T lymphocytes CRISPR Clustered regularly interspaced short palindromic repeats DC Dendritic cell DCK Deoxycytidine DNA Deoxyribonucleic acid EDTA Ethylenediaminetetraacetic acid EGFR Epidermal growth factor receptor Fab Fragment antigen binding FACS Fluorescence activated cell sorting Fc Fragment crystallizable region FDA Food and Drug Administration FR Framework region GFP Green fluorescence protein GITR Glucocorticoid-induced TNFR family related gene GM-CSF Granulocyte-macrophage colony-stimulating factor GVHD Graft versus host disease H Hours HIPK1 Homeodomain-interacting kinase 1
vii HSV Herpes simplex virus IFN Interferon IL Interleukin Ig Immunoglobulin IMiD Immunomodulating drugs KIR Killer cell immunoglobulin-like receptor LAG-3 Lymphocyte-activation gene 3 LTR Long terminal repeat LV Lentivirus MART-1 Melanoma antigen recognized by T cells 1 mAb Monoclonal Antibody MDSC Myeloid-derived suppressor cells MHC Major histocompatibility complex Min Minutes MLV Murine leukaemia virus MRD Minimal residual disease NHL Non-Hodgkin’s lymphoma NK Natural killer NSG Non-obese diabetic SCID gamma OR Objective response PBS Phosphate buffered saline PFA Paraformaldehyde PC Plasma cell PCR Polymerase chain reaction PD Programmed cell death protein PD-L Programmed death ligand PGE2 Prostaglandin E2 PR Partial Response PVDF Polyvinylidene difluoride RNA Ribonucleic acid Rpm Rotations per minute RPMI Roswell Park Memorial Institute ScFv Single chain variable fragment SCID Severe combined immunodeficiency SD Stable disease SDS Sodium dodecyl sulfate Sec Seconds TBS Tris-buffered saline TCR T cell receptor TIL Tumour infiltrating lymphocyte Tcm Central memory T cell Th Helper T cell Treg Regulatory T cell Tscm Stem memory T cell TGF Tumour growth factor TK Thymidine kinase TMPK Thymidylate kinase TNF Tumour Necrosis Factor
viii VEGF Vascular endothelial growth factor ZAP70 Zeta-chain associated protein 70
ix Chapter 1 Introduction 1.1 Cancer
1.1.1 The Hallmarks Of Cancer
Cancer is a wide variety of diseases that together are the leading cause of death in Canada[1]. In 2015 over 200,000 Canadians were diagnosed with cancer and approximately 78,000 died from their disease[1]. Cancer develops when the genetic instructions of a cell become damaged or misread leading to a population of malignant cells that have acquired uncontrolled and limitless cell growth[2]. The cancerous cells begin to provide their own growth signals, become insensitive to and evade anti-growth and apoptosis signals[2]. Cancer cells also become invasive and metastatic by creating an environment of sustained angiogenesis[2]. More recently, it has been accepted that acquiring the ability to evade the immune system is also a fundamental hallmark of cancer[3].
1.1.2 Cancer Immunoediting
The concept of boosting the immune system to treat cancer has been around for over 100 years dating back to the end of the 19th century when Dr. William Coley used bacterial toxins to enhance the immune system of cancer patients to treat their disease[4]. The observable benefit has led to the investigation of how the immune system interacts with cancer and the development of immunotherapies. Midway through the 20th century, immunologists began to recognize that tumours were immunologically distinct from the self[5]. In 1970, the hypothesis of cancer immunosurveillance proposed that a healthy immune system could recognize and destroy nascent transformed cells and that in order for cancer to develop it must learn to evade or shutdown the immune system of the host[6]. The development of monoclonal antibodies (mAbs), transgenic mice and gene targeting systems has allowed this hypothesis to be more precisely investigated. As this theory has matured, it has become more apparent that the immune system not only functions in host protection but also in tumour sculpting by selecting for variants that are better suited to survive in an immunologically intact host[7, 8]
1 2
This larger story has been termed cancer immunoediting and has three phases; elimination, equilibrium and escape[9]. Immunosurveillance or host protection occurs in the elimination phase when effector arms of the immune system, specifically cytotoxic T lymphocytes (CTLs) and natural killer (NK) cells, recognize malignancies and destroy them. Cells that are not killed enter into the equilibrium phase, where lymphocytes put a constant pressure to contain but not extinguish surviving cells. During this tumour-sculpting phase the cancerous cells undergo a Darwinian selection for variants that are better able to survive and grow with this immune pressure. This can eventually lead to the escape phase, where cancers become resistant to the immune system and expand to become clinically apparent. Understanding how tumours grow in the light of cancer immunoediting has changed the way we study cancer biology, treat patients and design novel therapies. For example, novel chemotherapies and epigenetic modulators that also induce immunogenic cell death and promote immune responses are being developed and tested in the clinic. Immune infiltrates and molecules have become important prognostic biomarkers in various diseases. There is also a growing concentration on developing immunotherapy platforms to treat patients with advanced disease.
1.1.3 Mechanisms of Tumour Escape
Cancers often adapt different mechanisms to increase central and peripheral tolerance to evade detection from the immune system. Cancer cells might gain immune privilege from CTLs and NK cells through a number of different mechanisms including; downregulating major histocompatibility complexes (MHC), helper T (Th) cell polarization, expression of immunosuppressive signals or the recruitment of immunosuppressive cells.
1.1.3.1 Downregulation of MHC
Virtually every cell type in the human body expresses class I MHC. Proteins from inside of the cell are processed and peptides are displayed on class I MHC to the T cell receptor (TCR) on CD8+ T cells for monitoring. This allows T cells to sample the inside of other cells in order 3 recognize and kill any that express foreign antigens related to a pathogen or generated during oncogenesis. It is well documented that tumour cells can downregulate or lose MHC expression[10]. The downregulation of MHC can be associated with invasive and aggressive tumours[11]. Without MHC expression, T cells cannot monitor cells for infection and oncogenesis. NK cells, however, use MHC as ligands for inhibitory receptors. The lack of MHC expression on the surface of malignant cells leads to a disrupted balance of activating and inhibitory signals within a network of receptors, alerting NK cells. [12]. In another phase of tumour sculpting, malignant cells might adapt other mechanisms to avoid NK cells by tilting the balance of signals back into inhibition or by immunosuppressive cytokines.
1.1.3.2 Polarization of The Th Response
Antigen presenting cells (APC) display antigen peptides to CD4+ Th cells. This leads to the differentiation of Th effector cells to provide the appropriate immune response. The major pathways of differentiation are towards Th1 and Th2 cells[13]. Th1 cells or type 1 responses are thought to be required for successful cellular immunity against virally infected or malignant cells[14]. Th1 effector cells can directly kill tumour cells but their main function is to generate and augment a CTL response. Type 2 responses or Th2 effector cells are associated with humoral and allergic responses. Tumour cells often release factors such as IL-6, IL-10, tumour growth factor-β (TGF-β), and prostaglandin E2 (PGE2) to polarize the immune response away from Th1 effector cells[15]. This can often lead to an ineffective or even a tumour promoting response.
Th17 cells are another interesting subtype of effector cells that play complex and conflicting role in anti-tumour immunity. Th17 cells have been shown to have a greater ability to stimulate CD8+
T cells and eradicate melanomas than Th1 cells in mouse models[16]. Conversely, Th17 cells have also been shown to promote tumour growth by releasing the immunosuppressive compound, adenosine, or by converting into T regulatory (Treg) cells[17, 18]. The balance of different Th effector subtypes plays a role in mounting and directing a successful anti-tumour immune response.
4
1.1.3.3 Immunosuppressive molecules
Cancerous cells often increase the expression of immunosuppressive molecules to avoid immune destruction. Tumour cells often express programmed cell death protein 1 (PD-1) ligands to increase apoptosis of tumour-reactive T cells[19]. PD-1 is a protein belonging to the B7 family that functions as an inhibitory receptor expressed on T cells at the immunological synapse. Its ligands, PD-L1 and PD-L2, are normally expressed on APCs in response to interferon-γ (IFN-γ) to maintain central and peripheral tolerance[20-22]. Tumour cells have also been shown to express indoleamine 2,3-dioxygenase to induce T cell tolerance by causing differentiation of Th cells into Treg cells[23]. B7-H4 is another molecule that can be expressed by tumour cells to avoid immune destruction[24]. This B7 family member protein has been shown to inhibit growth, secretion of activating cytokines, and decrease the cytotoxicity of T cells [25]. The expression of B7-H4 in the tumour microenvironment of ovarian carcinomas has been shown to positively correlate with the amount of infiltrating Treg cells and immunosuppressive cytokines, IL-6 and IL-10[24].
1.1.3.4 Immunosuppressive cells
Immunosuppressive cells are often recruited to provide peripheral tolerance at the tumour site.
Treg cells are important in preventing autoimmune disease[26]. In a wide variety of cancers, large populations of Treg cells have been observed in tumour tissue, lymph nodes and peripheral blood of patients[27]. Increased numbers of Treg cells have been associated with diminished anti- tumour T cell activity, recurrence, and decreased patient survival[28]. Tumour cells attract Treg cells via the release of C-C motif chemokine 22[29]. Treg cells can diminish anti-tumour immunity through many mechanisms. Firstly, Treg cells can directly kill tumour-specific T cells and APCs[30]. They also release the immunosuppressive cytokines, IL-10 and TGF-β[31]. This directly inhibits APC expression of MHC molecules, CD80, CD86 and the release of IL-12, which are all necessary to mount an anti-tumour T cell response.
Myeloid derived suppressor cells (MDSCs) are a heterogeneous group of cells with myeloid origin that are potent suppressors of anti-tumour immunity. MDSCs include myeloid progenitor cells, immature dendritic cells (DCs), macrophages and granulocytes [32]. MDSC accumulation
5 is driven by inflammation, vascular endothelial growth factor (VEGF), granulocyte-macrophage colony-stimulating factor (GM-CSF), IL-1β, IL-6, IL-8, and PGE2[32]. MDSCs can suppress anti-tumour immunity through a diverse set of mechanisms that perturb the innate and adaptive immune systems. They inhibit T cells by depleting the microenvironment of the amino acids, arginine and cysteine, which are both necessary for T cell activation[33, 34]. MDSCs also disrupt T cell function by releasing reactive oxygen species and peroxynitrites to cause TCR nitration, which diminishes the ability of the TCR to bind to peptides displayed on MHCs[35]. They also decouple the signal transducing CD3ζ chain from the TCR complex, preventing tumour specific T cells from being activated[36]. MDSCs can also inhibit NK cells by downregulating their expression of activating receptors NKG2D, NKp46, and NKp44[37]. MDSCs also provide immune privilege to tumours by releasing IL-10 and TGF-β to polarize the immune response towards Th2 effector cells and recruit Treg cells [38, 39]. MDSCs, like Treg cells, have proven to be prolific suppressors and formidable obstacles of an anti-tumour response.
1.2 Cancer Immunotherapy
1.2.1 The Development of Cancer Immunotherapies
Cancer immunotherapy encompasses treatment approaches that aim to treat cancers by stimulating an immune response or by using parts of the immune system to specifically target malignancies. As mentioned before, the concept of immunotherapy has existed for over 100 years when Dr. William Coley used bacterial toxins to generate immune responses against cancers[4]. Cancer immunotherapy remained a small cult-like area of research until it experienced a renaissance in the last couple of decades mediated by scientific and technological advances, including the development of hybridoma technology, primary cell culture and expansion techniques and gene transfer systems. These advances have changed our understanding of cancer, the way fundamental therapies are viewed and have inspired the research and development of various different immunotherapy platforms. Data emerging from these approaches have taken immunotherapy into the forefront of cancer research.
6
1.2.1.1 Hybridoma Technology
In almost every area of cellular and molecular biology, mAbs have helped understand the function and interactions of proteins. In the context of cancer, this has helped uncover important protein pathways and characteristics of malignancies. They have also been used to distinguish between different types of cells to improve basic science and patient diagnosis. Clinically, they have been used to therapeutically block or activate molecules of the immune system to induce an anti-cancer immune response, or to specifically target molecules on cancerous cells to extinguish their growth and survival.
The hybridoma technology created by Köhler and Milstein in 1975 was pivotal in making antibodies invaluable research tools and the “magic bullets” of a wide variety of passive and active immunotherapies. They were able to create immortalized cell lines capable of expressing a single set of immunoglobulin genes by fusing together a mouse myeloma cell with a mouse spleen cell from an immunized donor[40]. The ability to make a specific antibody to a predetermined antigen has greatly expanded the size of antibody libraries. Hybridoma cells can be cultured in bulk, which has made antibodies more readily available across the scientific community. Hybridoma technology has greatly expanded the quality, diversity and availability of the antibody libraries available to scientists and medical practitioners.
The potential for using mAbs in the clinic was clear but so was the immunogenicity associated with injecting mAbs from a non-human host into human patients. Creating chimeric antibodies by genetically replacing the mouse Fc region with a human one fully reduced the immunogenicity in some cases[41, 42]. This strategy was taken one step further through fully ‘humanizing’ antibodies by transferring the genetic sequence of the complementary determining regions (CDRs) of a non-human antibody to the sequence of a human antibody before purification[43]. Another method tested to overcome this problem was the creation of hybridomas from human cells[44]. However, the establishment of these cells and the production of large quantities of human mAbs has proven to be difficult[42]. It is unclear whether there is a clear Food and Drug Administration (FDA) regulatory advantage for any of these different
7 approaches over the others[42]. The FDA has approved over 30 human, humanized and chimeric mAbs to date for different diseases and many more are currently being clinically tested.
Other limitations of the hybridoma technology are the time it takes to develop a novel purified mAb, and the difficulty immunizing with self-antigens. Phage display technology may overcome these limitations. Phage display expresses a heterogeneous library of antigen binding proteins on the surface of bacteriophages and then screens them against the antigen of interest. The phage that expresses the protein with the highest affinity for the antigen can be isolated by a process called bio-panning. The binding phage can then be used to express the binding protein in E. coli for the purpose of purification. The binding protein can then be characterized and used. This process is much shorter than the process of immunizing mice, collecting spleens, and fusing them to myeloma cells. Libraries can consist of random peptides, and antigen binding fragments (Fabs) or single chain variable fragments (scFvs) from collected antibody sequences. Libraries often contain billions of potential binding proteins. The size of the library is vital to the success of finding a protein that binds strongly to an antigen. Phage display technology also offers flexibility in its application. The library can be screened against whole cells to identify potential target antigens on the surface of cancer cells. Phage display is becoming a popular technology to gather binding proteins to an antigen. It might become the preferred option with the development of larger libraries and more efficient protocols. It has the potential to become a valuable screening and therapeutic tool in personalized medicine.
1.2.1.2 Primary Cell Culture and Expansion
The ability to culture and expand primary T cells ex vivo has been a big obstacle in bringing T cell based immunotherapies into the clinic. The discovery of IL-2 made the ex vivo culture of primary T cells possible [45]. Shortly after its discovery, IL-2 expanded tumour infiltrating lymphocytes (TILs) were quickly used to treat patients with advanced renal or breast cancers, melanomas, and colon carcinomas, becoming the first adoptive cell therapy to be used in the clinic[46-48]. Partial tumour regression was observed in three patients[48]. These results were met with great optimism and led to the further study of TILs and other adoptive cell therapies.
8
It has become apparent that the quality and duration of the ex vivo culture of primary cells is vital to the success of the adoptive cell therapy. The addition of anti-CD3/anti-CD28 crosslinking magnetic beads to IL-2 culturing conditions results in a greater number of T cells in a shorter period of time, with a less differentiated phenotype[49, 50]. This has become the standard approach to T cell expansion. The addition of other cytokines to create specific T cell subsets is being explored pre-clinically. The addition of IL-15 results in central memory T cell (Tcm) like characteristics by activating telomerase and decreasing telomere loss[51]. This has been shown to increase the proliferative potential and anti-tumour activity[52]. The addition of IL-7 and IL-
15 leads to a memory stem T cell (Tscm) like phenotype. Using IL-21 instead of IL-2 has been shown to minimally differentiate CD8+ T cells and lead to higher expansion potential and anti- tumour activity[53]. CD4+ T cells can be pushed towards a Th17 phenotype by culturing them with anti-CD3/anti-inducible T-cell costimulator (ICOS) magnetic beads and exogenous IL-1β, IL-6, and IL-23[54]. The use of artificial APCs (aAPCs) has been shown to be a superior culturing method than the use of magnetic beads because of their ability to support greater proliferation potential and to reduce the use of consumable materials. The K562 cell line transduced with human leukocyte antigen (HLA)-A2, CD32, CD80, CD83, CD86, CD137L, and CD252 was able to support greater T cell proliferation while removing the need for costly magnetic beads[55]. The further optimization of primary cell culturing protocols could further increase the accessibility of primary cell culture for research and clinical use.
1.2.1.3 Gene Transfer Technology
The development of safe and effective gene transfer technologies has been paramount in bringing immunotherapies from the bench-side to the clinic. There exist viral and non-viral systems for gene delivery and each possess advantages and disadvantages. Non-viral systems that use lipids or polymers to carry deoxyribonucleic acid (DNA) into cells, may be the least disruptive and immunogenic but unfortunately lack the efficiency, expression and stability needed to provide a therapeutic benefit. For therapies where cellular hereditability and long-term expression is required, viruses from the Retroviridae family have become popular vectors.
9
The first demonstration of ex vivo gene transfer in the clinic was in 1990 where the retrovirus, murine leukemia virus (MLV), was used to transduce a neomycin selection gene into patient T cells to track them after they were reinfused to treat their advanced melanomas[56]. These transduced T cells were successfully engrafted and showed long-term persistence[56]. One of the first successful therapeutic uses of gene transfer in the clinic sought to add a functional version of the IL-2 receptor subunit γ gene into autologous stem cells of patients with severe combined immunodeficiency (SCID) XI that could not find a suitable bone marrow donor[57]. Recombinant γ-retroviruses were used to transduce autologous CD34+ cells ex vivo before they were reinfused into the patient[57]. This gene therapy was able to fully restore long-term T, B and NK cell counts and their function, which provided full correction of their disease[58, 59]. However, T-lymphocyte leukemias developed in 20% of patients because of insertional mutagenesis of known oncogenes[60, 61]. This early trial of gene therapy demonstrated the potential power to ameliorate disease and the serious dangers that could arise.
Lentiviruses (LVs) are emerging as the safest and most effective retroviral option for clinical use. Several changes have been made to the LV genome in order to maximize safety. In third generation systems, the LV genome is divided into 3 or 4 different plasmids that are usually transfected into 293T cells in order to create replication incompetent LV particles. Most systems incorporate packaging, transfer and envelope plasmids. The packaging plasmid contains all structural, enzymatic and regulator elements required for viral production in trans[62]. Depending on the system, the regulatory elements might be coded for on a 4th plasmid. The transfer plasmid contains the transgene as well as the necessary cis-acting features, psi (Ψ) ribonucleic acid (RNA) packaging signal, and 3′ and modified 5′ long terminal repeat (LTR) elements[62]. This multiple plasmid system ensures that packaged LV particles can only insert the transgene and cis-acting elements into the genome of the target cell and prevents the transfer of the viral genes necessary for LV packaging. Unnecessary viral proteins have been removed from this system in order to reduce the immunogenicity of transduced cells[63]. A self- inactivating transfer vector has also been developed to further decrease the generation of replication competent LV particles. A deletion was placed in the U3 region of the 3’ LTR, which after reverse transcription and integration sits in the 5’ LTR and abrogates its promoter function[64, 65]. With these current modifications, LVs have been shown to insert in ‘hot spot’
10 locations only 8% of the time compared to 21% of the time by γ-retroviruses when transducing CD34+ cells[66]. This study also demonstrated that γ-retrovirus insertion ‘hot spots’ were enriched in proto-oncogenes and proliferation controlling genes whereas LV ‘hot spots’ were not[66]. In vivo studies of LV transduced bone marrow cells and hepatocytes have shown that transgenes were primarily inserted into active genes that were not associated with growth and did not lead to any tumour formation [67-69]. This evidence indicates a favourable risk profile and supports the notion that LVs are safer than other retroviral gene transfer systems. Various modifications and developments are being made to further enhance transduction efficiency, transgene expression, and the safety of LV systems and, therefore, the clinical utility of this technology.
Cell fate control or suicide safety elements have been developed to provide a failsafe mechanism to mitigate any adverse toxicity from adoptive cells. These systems are often based on the delivery of an enzyme with a specific mutation along with the therapeutic gene. This enzyme gives transduced cells the unique ability to convert a nontoxic pro-drug into a cytotoxic compound. This essentially gives the ability to alleviate any adverse events by killing all the transduced cells and their progeny. The herpes simplex virus (HSV)-thymidine kinase (TK) system is widely used. Cells that possess HSV-TK can convert the pro-drug ganciclovir to the cytotoxic ganciclovir-triphosphate molecule, which is incorporated into DNA and leads to DNA chain termination and cell death[70]. This system was first used in the clinic to control graft versus host disease (GVHD) from adoptive lymphocytes used to treat patients with relapsed lymphoma or leukemia should it arise. Ganciclovir-induced elimination of the transduced cells was able to effectively control GVHD in all cases where it developed[71]. There are innate problems with this system that might result in incomplete elimination of transduced cells. For one, ganciclovir-triphosphate cytotoxicity is cell-cycle dependent, which might allow non- dividing cells to survive. Furthermore, the presence of an immunogenic protein of HSV origin could lead to the clearing of transduced cells by the host’s immune system and diminish their therapeutic effect[72]. Other cell fate control systems have been developed that use mutant versions of human proteins, thymidylate kinase (TMPK) and deoxycytidine (DCK). The mutant version of TMPK has up to 200-fold greater activity in phosphorylating the pro-drug azidothymidine (AZT) to the toxic version AZT-triphosphate compared to the wildtype version
11 of TMPK[73]. This difference in activity leads to apoptosis and cell death in cells expressing mutant TMPK at concentrations of AZT that is harmless to cells that don’t express it. [73]. The DCK system uses a mutant version of DCK that was designed to have active sites that allow it to activate various clinically relevant pro-drugs including brivudine, telbivudine and bromodeoxyuridine[74]. Both of these systems use human proteins with minimal modifications and thus should have low immunogenicity. They also both activate their respective pro-drug with good safety profiles and clinically relevant kinetics, and thus, provide viable alternatives to the HSV-TK cell safety system.
Designer nucleases such as zinc finger nucleases, transcription activator-like effector nucleases and clustered regularly interspaced short palindromic repeats (CRISPR) systems provide a more precise tool for gene therapy by allowing the targeted correction of gene sequences. They all have a reduced risk of insertional mutagenesis. These techniques provide a lot of promise but are not clinically ready. Transgene delivery methods need to be optimized to achieve higher efficiencies and the potential off-target effects still need to be explored. These technologies along with the further development of gene delivery systems will increase the efficacy, safety, diversity and availability of cellular immunotherapies.
1.2.2 Cancer Immunotherapies In the Clinic
Cancer immunotherapy encompasses treatment approaches that aim to treat cancers by stimulating an immune response or by using parts of the immune system to specifically target malignancies. Many platforms have been developed and tested including immunomodulating drugs (IMiDs), immunogenic chemotherapies, cytokines, adjuvants, diverse vaccination strategies to mount cellular and/or humoral anti-tumour immune responses, mAbs to target the tumour and/or modulate the immune system, and adoptive cell therapies. These strategies have shown varying degrees of success with some showing the potential to cure patients with advanced melanomas and B cell malignancies. Many of these therapies are designed to overcome the central and peripheral tolerance that limits the effective targeting of tumour cells by the immune system. Probably the greatest clinical successes to date have been with
12 immunomodulatory mAbs and with adoptive T cell therapies. Although IMiDs, adjuvants, cytokines and vaccines have become important parts of the immunotherapy landscape this section will focus on how mAbs and T cell therapies have been used to treat cancer.
1.2.2.1 Antibody Therapies
Dr. Paul Erhlich was the inventor of chemotherapy and the father of the idea of strategic medicine. He was given the Nobel Prize for his insights into the presence of antigen-binding side chains that were present on the surface of cells and released into the bloodstream in 1908. It is now known that these side chains include a wide variety of receptors, including antibodies. In this work he also postulated the need for “magic bullets” to specifically target cancer. The ability to bind to proteins on the surface of cancer cells has made antibodies one of the “magic bullets” of immunotherapy. They have been clinically used to target tumour cells to inhibit growth and survival signals or to directly deliver a toxic payload. They have also been used to target the immune system in order to modulate regulatory systems to induce a potent anti-tumour response.
1.2.2.1.1 Targeting the Tumour with mAb
One form of passive immunotherapy uses antibodies to target the tumour and disrupt growth and survival pathways. An inherent problem with using active immunotherapies to treat patients with advanced disease is that living with cancer and experiencing various treatments has left them severely immuno-compromised. Sometimes immunotherapies are able to reverse this immunosuppression but often they fail to do so. Certain cancers will increase the expression of proteins that give them a survival or growth advantage. Naked mAbs can be used to inhibit the function of these proteins to disrupt tumour growth, and the tumour microenvironment. Targeting the tumour with mAbs can also act as an active immunotherapy by engaging mechanisms of the immune system. Depending on the mAb and the patient, the cytotoxicity of the complement system and immune effector cells can be directed onto the tumour. Cetuximab, a chimeric IgG1 and panitumumab, a fully humanized IgG2, are both epidermal growth factor receptor (EGFR) specific mAbs that are FDA approved to treat colorectal cancer. They both
13 function by interfering with ligand binding, dimerization and signal transduction of EGFR [75, 76]. However, only cetuximab recruits NK cells for antibody dependent cellular cytotoxicity (ADCC) of tumour cells in patients because of its IgG1 subtype[77]. The addition of cetuximab to chemotherapy treatment has been shown to prolong progression free survival in patients with metastatic colon cancer who have wildtype KRAS alleles to 8.9 months compared to 8.0 months in patients given chemotherapy alone[78, 79]. In a phase I trial, panitumumab monotherapy was had anti-tumour activity in 36% of patients[80]. Anti-EGFR therapies have been well tolerated despite being associated with skin rashes due to off tumour expression of EGFR. For the most part these adverse skin reactions were minor but grade 3 skin related events developed in 19% and 7% of patients given cetuximab and panitumumab, respectively [78, 80]. These are two examples of mAbs that target the tumour to interfere with survival and/or direct an immune response.
Another strategy to treat immunosuppressed patients is to couple highly cytotoxic drugs to mAbs that bind to tumour antigens, in order to directly deliver a toxic payload to the interior of cancerous cells. There are three parts to consider when designing antibody drug conjugates. The first is the antigen used to target the malignancy. It is important to consider the expression and function of the antigen. The next thing to consider is the avidity and specificity of the mAb to the antigen. It is also important to understand the effects of the binding of the mAb to the antigen. The other parts of the antibody drug conjugate are the linker and the drug. Since the drug is being delivered directly to the cancer cell it is possible to use compounds that are too toxic for systemic injection. Most commonly, microtubule inhibitor derivatives of maytansine, or auristatin that are 1000 fold more toxic than standard chemotherapies are used[81]. The linker will control the properties of payload release and must be tailored for the drug, antibody and cancer being targeted. In order for the antibody drug conjugate to be effective, the drug must be internalized and directed to the correct place for it to exert its cytotoxic effect. Over 50 antibody drug conjugates are currently being tested in clinical trials[82]. One successful example is, adcentris, a CD30 specific chimeric IgG1 mAb conjugated to monomethyl auristatin E through a cathepsin cleavable linker. It gained FDA approval to treat classical Hodgkin’s lymphoma patients with high risk of relapse and progression after a phase III trial showed that patients that received adcentris had a significantly greater mean progression free survival than those who
14 were given the placebo (43 versus 23 months)[83]. Kadcyla is a HER2 specific humanized IgG1 mAb that is connected through a non-cleavable linker to emtansine. It has been approved to treat advanced HER2+ breast cancer after a phase III trial showed that patients given Kadcyla had a greater median progression free survival compared to patients given standard therapy (9.6 versus 6.4 months)[84]. The development of antibody drug conjugates has been stalled by poor translation from animal models to human patients. Antibody drug conjugates that are highly effective in animal models often have a maximum tolerated dose that provides suboptimal therapeutic benefit in humans. Potential toxicities are often missed in mouse models because of different expression patterns, or lack of expression of the human tumour antigen in healthy murine tissue. Nonetheless, these passive immunotherapies have shown great potential to be valuable oncological tools to enhance survival with limited toxicities in immuno-compromised patients with advanced disease.
1.2.2.2 Targeting the Immune System with mAbs
Immunomodulatory mAbs re-engage the immune system by acting as antagonists to immunosuppressive molecules or by overriding them by operating as agonists to activation signals. Undoubtedly one of the most successful examples of cancer immunotherapy is the use of mAbs for immune checkpoint-blockade. Essentially they work by allowing a broad range of tumour specific T cells to overcome peripheral tolerance in order to eliminate the cancer. Ipilimumab is a human IgG1 mAb that has been approved by the FDA to treat unresectable or metastatic melanoma. It has also been approved by the FDA as an adjuvant therapy to treat microscopic disease after tumour resection in patients with melanoma. Ipilimumab binds to the T cell inhibitory receptor, cytotoxic T-lymphocyte-associated protein 4 (CTLA-4) and is capable of mounting a potent and long-term T cell mediated immune response. T cells are activated by APCs through communications at the immunological synapse. APCs will activate TCRs with specificity for peptides of foreign processed antigens displayed by MHCs on compromised cells. T cells require additional signals in the form of stimulation of CD28 and cytokines for activation[85, 86]. T cells express CD28 at the immunological synapse and CD28 is activated by CD80 or CD86 on the APC. Once this happens, CTLA-4 is expressed by the T cell, which binds with greater affinity to CD80 and CD86 and thus dampens T cell activation overtime by
15 outcompeting CD28 for its ligands[87, 88]. This acts as a built-in off switch to modulate T cell activation. CTLA-4 is also expressed on Treg cells and is necessary for their immunosuppressive effector function [89, 90]. Ipilimumab blocks this off switch on effector T cells increasing their ability to communicate with APCs. It also prevents the Treg cells’ ability to suppress tumour reactive T cells. This frees up the tumour reactive T cells to receive activation signals from APCs and to destroy tumour cells[91]. Ipilimumab gained FDA approval to treat advanced melanoma after a phase III clinical trial showed that patients who received ipilimumab regardless of whether they received the cancer vaccine, GP100, or not, had a significantly greater median overall survival than those who didn’t (10 versus 6 months)[92]. The overall survival of patients in the two ipilimumab arms almost doubled the overall survival in the GP100 alone group at 12 months (43.6%, 45.6%, and 25.3%) 18 months (30.0%, 33.2%, and 16.3%) and 24 months (21.6%, 23.5%, and 13.7%)[92]. Perhaps the most astounding results were that all of the patients who received ipilimumab who survived 24 months continued to experience a durable benefit for the remainder of the study[92]. However, there was an increased amount of grade 3 or 4 immune related adverse events in patients treated with ipilimumab but most of these were reversible[92]. There were 14 deaths associated with ipilimumab treatment and 7 were due to immune related adverse advents[92]. These results revolutionized the field by demonstrating that once immune checkpoint-blockade is engaged it can modify the immune system of the patient to provide long- term control of tumour growth even after treatment has stopped.
PD-1 is another inhibitory receptor expressed on T cells at the immunological synapse. Its ligands, PD-L1, and PD-L2, are expressed on APCs to maintain central and peripheral tolerance[20-22]. Cancerous cells often upregulate PD-1 ligands to avoid immune destruction[19]. Two mAbs directed towards PD-1, pembrolizumab and nivolumab, have gained FDA approval to treat various malignancies and more strategies are being tested to target this axis. Pembrolizumab is a humanized IgG4 mAb specific for PD-1. One trial concluded that patients given pembrolizumab compared to those given ipilimumab, had a greater 6 month progression free survival rate (47% to 27%), one year overall survival rate (71% to 58%) and complete response (CR) rate of (33% to 12%)[93]. The pembrolizumab groups also experienced fewer grade 3 to 5 adverse events (11.7% to 19.9%)[93]. Another trial showed an overall response (OR) rate of 26% in patients treated with pembrolizumab that had ipilimumab-
16 refractory advanced melanoma[94]. Nivolumab is a human IgG4 mAb specific for PD-1 and has showed equally impressive results. These antibodies that target PD-1 have gained FDA approval to treat advanced melanoma, non-small cell lung cancer and Hodgkin’s lymphoma. Their clinical benefit in treating renal cell carcinoma, colorectal cancer, prostate cancer, bladder cancer, and ovarian cancer are being explored[95-97]. Inhibiting the PD-1 axis by blocking its ligands has also been successful. The antagonistic anti-PD-L1 mAb, durvalumab has shown a lot of promise in early trials and has been granted “breakthrough therapy” status by the FDA to fast track the testing of its efficacy in treating head and neck cancer and urothelial bladder cancer. Atezolizumab, another anti-PD-L1 mAb, has also been given “breakthrough therapy” designation to fast tract its clinical testing in non-small cell lung and bladder cancers. Inhibiting both the CTLA-4 and PD-1 axes has shown promising results. A phase III trial for melanoma compared groups of patients given ipilimumab, nivolumab and ipilimumab plus nivolumab. The combination therapy showed enhanced progression free survival (11.5 months) compared to both ipilimumab (2.9 months) and nivolumab (6.9 months) monotherapies [98]. Nivolumab even seemed to benefit patients with PD-L1 negative tumours, especially when combined with ipilimumab[98]. However, the combination therapy was associated with elevated rates of grade 3 or 4 adverse events compared to the monotherapies (55% ipilimumab plus nivolumab, 27.3% ipilimumab and 16.3% nivolumab)[98]. Checkpoint-blockade has shown to be an effective immunotherapy for some advanced cancers, especially for those with high mutational burden[99]. Checkpoint-blockade allows tumour-specific T cells to generate a potent anti-tumour response by releasing the breaks that cancerous cells put on them. Other potential checkpoint targets are being explored, as well as the synergy of checkpoint-blockade with other immunotherapies.
Checkpoint inhibitors have been described as releasing the brakes of the immune system. Another strategy to overcome immunosuppression is to push the immune system’s accelerators with agonistic mAbs. CD137 or 4-1BB, is a promising target because of its role in modulating different key immune effector cells. 4-1BB is expressed on T, NK, DCs, and Treg cells upon their activation[100]. Once expressed, 4-1BB interacts with its ligand, 4-1BBL, on the surface of various APCs. In T cells, the ligation of 4-1BB causes decreased activation-induced cell death, and increased TCR signaling, survival, proliferation and effector functions[101-103]. In NK
17 cells, 4-1BB activation enhances proliferation, release of IFN-γ, and cytolytic action[104]. In DCs, its stimulation promotes maturation by upregulating CD80 and CD86 and producing IL-6 and IL-12[105]. There is also some evidence that suggests that 4-1BB stimulation can directly and indirectly inhibit Treg cells and their immunosuppressive function[106]. Two agonistic mAbs to 4-1BB are currently being tested in early clinical trials. Urelumab is a humanized IgG4 mAb being tested in combination with other therapies to treat a variety of malignancies[107]. The other is PF-05082566, a human IgG2 mAb. It has been tested as a monotherapy in a phase I trial to treat patients with advanced malignancies[107]. Although, the results have been underwhelming, no dose-limiting toxicities have been observed. Further work is needed to evaluate if 4-1BB agonists will provide value as a monotherapy and/or in combination with other therapies. Other activating receptors being explored as potential accelerators of immune effector cells are CD27, CD134, and CD357.
Modulating the immune system with mAbs is one strategy to reverse the immunosuppression associated with cancer. Immunomodulatory monoclonals have many benefits including their ability to induce long-term disease control, and be an ‘off-the-shelf’ drug in a wide variety of cancers. The fact that the therapy does not have to be tailored to the patient’s cells or accompanied by lymphodepletion and stem cell transplant makes it more attractive, bearable and affordable compared to adoptive cell therapies. However, clinical responses are only seen in a small subset of patients. While, toxicities are being better managed there still exist significant toxicities due to the broad activation of the tumour specific and nonspecific T cells. A few biomarkers have already been identified that can help identify patients who may benefit most from checkpoint-blockade. The magnitude of tumour infiltrating T cells, tumour mutation burden and PD-L1 expression have all been shown to positively correlate with the success of checkpoint-blockade[99, 108, 109]. Genetic signatures that lead to resistance to checkpoint- blockade have also been identified[110, 111]. Identifying more biomarkers that predict which patients will respond and which ones will have adverse effects will further improve their overall efficacy in the clinic, as this will facilitate clinical trials with pre-selected patients more likely to benefit from the therapy.
18
1.2.3 Adoptive Cellular Therapy
Adoptive cellular therapy involves the isolation and reinfusion of lymphocytes into patients to treat disease. Most commonly this is done with T cells, although NK cell adoptive therapies are gaining traction. DCs have also been isolated, activated and then reinfused into patients as cellular vaccines. This strategy looks to activate DCs with specific peptides so that once they are reinfused they can mount a specific T cell response against tumour cells. The only FDA approved cellular therapy is Sipuleucel-T, a DC vaccine, for the use against metastatic castration-resistant prostate cancer[112]. Adoptive T cell therapies offer the potential to overcome many limitations associated with cancer vaccines. Mainly it bypasses the requirement for de novo activation of tumour reactive T cells. Adoptive T cell therapies may also have certain advantages that may overcome the limitations of the immunomodulatory mAbs described above. Specifically adoptive cell therapy allows for a more targeted approach to overcome peripheral immunosuppression and provides the opportunity to bypass central tolerance. There are several different types of adoptive cellular therapies that have shown clinical utility.
1.2.3.1 Tumour Infiltrating Lymphocyte
TIL therapy involves the isolation and expansion of T cells that have invaded into the tumour. The rapid expansion in the presence of activating cytokines can lower the activation threshold of the tumour specific T cells that already have ability to invade the tumour. As mentioned before this started with the pioneering work by the Rosenberg group in the early 1980s[46]. The observable anti-tumour response was met with optimism but left room for improvement. Current protocols allow for rapid identification and expansion of T cells with high avidity for the patient’s tumour(s). Single T cells from the resected tumour can be expanded to therapeutic numbers in 5-6 weeks. These rapid expansion protocols have allowed T cells to retain their effector function and thus have been a key technical advancement in the improvement of TIL therapy. In recent trials, protocols using TILs to treat advanced melanoma have seen OR and CR rates of approximately 53% and 24%, respectively[113]. More encouragingly, 95% of the patients who had complete tumour regression, continued to have complete durable responses for over 5 years[114]. The use of lymphodepleting chemotherapy has significantly improved TIL therapy by increasing T cell expansion and persistence in patients[115]. Possible explanations for
19 this are the increase of homeostatic space and cytokines such as IL-7 and IL-15. It is also possible that lymphodepletion removes regulatory immune cells and the immunosuppressive cytokines associated with them. Like checkpoint-blockade, TIL therapy has shown the ability to provide long-term and durable anti-tumour T-cell responses to a subset of patients.
The success of TIL therapy has been limited to a small subset of patients with advanced melanoma. Isolating and expanding TILs with tumour specificity in other cancers have proven to be more difficult[116]. This may be due to the relatively high mutational burden and subsequent immunogenicity of melanoma compared to other cancers. Even within patients with advanced melanoma, only half have TILs present in tumours and only 81% of those have anti-tumour activity[117]. Furthermore, the most successful efforts have only given 24% of this already small group of patients a cure. It appears that in patients who respond, their TCR repertoire is more likely to be sufficient because of the high immunogenicity of their tumours. Like checkpoint- blockade, the expansion of TILs is able to overcome peripheral tolerance and seems to be successful when this is the peremptory impediment. Patients who fail may be also limited by central tolerance. For these patients, their TCR repertoires need to be expanded in a safe way to target self-antigens that are overexpressed on tumour cells. The obstacle of finding targets in tumours with low mutation burdens still needs to be overcome. The concept of engrafting patients with an enhanced TCR repertoire to target cancers is very intriguing. Demonstrating the in vivo persistence of adoptive cells was the first step. Building the synthetic repertoire is the next step in providing consistent successful tumour rejections.
1.2.3.2 TCR modified T cells
In order to provide adoptive cell therapy to a larger section of patients with melanoma and other diseases, T cells from peripheral blood have been isolated and engineered to be tumour reactive. In order to make these T cells tumour specific they can be genetically modified to express tumour reactive TCRs to known tumour antigens. High avidity TCRs can be identified and cloned from a patient who showed a robust immune response. They can also be isolated from mice with human MHCs that have been immunized with the tumour antigen of interest. One
20 benefit to using murine TCRs is that recombination with endogenous TCR genes that leads to off target toxicities or ineffective TCRs is minimized[118]. However, they are more likely to be immunogenic and become ineffective[119]. Regardless of the source, synthetic TCRs can be cloned into gene transfer vectors, typically retro or lentiviruses, and then engineered into patients’ T cells. A highly avid human TCR, DMF5, to melanoma antigen recognized by T cells (MART-1) was identified and cloned into patients’ T cells from peripheral blood for adoptive cell therapy. Objective responses were seen in 30% of patients, which were accompanied by long-term persistence of transduced T cells[120]. The efficacy of the DMF5 TCR was improved by pairing it with a DC cell vaccine pulsed with MART-1 peptides. This combination saw 69% of patients experience tumour regression[121]. Unfortunately, none of these patients experienced the long-term and complete tumour regression seen with TIL therapy. NY-ESO-1 specific TCRs have also been transduced into T cells from peripheral blood to treat advanced melanoma. Tumour regression was seen 11 out of 20 patients including 4 complete responses[122]. Three of which have continued to show durable responsex at the latest follow-up at 40-52 months [122]. NY-ESO-1 TCR engineered T cells have also had clinical success in treating synovial cell sarcomas and multiple myeloma (MM), showing clinical responses in 61% and 80%, respectively[122, 123]. Melanoma antigen gene (MAGE) family proteins A3 and A4, have also been targeted by TCR engineered T cells to treat a variety of metastatic cancers including melanoma with variable success[124, 125]. These trials contain examples of patients where TILs were not present or accessible but T cells from peripheral blood were given the ability to provide a durable and sustained anti-tumour T cell response. There are many possible explanations why they have not been as successful as TIL therapy. Firstly, beyond a tumour specific TCR, these T cells might lack activation signals that TILs have that allow entry into the tumour microenvironment. Another possibility is that although the synthetic TCRs are detected on the surface of T cells they might form chimeric TCRs by binding to the endogenous TCR chains. This would lead to inactive TCRs or even worse, TCRs with alternative specificity. This has been prevented by use of zinc finger nucleases, small interfering (si) RNA, and alterations to the constant regions of TCR chains. It is also possible that the amount of TCR molecules is not sufficient to activate the T cell. Efforts are being made to increase the expression of exogenous TCRs. It is also likely that targeting tumours through one tumour antigen is not sufficient for a complete response. Also TCR therapy requires antigen presentation on MHC and MHC loss is a common mechanism that tumours use to avoid immune destruction. Identification of more
21 tumour antigens will provide more targets and allow polyclonal TCR T cell therapies to be tested.
There are other limitations to TCR engineered T cell therapies that have prevented them from achieving their full potential. There have been severe adverse toxicities associated with every TCR therapy. This was to be expected, as breaking central tolerance can be very dangerous. This requires a thorough understanding of expression patterns to minimize and avoid toxicities. Patients given MART-1 TCR engineered T cells exhibited severe rashes in normal tissues where melanocytes were present, including skin, eyes and inner ears. A carcinoembryonic antigen (CEA) specific TCR showed indications of response potential but severe life threatening colitis presented in all patients, probably due to on-target, off-tumour activity[126]. TCRs that target MAGE family proteins showed severe neurological toxicities, including two fatal cases of periventricular leukomalacia[125]. Two patients also died from cardiac toxicities because of unexpected TCR activity[127]. All of the TCR treatments are associated with intense cytokine release syndrome (CRS) by transferred cells. For the most part this is a manageable side effect. Furthermore, each TCR can only be used in patients with the matching HLA type. This increases the amount of TCRs that need to be developed and tested in order to treat the entire patient population. Even with the limitations and adverse toxicities, genetically engineered TCR T cells have proven to be valuable tools in treating advanced cancers.
1.2.3.3 Chimeric Antigen Receptors
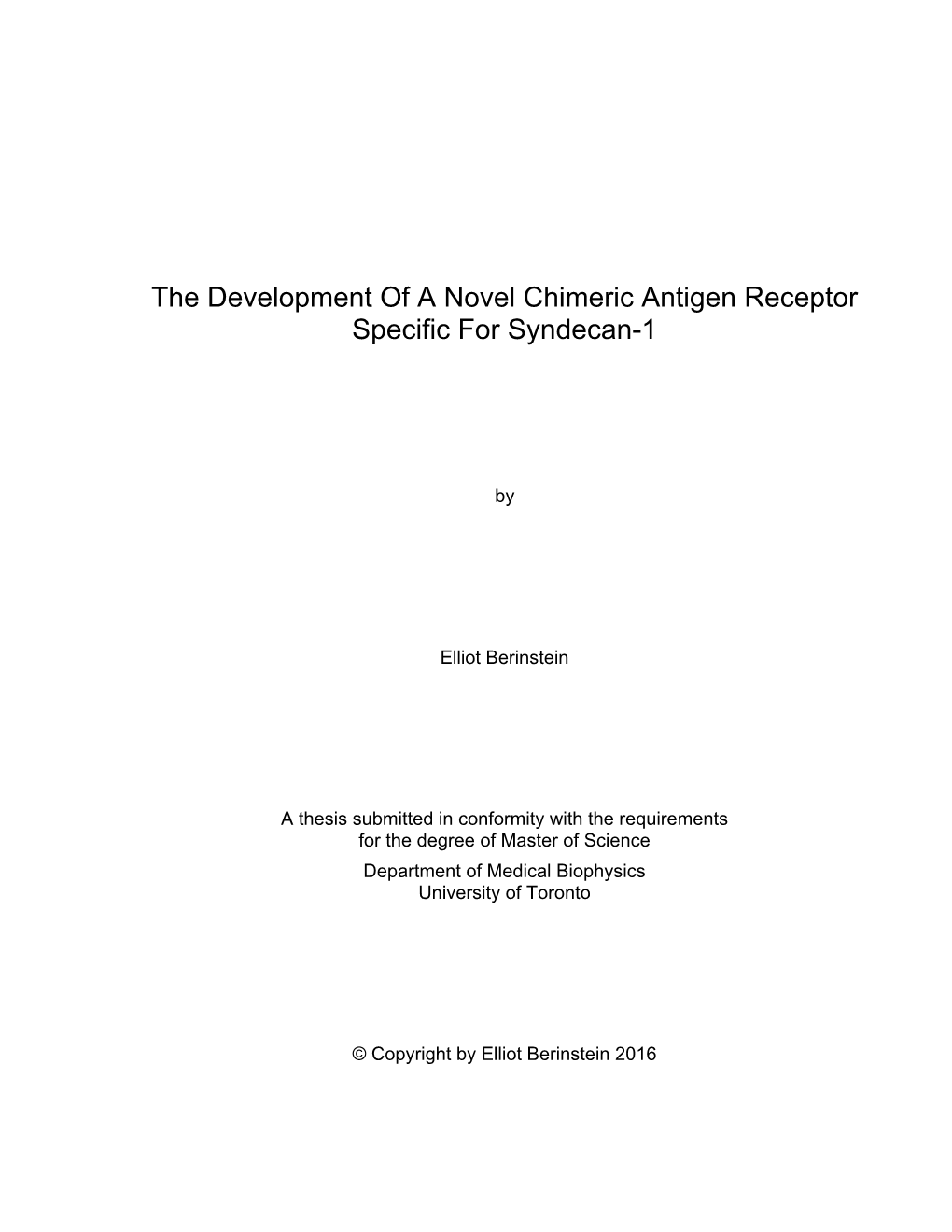
Chimeric antigen receptors (CARs) represent another tool to direct T cells to attack tumour cells and build the library of synthetic tumour targeting receptors. As demonstrated in Figure 1.1a, CARs usually consist of an extracellular antigen recognition domain derived from a scFv of a mAb linked through hinge and transmembrane domains to intracellular co-stimulatory and CD3ζ signaling domains. The antigen recognition domain targets proteins on the surface of tumour cells. One advantage of CARs is that they bypass the need for TCR-MHC interactions. This can also be a disadvantage, as it limits the targets to cell surface proteins, whereas TCRs can target intracellular proteins as well. The signaling domains work together to provide the necessary
22 activation signals to initiate the cytotoxic power of T cells. First generation CARs combined scFvs to ζ or γ activation chains[128]. The extension of the scFv with a hinge domain was shown to enhance CAR function by increasing its ability to bind to antigens[129]. Typically, domains derived from the CD8 co-receptor or from the constant regions of IgGs have been used. Many research groups prefer CD8 because it has less potential immunogenicity and a more natural function within the immunological synapse. The realization that the endogenous activation of co-stimulatory receptors were not sufficient, led to their addition to the cytoplasmic portion of CARs. Signaling domains from one of CD28, CD134 or CD137 have been used in 2nd generation CARs. This has been shown to increase the cytotoxicity, persistence and cytokine secretion of T cells[130]. Third generation CARs utilize two of these co-stimulatory domains in their constructs. Figure 1.1B shows the general configuration of the different generations of CARs. The added benefit of a second co-stimulatory domain is uncertain [131]. A new clinical trial is being undertaken with the hope to provide answers to this question by testing the ability of 2nd and 3rd generation CARs to treat non-Hodgkin’s lymphomas (NHLs) [132]. Other co- stimulatory domains have been used to explore the benefit of driving CAR T cells towards a certain phenotype[133, 134]. Armoured CARs include a separate gene that enhances T cell function or modulates the tumour microenvironment. The expression of CD40L along with a 2nd generation CAR improved endogenous and adoptive T cell function by priming CD40+ malignancies for attack and supporting DC maturation and antigen presentation[135]. Likewise, 4-1BBL co-expression has been shown to stimulate both endogenous and adoptive T cells and in doing so increases the efficacy of the anti-tumour response[136]. Another type of armoured CAR includes a gene that leads to the secretion of proinflammatory cytokines[137, 138]. Systemic injection of these cytokines often proves to be toxic. These armoured CAR T cells can home to the tumour microenvironment and provide the localized administration of cytokines to avoid systemic toxicities. For example, armoured CAR T cells that release IL-12 have been shown to have enhanced in vivo persistence due to their resistance to Treg cells and MDSCs[137].
23
Design of CARs
Extra-cellular mAb binding domain
Hinge and transmembrane domains
α β Intracellular signaling γ ε ε δ domains
Evolution of ζCARs ζ CD28 4-1BB OX40 TCR Complex CD8
1st Generation 2nd Generation 3rd Generation
Co-stimulatory domain CD3ζ Co-stimulatory CD3ζ domain X2
CD3ζ
! Cytotoxicity ! Cytotoxicity !! Cytotoxicity ! Proliferation !! Proliferation ! Cytokine secretion !! Cytokine secretion Figure 1.1. A) Shows the different! domains In vivo persistence of a CAR and their !! typical In vivo origin. persistence B) Shows the conformation of 1st, 2nd and 3rd generation CARs.
CAR research has been reinvigorated by the clinical success of CD19 specific CAR T cell adoptive therapy. Multiple groups have used 2nd and 3rd generation CD19 CAR T cells to treat a wide variety of CD19 malignancies including, B cell acute lymphoblastic leukemia (B-ALL), B cell chronic lymphocytic leukemia (B-CLL), and other NHLs. CD19 is a lineage-restricted marker and is present on normal and malignant B cells. There have been various trials that have
24 tested different CD19 CAR constructs, diseases, patient selection criteria, T cell subsets, and preconditioning regimens. CD19 CAR T cells have had the greatest success in treating adults and children with B-ALL. The first results came from a trial that used autologous T cells transduced with a CD19 specific CAR with CD28 and CD3ζ signaling domains to treat 5 adult patients with relapsed or refractory B-ALL. All 5 patients had CRs and were given minimal residual disease negative (MRD-) status[139]. Four of five of them were eligible for allogeneic stem cell transplants (allo-SCTs), which has proven to provide long-term responses for MRD- patients[139]. A follow up report at the 2015 American Society of Clinical Oncology meeting, showed that 93% of the 32 patients from this trial showed CRs [140]. Results have been just as encouraging in pediatric patients with the first report showing that 90% of the 30 patients had CRs[141]. The latest numbers presented at the 2015 American Society of Hematology conference revealed that to date, 55 of the 59 children treated with CD19 CAR T cell therapy experienced complete remissions[142]. In the context of B-ALL, CAR T cells have proven to be an extremely effective tool to bridge patients to allo-SCT and to durable remissions. Results in treating B-CLL are more modest but still impressive with the biggest trial showing OR and CR rates of 58% and 29% respectively[143]. Although the response rates were not as high as in B- ALL, it was very encouraging that of the 4 complete responders from this trial, 2 continued to have durable responses and CAR T cell persistence for over 5 years[143]. This evidence of adoptive T cell persistence indicates that CAR therapy could provide more than a bridge to other proven therapies. CD19 CAR therapy has also had success in treating a variety of lymphomas. One trial that focused on other NHLs showed CR rates of 53%[144]. Another trial administered CAR T cells immediately after allo-SCT in patients with aggressive NHLs. Five of the eight patients continued to show CRs at their latest follow-up at 11-18 months after CAR T cell infusions[145]. It is very encouraging that studies with different CAR designs, patient groups and preconditioning regimens have all yielded positive results. Even more encouraging, is the durable remissions observed in some patients without additional therapy.
Understanding why some patients experience long-term CAR T cell persistence and remission requires further study. Durable remissions only occur in 50% of patients with B-ALL[142]. Most of the time patients relapse with CD19- disease[142]. There have also been documented cases of relapsed disease with alternative splice variants of CD19 that lack the exon containing the
25 epitope of the scFv in the CAR[146]. These relapses show the limitations of a single target approach no matter how potent it is. They also give credence to the development of other CARs to target malignancies of the B cell compartment. CD20 and CD22 show similar expression profiles as CD19. At the very least they could provide a tool to treat relapsed disease, especially in patients who have previously demonstrated the in vivo proliferation and persistence of adoptive T cells necessary for an effective CAR T cell response.
The most common and serious toxicity associated with CD19 directed CAR therapy is CRS. All patients experienced some sort of symptoms due to CRS. The severity of CRS can range from mild flu like symptoms and reversible neurological conditions to more life threatening ones such as vascular leak and multi-organ dysfunction. CRS is caused by a high level of T cell proliferation that results in significant production of inflammatory cytokines, specifically IL-6, IL-10, and IFN-γ[147]. The combination of ventilator support, vasopressors, corticosteroids and an anti-IL-6 receptor antibody, tocilizumab, have proven to be effective in managing most severe cases of CRS[148]. There is mixed evidence on whether the severity of CRS is linked to the degree of disease burden or not. It does seem to be a requisite side effect to T cell therapies. Therefore, it is important for clinicians to understand CRS and to be prepared to best manage the symptoms.
Perhaps the biggest limitation of CAR therapy is the lack of tumour-restricted antigens. CD19 is not tumour restricted but it is limited to a cell compartment whose function is replaceable. B cell aplasia is a necessary side effect of CD19 CAR therapy and is often used as an indication of CAR T cell persistence. It is considered an on-target but off-tumour toxicity. B cell aplasia can be managed by the administration of replacement immunoglobulins. The long-term consequences of B cell aplasia need to be monitored in future follow ups to be fully understood. Targeting a more vital lineage such as the T cell compartment or an organ is not possible. It is hard to predict the on-target but off-tumour toxicities due to the different expression levels across different tissues. HER2 was predicted to be a viable target because it is drastically overexpressed in some tumours and mAb treatments have been well tolerated. However, HER2 CAR T cell therapy led to acute respiratory failure, which eventually was fatal[149]. This resulted in the
26 termination of the trial. Likewise, carbonic anhydrase IX targeting seemed attractive but led to severe liver toxicities forcing abolition of treatment with corticosteroids[150]. There have been trials using other antigens to target various solid and hematological malignancies. These trials have either had intolerable toxicities or unsatisfactory efficacy. The therapeutic window has proven to be a lot smaller for cancers outside of the B cell compartment. Theoretically it is possible to safely target antigens that are overexpressed on tumours by fine-tuning the avidity of the antigen binding domain to only bind to cells with high expression of the antigen. This might lead to more cases of tumour escape or be logistically impossible because of the variation between patients. Another strategy is to employ cell fate systems into CAR therapies to be able to abruptly halt them if signs of toxicities appear. However, this is a reactive measure instead of a proactive one. This mechanism is also not ideal because it abolishes the anti-tumour activity to prevent toxicities. Another safety mechanism being developed for CAR therapy is a remote control tunable system based on the small molecule-mediated dimerization of two separate proteins. The presence of the dimerizing small molecule effectively turns the CAR on in a dose- dependent manner[151]. There has also been preclinical work to design safer CARs systems that require combination antigen recognition. One strategy is to separate the co-stimulatory and CD3ζ chain into two separate CARs that target different antigens[152]. Another dual receptor system was able to target tumours with more precision by using combination antigen sensing circuits. The first receptor targets the more widely expressed tumour antigen and once ligation occurs, a signal is initiated that leads to the expression of a 2nd receptor, which would be a traditional CAR[153]. These systems require the presence of two tumour antigens to activate CAR T cells instead of one. This would make CAR T cells more tumour specific and limit the on target toxicities in healthy tissue. However, there is evidence that in these systems, tissue that expresses both tumour antigens act like secondary lymphoid organs where T cells can activate and recharge. Activated T cells are then capable of targeting tissues with only one of the two antigens. A potentially more effective system is the expression of an inhibitory CAR (iCAR) along with traditional ones. The iCAR suppresses T cell activity in the presence of a specific antigen that is only expressed on healthy tissue. The iCAR uses CTLA-4 and PD-1 signaling domains to suppress T cell activity[154]. These iCARs are able to provide a dominant inhibitory signal that depends on the balance of the inhibitory and activating molecules. Furthermore, this inhibition was reversible and transient. This effectively allowed the adoptive T cells to avoid healthy tissue with both antigens while targeting tissue with the tumour antigen. This resulted in
27 a dynamic process that improved CAR T cell precision. All of these systems allow T cells to be given a more complex set instructions to better recognize cancer cells and limit off tumour toxicities.
There has been some debate about whether CAR therapy can be extended to other cancers. B cell malignancies have proven to be a viable target for CAR therapy for many reasons. Mainly, the lack of tumour-restricted antigen limits our targets to tumour antigens that are shared with healthy tissue. Unlike other compartments, the function of B cells can be replaced with medication. This allows CD19 CARs to wipe out the entire healthy compartment along with the malignancy. This is not possible in cancers arising from more vital cell lineages. B cell malignancies also tend to share more than just the expression of CD19 with their healthy counterparts. Healthy B cells work in concert with T cells to provide adaptive immunity to the host. They can act as APCs to T cells to help augment a T cell response. Malignant cells often retain the cellular machinery to present antigens and the co-stimulatory molecules to activate T cells making them ideal targets for T cell therapy. Further to this point, it is known that cancers can use B cells to polarize the cellular immune response towards Th2 cells in order to suppress the anti-tumour response. Therefore, destroying the B cell compartment might allow a Th1 response to occur that supports adoptive T cell persistence and function in vivo. One of hypotheses to why a CD19 CAR was able to provide a durable response to a patient with MM whose malignancy consisted of 0.5% CD19+ cells was that elimination of the B cell compartment improved the effectiveness of the anti-tumour immune response by removing the B cell mediated immune tolerance[155]. It is also the rationale for pairing a CD19 CAR with a mesothelin-specific CAR in an upcoming clinical trial for pancreatic cancers[156]. Finally, other than a lack of viable targets, CAR T cells have had difficulty treating solid tumours because of the poor penetration and persistence in the tumour microenvironment. Armoured CARs and checkpoint-blockade combination therapy hope to help T cells overcome the peripheral tolerance associated with solid tumours. CARs are also being developed to target tumour associated cells via vascular endothelial growth factor receptor-2 (VEGFR-2) and fibroblast activation protein (FAP) to help increase penetration of T cells into the tumour microenvironment.
28
1.2.3.4 NK Adoptive Cellular Therapies
NK cells are another cell type being used for anti-cancer adoptive cell therapies. There are several advantages for using NK cells over T lymphocytes. Primarily, NK cells have spontaneous cytotoxic activity against cancerous cells and have multiple mechanisms to detect malignancies. NK cells have been shown to be able to serially kill tumour cells [157]. As no such evidence of this ability in T cells exists, NK cells may be more efficient cancer killers. On top of their lytic potential, NK cells can also support an endogenous T cell response by releasing
IFN-γ to promote DC maturation, Th1 polarization and CTL differentiation[158]. As mentioned before, immunomodulatory and tumour targeting mAbs rely on the stimulation of NK cells as part of their anti-tumour activity. The first adoptive NK cell therapy involved reinfused lymphokine-activated killer cells to treat metastatic cancers in the 1980s. The IL-2 activated autologous NK cell reinfusions saw objective responses in 11 of 25 patients[159]. However, this therapy was limited by the toxicity of the high dose of IL-2 that accompanied the infusions[159]. Haploidentical NK cells were shown to have increased benefit if there was a killer cell immunoglobulin-like receptor (KIR) mismatch with the donor and the recipient because of an alloantigen-specific response[160]. Three out of four patients with KIR mismatched donors showed CRs, whereas only 2 out of 15 without KIR mismatch experienced a CR[160]. One patient even showed persistence and expansion of grafted NK cells showing the potential to provide long-term disease control[160]. Not only do allogeneic NK cells provide greater anti- cancer activity, but they also allow for a higher flexibility in the selection of donor cells and for cryopreservation, both of which permit the immediate administration of cells to patients. Additionally, adoptive NK cell therapies have not been associated with CRS [161]. It is possible that this is because of their distinct cytokine profile that does not include the proinflammatory cytokines associated with T cells. Peripheral blood derived NK cells have also been tested as effector cells for various CAR constructs[162]. It is clear that CARs can specifically direct the lytic ability of NK cells but it is unclear if this strategy provides an advantage over CAR T cells in preclinical models[162]. Two different pilot trials are testing haploidentical CD19 CAR NK cells in the clinic but results have not been published[163, 164].
29
Adoptive NK cell therapies have been limited by the ability to expand them to the required numbers for clinical application. The development of NK specific aAPCs has helped overcome this problem[165]. Genetically engineering primary NK cells has also proven to be difficult even with viral vectors[161]. One intriguing option to bypass these obstacles is using cytotoxic NK cell lines. The NK-92 cell line is the most developed one being tested. The NK-92 cell line was derived from a 50 year old male with a rapidly progressing NK cell lymphoma[166]. The NK-92 cell line has been shown to have robust and consistent cytotoxicity against various cancer cell lines[166]. NK-92 cells have been shown to have anti-tumour activity and acceptable tolerability in phase I clinical trials[167, 168]. One trial saw 75% of patients have an anti-tumour response[168]. It is also possible to genetically engineer these immortalized cell lines because it is easier to culture and sort them. This has led to the exploration of genetically engineered NK- 92 cells with various anti-cancer receptors. A high affinity variant Fc receptor, CD16 F158V, has been transduced into NK-92 cells and is being tested with mAbs in clinical trials[169, 170]. CAR engineered NK-92 cells have also been explored preclinically and have shown enhanced antigen specific cytotoxicity[162]. Furthermore, it is estimated that NK-92 therapy is approximately 10 fold cheaper than using primary cells[171]. The main limitation of this approach is the need to prevent in vivo persistence and proliferation of infused cells because of their malignant origin. Irradiation has shown to prevent this while maintaining their anti-cancer cytotoxicity[172]. It is unlikely that this approach will directly provide long-term disease control. Nonetheless, the NK- 92 cell line provides a more affordable, off-the-shelf platform to target tumours through various mechanisms.
1.3 Multiple Myeloma
1.3.1 Biology Of Multiple Myeloma
Multiple myeloma (MM) is a type of cancer characterized by the uncontrolled proliferation of clonal plasma cells (PCs) in the bone marrow. These cancerous PCs are called myeloma cells. The myeloma cells secrete monoclonal immunoglobulins that can be detected in the blood or urine. The expansion of myeloma cells in the bone marrow often compromises the development of other hematopoietic cells. The expansion can also offset the balance of minerals, leading to anemia and weak and damaged bones and kidneys. MM is the second most common
30 hematopoietic cancer after NHL. Approximately 2700 Canadians were diagnosed with MM and 1400 succumbed to the disease in 2015 [1]. Novel therapies have increased the median survival from 3 to 6 years in the past two decades[173]. The 5 year survival is still only 45% showing a need for novel therapies[1].
1.3.2 Standard Therapy For Multiple Myeloma
The most effective treatment for patients with MM is myeoloablative high-dose melphalan therapy (200mg/m2) with autologous stem cell transplant[174]. However, not all of the elderly patients can tolerate the toxic effects associated with high dose melphalan treatment and transplantation. Patient eligibility must be assessed based on age, absence of heart, lung, liver and kidney dysfunction and other uncontrolled comorbidities such as diabetes. Autologous stem cell transplantation may improve outcomes but is not curative and all patients will eventually relapse. Combining one or more of the novel IMiDs such as thalidomide and lenalidomide, and novel proteasome inhibitors, including bortezomib, with standard drugs such as cyclophosphamide, dexamethasone, and doxorubicin has further increased the effectiveness of this first line therapy and has led to higher remission rates[175]. Patients who are not eligible for transplant must put an emphasis on tolerability of treatment to minimize excessive morbidity and mortality. Response quality has been shown to increase over time so treatment is often given in cycles to this group[176]. Quality of life and drug tolerability are major factors for this patient group when treating this incurable disease. Using a combination of low dose melphalan, prednisone, bortezomib, thalidomide and/or lenalidomide has shown to prolong the life of transplant ineligible patients. Finally, the last thing to consider in treating patients is maintenance therapy. The development of novel drugs with lower toxicity profiles has resulted in maintenance therapy becoming more popular. Multiple meta-analyses of trial results for transplantation eligible patients showed a benefit in progression-free and overall survival when thalidomide maintenance therapy was administered versus no maintenance therapy[177-179]. Two phase III trials showed significant prolonged survival when patients were treated with lenalidomide maintenance therapy compared to a placebo after high dose melphalan therapy and transplant[180, 181]. The low toxicity of this drug has allowed it to be tested as a maintenance therapy in elderly patients not eligible for transplant and showed a significantly prolonged
31 progression free survival but no overall survival benefit was observed[182]. The value of maintenance therapy is still debated as the increase in progression free survival must be weighed against the quality of life of patients. Novel immunotherapies including IMiDs have already become a key part of treating and improving both the length and quality of life of patients. Novel therapies specifically immunotherapies have shown a lot of promise to have a profound impact on how MM will be treated.
1.3.3 Tumour Associated Antigens for immunotherapy in Multiple Myeloma
The most important step in designing a targeted immunotherapy is picking an antigen that allows for the effective targeting of the disease with limited toxicities. There have not been any tumour- restricted antigens identified in MM. However, there are some tumour-associated antigens that could prove to be viable targets for the treatment of MM.
1.3.3.1 Cyclic ADP Ribose Hydrolase (CD38)
CD38 is a small multifunctional glycoprotein widely expressed on lymphoid and myeloid lineages[183]. It is an attractive antigen because it is highly expressed on MM cells in about 80% of patients[184]. Its expression on activated T and NK cells makes it less attractive for active immunotherapies. Nonetheless, a fully humanized IgG1 anti-CD38 mAb, daratumumab, has been shown to be effective in utilizing ADCC, complement dependent cytotoxicity (CDC) and antibody dependent cellular phagocytosis (ADCP) to target MM cells[185]. A second IgG1 mAb specific for CD38, SAR65098, has been shown to have effective anti-MM activity preclinically[186]. Both mAbs have shown clinical responses in about 30% of patients when used alone[187, 188]. Furthermore, they have both shown impressive clinical results when paired with lenalidomide with OR rates being around 70% for each combination [189, 190]. The anti- tumour potential of CD38 CAR T cells has been demonstrated in mouse models for B-NHL and it is appealing to test them in MM models[191].
32
1.3.3.2 TNF Receptor Superfamily Member 5 (CD40)
CD40 is a glycoprotein involved in the co-stimulation and activation of immune cells. It is expressed on B cells, PCs and DCs. CD40 expression on MM cells is considerably elevated and plays a role in tumour growth and migration through autocrine IL-6 stimulation[192, 193]. Two different antibodies have shown anti-MM clinical activity. The first being dacetuzumab, a non- blocking, partial agonistic humanized IgG1 mAb[194]. It has been shown to initiate ADCC, while also upregulating cytotoxic ligands and suppressing IL-6 receptor expression on MM cells[195, 196]. A phase I trial using dacetuzumab monotherapy showed acceptable safety profiles but modest clinical benefit with only 20% of patients achieving stable disease (SD) [197]. Another phase I trial combining dacetuzumab with lenalidomide and dexamethasone showed tolerable adverse toxicities and enhanced clinical activity with OR and SD rates being 39% and 30%, respectively[198]. Lucatumumab is another fully humanized IgG1 CD40 specific mAb. Unlike dacetuzumab it is an antagonistic mAb that blocks interactions between CD40 and its ligands and mediates ADCC[199]. In a phase I trial that treated 28 patients with dacetuzumab monotherapy, 1 patient had a partial response (PR) and 12 achieved SD[200]. It could potentially be amplified with a combination of lenalidomide and dexamethasone. Dose limiting toxicities were seen in the form of grade 3 and 4 elevations of amylase, lipase and liver enzymes, which could limit using it to target more potent therapies such as CAR T cells.
1.3.3.3 NCAM1 (CD56)
CD56 is a glycoprotein that plays a role in cell-to-cell adhesion in neurons, glia, smooth muscle and NK cells along with specific subsets of T cells. CD56 is oddly expressed on malignant PCs and not on healthy ones[201]. Even with its broad expression, CD56 has become a popular target of MM therapies. A humanized IgG1 anti-CD56 mAb, lorvotuzumab, conjugated with maytansine (DM1) showed selective killing of CD56+ MM cells in vitro and showed a survival advantage in mouse models[202]. A phase I trial showed no dose limiting toxicities while providing 50% of patients with an OR when used in combination with lenolidomide and dexamethasone[203]. Anti-CD56 CAR T cells have shown good anti-MM activity in mouse models. CD56 directed therapies have shown promise but their potency may ultimately be limited by their off tumour toxicities.
33
1.3.3.4 HLA-DR Antigens-Associated Invariant Chain (CD74)
CD74 helps direct the α and β chains of class II MHCs to the cell surface[204]. CD74 expression is limited to B cells, macrophages, DCs, Langerhan cells and activated T cells[205]. CD74 expression is observed in approximately 80% of cases of MM, with most expressing moderate to high levels in the majority of malignant PCs[206]. A humanized IgG1 mAb specific for CD74, milatuzumab, has been shown to inhibit the growth of MM cells by blocking the receptor function of CD74[206]. Only 26% of patients with MM achieved SD after monotherapy with milatuzumab in a phase I trial[207]. CD74 is also rapidly internalized and recycled upon milatuzumab binding, making it an attractive target for antibody drug conjugate therapy. A milatuzumab–doxorubicins antibody drug conjugate phase I/II trial is currently underway but no results have been published[208].
1.3.3.5 Syndecan-1 (CD138)
CD138 is a heparin sulfate proteoglycan that belongs to the syndecan family. The ectodomain consists of a core protein with glycosaminoglycan sites that bear heparin sulfate and chondroitin sulfate chains. The intracellular portion consists of highly conserved signaling domains. CD138 has many functions that have been implicated in adhesion, growth, survival and invasion of MM cells. The heparin sulfate chains have been shown play a big role in adhesion to the microenvironment by binding to collagen and fibronectin[209]. The heparin sulfate chains also tune membrane signaling by binding to extracellular ligands and controlling their concentration [210]. CD138 also regulates the concentration of intracellular ligands by mediating their internalization via lipid raft dependent endocytosis[211]. Internalized CD138 has been shown to direct the shuttling of the marcomolecular cargo to lysosomes, and exosomes, and to the cytosol and the nucleus. The ectodomain of CD138 can also be shed into the tumour microenvironment to further modulate the concentration of growth factors[212]. This has been associated with angiogenesis and a more aggressive and invasive phenotype[212, 213]. The nuclear translocation of CD138 has also been shown to induce proliferation and differentiation[214]. CD138 is expressed on most malignant and normal PCs and absent from other hematopoietic cells in 100%
34 of patients[215]. For this reason, CD138 is widely considered to be a sensitive and specific marker for PCs and is used as a diagnostic marker to identify and quantify MM cells[216]. However, it is also expressed on the basolateral side of epithelial cells which could lead to on target toxicities. Nevertheless, a CD138 specific mAb, indatuximab, conjugated with the maytansinoid derivative, DM4, was well tolerated in a phase I/IIa trial involving MM patients[217]. This treatment was also effective with 28 out of 36 patients experiencing an OR. However, only 3 patients had CRs. There is hope that cellular therapies targeting this protein could have more potency and durability against this disease. CD138 is being used as a target in CAR T cell therapy to treat MM in a phase I/II trial[218]. So far the anti-tumour activity of these CAR T cells has been limited to date with 4 of 5 patients showing SD ranging for 3-7 months but no severe toxicities were observed[219]. The tolerability of CD138 targeted therapies along with its expression pattern makes it one of the more desirable targets on MM.
1.3.3.6 B Cell Maturation Antigen (CD269)
CD269 is expressed on maturing B cells and PCs[220]. It is also expressed on MM cells. CD269 provides anti-apoptotic and proliferation signals through interaction with its ligands[221]. A humanized IgG1 mAb conjugated with monomethyl auristatin F (MMAF), GSK2857916, has been shown to have anti-MM activity through the antagonism of its receptor function, internalization of MMAF, and initiation of ADCC and ADCP[222]. GSK2857916 is currently being investigated in a phase I trial [223]. CD269 specific CAR T cells are also being clinically developed and a phase I trial has shown promising results with both the patients treated at the highest dose level having CRs [224]. CD269 is a very promising target for immunotherapies.
1.3.3.7 SLAMF7 (CD319)
CD319 is an immunoglobulin like protein that plays a role in adhesion of various lymphoid and myeloid cells, including PCs, DCs, T, NK and NKT cells[225]. Like CD138, it is a robust marker for normal and malignant PCs[226]. It promotes growth of MM cells by mediating adhesion to bone marrow stromal cells[227]. A humanized IgG1 mAb, elotuzumab, has shown significant preclinical ability to induce ADCC and CDC against MM cells[227]. In a phase II
35 trial for refractory MM, the group of patients given elotuzumab, lenalidomide and dexamethasone had a better OR rate than the group given only lenalidomide and dexamethasone (79% versus 66%)[228]. A CD319 specific CAR has been shown to enhance the specific cytotoxicity of NK and T cells in preclinical models[229, 230]. Off tumour expression of CD319 on immune effector cells does not appear to limit the potential to direct active immunotherapies. Its high and broad expression across patients, as well as its stable expression makes it an attractive antigen to target.
1.4 Rationale
MM is an incurable disease characterized by the uncontrolled proliferation of clonal PCs in the bone marrow. There has been great improvements in the standard of care in the last 20 years but the 5 year survival is still only 45%[1]. Bone marrow transplants have been shown to prolong the life of patients with MM but all patients eventually relapse. Furthermore, there is a large subset of patients that are not eligible for bone marrow transplants. There is a need for novel therapies that not only increase the survival rates but also decrease the morbidity. The majority of resources have gone into developing novel antibody therapies that target the disease. Although these results have shown great potential, the most encouraging results have come from cellular therapies. A recent phase I/II, treating patients with autologous T cells from peripheral blood engineered to express a NY-ESO-1 TCR showed encouraging results. Out of 20 patients, 2 had CRs, 14 had near CRs and 2 more had PRs[123]. Ten of these patients showed no sign of progression after 1 year. Autologous T cells engineered with a CD19 specific CAR led to a CR with no evidence of progression or signs of disease 12 months after treatment in one patient[155]. Although only 1 out of 10 patients showed a CR this result is remarkable considering that less than 1% of the patient’s cancer was CD19+. Another group isolated T cells from the bone marrow of patients for adoptive cell therapy because it is the tumour microenvironment of MM[231]. These marrow-infiltrating lymphocytes gave 27% of patients a CR and another 27% a PR [231]. Given that the function of PCs is replaceable, and the natural ability of lymphocytes to enter the bone marrow, cellular therapies could represent the best chance to provide a cure to this disease.
36
1.5 Purpose and Specific Aims
Purpose: The purpose of this project is to develop a CD138 specific CAR from a novel antibody. CD138 was chosen because of its broad expression across patients, along with its absence from key immune effector cell populations. Although a CD138 CAR already exists, the experience with CD19 CARs has taught us that there can be benefit to having multiple CARs to the target the same antigen. Multiple CARs could help ascertain the optimal epitope. Distal epitopes have been shown to have increased accessibility but might be less effective because of the large distance between the effector and target cell upon binding. So far the balance between these factors has been determined on an antigen-to-antigen basis through trial and error. Furthermore, having multiple CARs could help avoid the immunogenicity and anaphylaxis associated with multiple infusions of T cells expressing the same CAR, and provide an option to target the relapse of clones with variants of the antigen. CD138 specific CARs could provide valuable tools to treat patients with MM and other CD138+ diseases.
Specific Aims:
1.) Generate novel mAbs specific for the extracellular portion of the core protein of CD138
2.) Design a second generation CAR using the scFv from a novel mAb as the antigen recognition domain and produce a lentiviral vector for this construct.
3.) Test the functional ability of this CAR to recognize CD138+ cells, and to initiate activation signals to enhance CD138 specific cytotoxicity
Chapter 2 Methods 2 Methods 2.1 Antibody Purification
Hybridoma cells were cultured in Roswell Park Memorial Institute (RPMI) media supplemented with 10% fetal bovine serum and adapted to grow in serum free CD hybridoma AGT media (Thermo Scientific, Cat#12372017). Once cells were growing in serum free hybridoma media, they were seeded at a cell density of 0.3x106 viable cells/mL and grown until cells reached 1x106 viable cells/mL. Once cell growth was consistent for 3-5 passages cultures were expanded to 1L. The supernatant was collected once the cell viability reached 40%. The supernatant was centrifuged at 3000g for 30 minutes (min) to remove all precipitate. Antibody was then precipitated out of the supernatant by adding 1L (NH4)2SO4 (730.5g/L) drop wise at 4°C. The supernatant was centrifuged for 30 min at 3000g and the pelleted antibody was resuspended in 10mL of phosphate-buffered saline (PBS). The antibody solution was dialyzed in PBS overnight. The dialyzed antibody solution was centrifuged at 2000 rotations per minute (rpm) for 10 min and the supernatant was collected and run through a High Trap Protein G column – 5 mL (GE Healthcare Life Sciences, Cat# 17-0405-01) to purify and concentrate the antibody.
2.2 CD138 Overexpression Cell Lines
The syndecan-1 sequence was synthesized by Genscript and then subcloned into a pDY vector. The pDY syndecan-1 plasmid was transfected along with pCMV, pMDG and pADV into 293T cells. The supernatant was collected 36 hours (h) and 60 h after transfection and concentrated by centrifugation at 19000 rpm. Jurkat and OCI AML-1 cells were transduced with the concentrated LV at a multiplicity of infection (MOI) of 10. Cells expressing syndecan-1 were detected by staining with the CD138 specific antibody, MI15 (BD Biosciences, Cat#551902), and then CD138+ cells were sorted for by fluorescence-activated cell sorting (FACS) twice.
37 38
2.3 Flow Cytometry
Cells were isolated from in vitro cultures and washed once in FACS buffer, PBS supplemented with 2% fetal bovine serum, ethylenediaminetetraacetic acid (EDTA) and sodium azide. The cells were then stained with 0.5µg of MI15 mAb, and with 0.5µg of the mAbs purified from the hybridoma clones 3E9B6, 8C1D12, and 3G1D1 for 30 min at 4°C. Cells were then stained with an allophycocyanin conjugated goat anti-mouse heavy and light chain polyclonal antibody (Thermo Scientific, Cat #A-865) for 30 min at 4°C. Cells were washed 2 times in FACS buffer and then fixed in 1% paraformaldehyde (PFA). Flow cytometry was preformed on a FACS Caliber and then analyzed on Flow Jo 9.2.
2.4 Growth Assays
50,000 cells were seeded in 200µL of growth media supplemented with 5µg/mL of 3E9B6, isotype control or an equivalent volume of PBS. Cells were cultured in triplicate in 48 well plates. At their respective time points, each well was mixed by pipetting and collected for counting. Cells were collected at 48 h and 96 h after seeding.
2.5 Proteome Profiler Human Phospho-Kinase Array Kit
RPMI 8226 cells were grown in the normal growth media supplemented with 5µg/mL of IgG2 nonspecific mAb 5µg/ml of 3E9B6 mAb for 30 min at 37°C. Cell lysates were prepared and run on a Proteome Profiler Human Phospho-Kinase Array Kit (R and D systems, Cat# ARY003B). 400 µg of cell lysates were incubated overnight with the Human Phospho-Kinase array. The array was washed to remove unbound proteins. The array was then incubated with a cocktail of biotinylated detection antibodies. Horseradish peroxidase conjugated streptavidin and chemiluminescent detection reagents were applied and a signal was determined that corresponds to the amount of the respective bound phosphorylated protein.
39
2.6 Western blots
Cells were lysed in radioimmunoprecipitation assay buffer supplemented with 1mM sodium orthovanadate and phosphatase and protease cocktail inhibitors. Cells were lysed for 30 min on ice and then centrifuged at 4°C for 10 min at 14000 rpm. Supernatants were collected and stored at -80°C. Cell lysates were normalized based on number of NK-92 cells or protein concentration. Lysates were run on a 12% sodium dodecyl sulphate (SDS) gel and transferred to a polyvinylidene difluoride (PVDF) membrane. Membranes were blocked with tris-buffered saline (TBS) supplemented with 5% bovine serum albumin (BSA) and 0.1% tween. The PVDF membrane was then stained with primary antibody for 18 h at 4°C. Membranes were washed and stained with a horse radish peroxidase conjugated anti-mouse or anti-rabbit antibody for 18 h at 4°C. Chemiluminescent detection reagents were applied to the membrane and a signal was collected on X-ray film.
2.7 Gene Sequencing
Cells were isolated from in vitro cultures and washed once in PBS. RNA was extracted from cells using TRIzol (Thermo Fisher Scientific, Cat# 15596018) and then reverse transcribed using oligomer T primers. Heavy chain genes were specifically amplified in a polymerase chain reaction (PCR) using the degenerate forward primer 5’ GCT TAC GTC GAC SAR GTN MAG CTG SAG SAG TC and the reverse primer 5’ GGA AGA TCT ATA GAC AGA TGG GGG TGT CGT TTT GGC. Light chain genes were amplified in a PCR using the degenerate forward degenerate primer 5’ CGC CCG GAA GTC GAY ATT GTG MTS ACM CAR WCT MCA and the reverse primer 5 ‘ GGA AGA TCT GGA TAC AGT TGG TGC AGC ATC. Each PCR reaction contained: 0.2mM of each primer, 1 µg of complementary DNA, 0.2 mM deoxynucleoside triphosphates, 1x platinum Taq polymerase buffer, 1.5 mM magnesium dichloride, and 1 U Platinum Taq polymerase (Thermo Fisher Scientific, Cat# 10966018), in a 50 µL reaction. Cycling conditions were: initial melt at 94°C for 2 min followed by 30 cycles of a three-step program consisting of 30 sec at 94°C; 30 sec at 51.5°C; and 40 sec at 72°C. The reactions were then held at 72°C for 2 min and cooled to 4°C. Reactions were then gel purified from a 1.8% agarose gel and digested with Sal1 and BglII for heavy chains and EcoR1 and BglII for light chains for 1 h at 37°C. Reactions were then column purified and ligated into pBluescript
40 and transformed into XL gold cells. Plasmid DNA was then sent to The Centre For Applied Genomics for Sanger sequencing. Results were analyzed and the heavy chain and light chain sequences were compiled and compared.
2.8 Chimeric Antigen Receptor Lentiviral Design and Production
The 3E9B6 HL CAR sequence was designed to have a CD8 leader sequence (amino acids, 1-23), scFv grafted with the protein L binding sequence, DVQMTQSPASLSVSVGETVTITC, in the framework (FR) 1 region, CD8 hinge domain (amino acids, 117-183), CD8 transmembrane domain (amino acids, 184-203), CD137 (amino acids, 214-255) signaling domain, and CD3ζ, also known as, CD247 (amino acids, 52-164) signaling domain. This sequence was synthesized by Genscript and then subcloned into a pDY vector already containing an internal ribosome entry site (IRES) followed by enhanced green fluorescent protein (eGFP) by using EcoR1 and BamH1 restriction enzymes. The pDY 3E9B6 HL CAR IRES eGFP was transfected along with pCMV, pMDG and pADV into 293T cells. The supernatant was collected 36 h and 60 h after transfection and concentrated by centrifugation at 19000 rpm. The concentration of functional LV particles was determined by transducing a titrated amount of the LV into 293T cells and measuring the amount of eGFP positive cells.
2.9 NK-92 Transduction
NK-92 (5x105) cells were isolated from in vitro cultures. Cells were washed and suspended in growth media supplemented with 25 MOI of LV, 8 µg /mL of protamine sulfate and 6µM of BX795 (TOCRIS, Cat#4318) in a final volume 1 mL. The cells were centrifuged at 1000g for 90 min at 30°C. After centrifugation, the cells were resuspended in the supernatant and were incubated at 37°C for 18 h. At the end of the incubation, cells were washed in PBS and resuspended in 1mL of fresh growth media. The eGFP expression was analyzed 72 h later by flow cytometry.
41
2.10 Protein L Binding
Cells were isolated from in vitro cultures and washed twice in PBS supplemented with 4% BSA. Cells were stained with 0.04µg/mL of biotinylated protein L (Thermo Fisher Scientific, Cat# 29997) and incubated for 45 min at 4°C. Cells were then stained with 0.05 µg /mL of streptavidin conjugated with R-phycoerythrin (PE) (Biolegend, Cat#405203) for 30 min at 4°C. Cells were washed 3 times in FACS buffer and then fixed in 1% PFA. Flow cytometry was preformed on a FACS Caliber or LSR Fortessa and then analyzed on Flow Jo 9.2.
2.11 Cytotoxicity Assay
Target cells were incubated with 0.5 µM red CMTPX dye (Thermo Fisher Scientific, Cat# C34552) diluted in serum free media for 45 min at 37°C. A constant number of target cells were then incubated with effector cells at specific ratios for 4 h at 37°C. 1 mL of cold PBS was added to each co-culture and then centrifuged for 5 min at 300g and 4°C. Cells were resuspended in 300µl of annexin V binding buffer containing allophycocyanin conjugated annexin V (Thermo Fisher Scientific, Cat# A35110) and 50,000 counting beads (Thermo Fisher Scientific, Cat#C36950). Cells were incubated in the dark at room temperature for 15 min and then put on ice. Samples were run immediately on an LSR Fortessa and the data was analyzed on Flow Jo 9.2. Dead cells were excluded by FSC/SSC and being positive for annexin V staining. The percent cytolysis was determined by formula (100%-(Live cells in sample/Total amount of target cells in minimum cell death control)*100). The percentage of specific lysis was then determined by the formula (%cytolysis sample-%cytolysis target minimum control)/(%cytolysis target maximum control-
%cytolysis target minimum control)*100%. A two-tailed unpaired student’s t test was preformed comparing %cytolysis of different effector cells at the same ratio.
42
Chapter 3 Results 3 Results 3.1 CD138-positive hybridoma clones were identified by indirect ELISAs
A post-doctoral fellow in Dr. Medin’s lab purified soluble protein with a GST tag from BL21 cells. This protein was made up of 5 repeats of the distal region of the exogenous core protein of human CD138. This protein was used instead of full length CD138 in order to enhance the immunogenicity of this region. The protein was sent to Genscript to immunize mice for hyrbridoma generation. They identified positive clones by an indirect ELISA that screened the ability of antibodies in the supernatant of each clone to bind to the soluble GST-CD138 modified protein versus the GST tag alone (Figure 3.1). The 3E9B6 (A), 3G1D1 (B) and 8C12D1 (C) were identified as clones that produce mouse IgG2 mAbs specific for this GST-CD138 protein and not for the GST tag.
43
3" A)" 3E9B6* 2.5"
2" =GST6CD138"""" =GST"""" 1.5" Absorbance* 1"
0.5"
0" 1:10" 1:30" 1:90" 1:270" 1:810" 1:2430" Blank" Dilu/on*of*Supernatant*
3" B)" 3G1D1* 2.5"
2" =GST6CD138"""" =GST"""" 1.5" Absorbance* 1"
0.5"
0" 1:10" 1:30" 1:90" 1:270" 1:810" 1:2430" Blank" Dilu/on*of*Supernatant*
3" 8C12D1* C)" 2.5"
2" =GST6CD138"""" =GST"""" 1.5" Absorbance* 1"
0.5"
0" 1:10" 1:30" 1:90" 1:270" 1:810" 1:2430" Blank" Dilu/on*of*Supernatant*
Figure 3.1 Antibodies made by hybridoma cells are specific for GST-CD138 via ELISA Supernatants from cultures of the hybridomas (A) 3E9B6, (B) 3G1D1 and (C) 8C12D1 were collected. Diluted supernatants were run on ELISAs coated with 1µg/ml in 100µL/well of GST- CD138 or GST purified protein. Supernatants were diluted and added to the ELISA. Secondary goat anti-mouse IgG Fc antibody conjugated peroxidase was added to each well and then absorbance was determined.
44
3.2 CD138 Positive Hybridoma clones ability to bind to CD138 was confirmed by western blot
In order to confirm the results from the previous ELISA, Genscript also tested the ability of these antibodies to bind to GST-CD138 by western blot. Antibodies from the 3E9B6, 3G1D1 and 8C12D1 clones showed the ability to bind to the GST-CD138 protein and not to the GST tag by itself. This confirms the results from the ELISA that the 3 clones produce mouse IgG2 mAbs specific for the CD138 part of GST-CD138 soluble protein.
45
Figure 3.2 Antibodies made by hybridoma cells are specific for GST-CD138 via western blot 100ng of GST-CD138 and GST protein was loaded into an SDS-Page gel. The protein was transferred to a PVDF membrane. Supernatants from hybridoma clones 3E9B6, 3G1D1 and 8C12D1 were collected and used to stain the membranes. Secondary goat anti-mouse IgG Fc antibody conjugated peroxidase was used to detect presence of mAb from hybridoma supernatants.
46
3.3 Purified mAb binds to CD138 positive cell lines
The previous figures show that the 3 hybridomas produce antibodies with the ability to bind to the customized purified protein that was used to immunize the mice. I showed that these antibodies also bind to the full-length protein with more typical post-translation modifications by staining a panel of cell lines with the purified mAb from each clone. The mAbs from clones 3E9B6 (red), 3G1D1(orange) and 8C12D1 (green) and the commercially available MI15 clone (purple) showed no specific binding to the CD138- Jurkat cell line (A) compared to unstained (grey shaded) and isotype (blue) controls. A Jurkat CD138+ cell line was generated using a LV overexpression vector. The MI15, 3E9B6, 3G1D1 and 8C12D1 mAbs showed verifying degrees of specificity for the Jurkat CD138+ (B) cell line, and the CD138+ MM cell lines, RMPI 8226 (C), MM1.R (D), and U226 (E). Unlike the MI15 mAb, the 3E9B6, 3G1D1 and 8C12D1 mAbs showed binding to a CD138+ murine cell line, NIH 3T3 (F). The results show that the MI15 mAb only has specificity for human CD138, whereas the 3E9B6, 3G1D1 and 8C12D1 mAbs might have specificity for both human and murine CD138. This cross-reactivity would make them a superior mAb for testing in preclinical mouse models because of the added ability to monitor on target toxicities that might occur in murine cells that express CD138.
47
Figure 3.3 Specificity of purified mAb for CD138+ cell lines Jurkat (A), Jurkat LV CD138 (B), RPMI-8226 (C), MM1.R( D), U226 (E) and NIH 3T3 (F) cells were collected from in vitro cultures. Cells were isolated and stained for 30 min at 4°C with 0.5µg of purified mAb from the 3E9B6(red), 3G1D1(orange) 8C12D1(orange) MI15(purple) and B81-3 isotype control (blue) clones. Cells were run on a FACS Calibur and analyzed on FlowJo 9.2. Samples stained with mAb are displayed in their respective colours and compared to an unstained sample (grey shaded).
48
3.4 3E9B6 stimulates growth of CD138 positive cells
The utility of the 3E9B6 mAb was chosen to be further investigated because it showed a high binding titre to GST-CD138 and the broadest specificity for CD138+ cells. The anti-MM activity of the mAb was investigated. Figure 3.4 shows that 3E9B6 ligation to CD138 appears to stimulate proliferation of CD138+ cells. 3E9B6 and an isotype control purified in the Medin lab were added to cultures of RPMI 8226 (A), OCI AML-1 LV CD138 (B) and the OCI AML-1 (C) cells. CD138+ cells showed higher number of cells at different time points when they were cultured in the presence of 5µg/ml of 3E9B6. Binding of 3E9B6 to CD138 appears to be capable of enhancing growth and/or survival in cells with its natural and artificial expression.
49
Figure 3.4 Stimulation of CD138+ cells by 3E9B6 RPMI 8226 (A), OCI AML-1 LV CD138 (B), OCI AML-1 (C) were collected from in vitro cultures and washed with PBS. Cells were grown in normal growth media supplemented with PBS (blue), 5µg/ml of IgG2 nonspecific mAb (red) or 5µg/ml of 3E9B6 mAb (green). Cell counts were taken in triplicate every 48 hours.
50
3.5 3E9B6 stimulation affects intracellular signaling pathways
The molecular mechanism of 3E9B6 mediated proliferation and/or survival could help understand CD138’s role in MM oncogenesis and progression as well help predict any clinical use for the 3E9B6 mAb. RPMI 8226 cells were stimulated with 5µg/mL of 3E9B6 mAb (blue) or 5µg/mL of IgG2 nonspecific mAb (red) for 30 min at normal growth conditions. The Proteome Profiler Human Phospho-Kinase Array Kit revealed the potential activation or inhibition of various protein pathways. Figure 3.5 shows the notable results that include the increased phosphorylation of S15, S46 and S392 residues on p53 and the decreased phosphorylation of Src and ERK1/2 in cells grown with 3E9B6. Further investigation of the molecular mechanisms of 3E9B6 stimulation will reveal CD138’s role in MM growth and survival and 3E9B6’s potential as an antibody drug conjugate or adjuvant to boost the activity of healthy plasma cells.
51
Figure 3.5 Proteome Profiler Human Phospho-Kinase Array Kit RPMI 8226 cells were grown in the normal growth media supplemented with 5µg/ml of IgG2 nonspecific mAb(red) or 5µg/ml of 3E9B6 mAb blue for 30 min at normal growth conditions. Cell lysates were prepared and run on a Proteome Profiler Human Phospho-Kinase Array Kit. Proteins from the array that showed differences in phosphorylation levels are displayed.
52
3.6 Phosphorylation of p53 is upregulated by 3E9B6
The biggest difference in phosphorylation levels between cells grown with 3E9B6 and an isotype control was on p53, specifically at the S392 residue. The phosphorylation of wildtype p53 leads to its stabilization and subsequently to apoptosis and cell cycle arrest[232]. The phosphorylation of the S392 residue by casein kinase 2 (CK2) has been shown to enhance wildtype p53’s DNA binding ability[233, 234]. Many cancers including MM have been associated with p53 mutations. These mutations could result in a loss of the ability to regulate apoptosis and/or gain of oncogenic function that promotes an aggressive cell phenotype. These observations were made in RPMI 8226 cells that have an oncogenic gain of function p53 mutation. The phosphorylation of mutant p53 has been shown to interfere with other transcription factors and DNA repair proteins to prevent apoptosis and create genetic instability[235-237]. The phosphorylation of mutant p53 at S392 has been shown to have an anti-apoptotic effect and to regulate p53’s oncogenic function[238]. Cells were grown in the normal growth media supplemented with PBS, 5µg/mL of IgG2 nonspecific mAb or 5µg/mL of 3E9B6 mAb for 30 min at normal growth conditions. Figure 3.6 shows that 3E9B6 ligation leads to p53 phosphorylation at residue S392 within 30 min. The mechanism for p53 activation and the role of CK2 in this process remains unknown.
53
Figure 3.6 Stimulation of RPMI 8226 cells by 3E9B6 leads to phosphorylation of p53 RPMI 8226 cells were grown in the normal growth media supplemented with 5µg/ml of IgG2 nonspecific mAb (red) or 5µg/ml of 3E9B6 mAb blue for 30 min at normal growth conditions. Cell lysates were run on a 12% SDS gel, transferred to a PVDF membrane and stained for pS392 p53, p53 and actin.
54
3.7 Sequencing mAb heavy and light chains
The antibody heavy and light chain genes from the hybridomas were sequenced by a protocol involving the specific PCR amplification using universal degenerate primers, sub-cloning into a shuttle vector and Sanger sequencing. The universal primers were adapted from Wang et al[239]. The primers were optimized for more specific amplification, and less disruptive sub-cloning into the pBluescript shuttle vector, for a more wide-ranging method. The amino acid sequences were confirmed by mass spectrometry in Dr. Richard Drake’s lab at the Medical University of South Carolina and aligned with the DNA sequences that we determined. The amino acid sequences are shown in figure 3.7. The CDR regions were predicted in silico by IGBLAST and are shown in red. 3E9B6 was shown to be 97% similar to 8C12D1 with only one different amino acid in the predicted CDR. It is likely that these clones share a similar ancestry. Whereas, 3E9B6 shares only 63% amino acid homology with 3G1D1 clone indicating that they are from entirely distinct clones.
55
mAb$ Heavy$Chain$ Light$Chain$ 3E9B6$ Q$V$Q$L$E$E$S$G$P$S$L$V$K$P$S$Q$T$L$S$L$T$C$S$V$$T$G"D"S"I"T"S" D$I$V$L$T$Q$T$P$L$S$L$P$V$S$L$G$D$Q$A$S$I$S$C$R$S$S$Q"S"L"V"H"S" G"Y"W$N$W$I$R$K$F$P$G$N$K$L$E$Y$M$G$Y$I"R"Y"S"G"S"T$Y$Y$N$P$ N"G"N"T"Y$L$H$W$Y$L$Q$K$P$G$Q$S$P$K$L$L$I$Y$K"V"S"N"R"F"S$G$ S$L$K$S$R$I$S$I$T$R$D$T$S$K$N$Q$Y$Y$L$Q$L$N$S$V$T$T$E$D$T$A$T$Y$ V$P$D$R$F$S$G$S$G$S$GT$D$F$T$L$K$I$S$R$V$E$A$E$D$L$G$V$Y$FC$S$ Y$C$A$R$W"L"P"H"A"M"D"Y"W$G$Q$G$T$S$V$T$V$S$S$$ Q$S"TH"V"P"P"T"F$G$G$G$T$K$L$E$I$K$R$A$$$$$ $ $ 3G1D1$ Q$V$K$L$E$E$S$G$P$G$L$V$Q$P$S$Q$S$L$S$I$T$C$T$V$S$G"FS"L"T"S"Y" D$I$V$L$T$Q$S$P$L$T$L$S$V$T$I$G$Q$P$A$S$I$S$C$K$S$S$Q"SL"L"D"S" G"V$H$W$V$R$Q$S$P$G$K$G$L$E$W$L$G$V"I"W"S"G"G"S"T"D$Y$N$A$ D"G"K"T"Y"L$N$W$L$L$Q$R$P$G$Q$S$P$K$R$L"I"Y"L"V"S$K$L$D$S$G$ $ A$F$I$S$R$L$S$I$S$K$D$N$S$E$S$Q$V$F$F$K$M$N$S$L$Q$A$N$D$T$A$I$ V$P$D$R$F$T$G$S$G$S$G$T$D$F$T$L$K$I$S$RV$E$A$E$D$L$G$V$Y$Y$C$ Y$Y$C$A$R$N"YG"T"W$G$Q$G$T$L$VT$V$S$A$$$$$$$ W$Q"G"T"H"F"P"L"T"F$G$A$G$T$K$L$E$L$K$R$A$$$$$ $ $
8C12D1$ V$D$E$V$K$L$E$E$S$G$P$S$L$V$K$P$S$Q$T$L$S$L$T$C$S$VT$G"D"S"I"T" D$I$V$L$T$Q$S$T$L$S$L$P$V$S$L$G$D$Q$A$S$I$S$C$R$S$S$Q"S"L"V"Y"S" S"G"Y"W$N$W$I$R$K$F$P$G$N$K$L$EY$M$G$Y$I"S"Y"S"G"S"T$Y$Y$N$ N"G"N"T"Y$L$H$W$Y$L$Q$K$P$G$Q$S$P$K$L$L$I$Y"K"V"S"N"R"F"S$G$ P$S$L$K$S$R$I$S$I$T$R$D$T$S$K$N$Q$Y$Y$L$Q$L$N$S$V$T$T$E$D$T$A$T$ V$P$D$R$F$S$G$S$G$S$G$T$D$F$T$L$K$I$S$R$V$E$A$E$D$L$G$V$Y$F$C$ Y$Y$C$A$R$W"L"P"H"A"M"D"Y"W$G$Q$G$T$S$V$T$V$S$S$$ S$Q$S"T"H"V"P"P"T"F"G$G$G$T$K$L$E$I$K$R$A$ $ $
Figure 3.6 Amino acid sequences of the heavy and light chains of the mAb The genes for the mAb heavy and light chains were sequenced by a protocol involving the specific PCR amplification using universal degenerate primers, sub-cloning into a shuttle vector and Sanger sequencing. The CDR regions were predicted in silico by IGBLAST and are shown in red.
56
3.8 The design of the 3E9B6 Chimeric Antigen Receptor The main goal of this project was to design and test a novel CAR that is specific for CD138. A 2nd generation CAR was designed using the scFv from the 3E9B6 mAb as the antigen recognition domain. 3E9B6 was chosen because of its apparent superior avidity and specificity towards CD138. An IRES eGFP was added into this transgene to provide a mechanism to detect transduced cells. The expression of eGFP is able to act as a transduction marker but cannot be used to infer the degree of CAR expression. The two separate proteins are coded for on the same transgene and but translated independently. Their insertion and transcription are tied together but their expression and stability are still unrelated. Direct detection is necessary for accurate analysis of protein expression. In the past this has proven to be difficult. CARs have been detected using mAbs that bind to antigen binding fragments of the scFv[240]. However, these mAbs do not consistently work for every CAR and some trial and error is necessary. This difficulty led to the development of a mAb specific for one of the CD19 CARs to detect it directly[241]. This strategy is effective but costly, and inefficient. We have decided to use protein L, a light chain specific immunoglobulin like protein from Peptostreptococcus magnus, to directly detect CAR expression[242, 243]. Protein L binds to most mammalian antibody light chains. However, we predicted it would not bind to the light chain of 3E9B6 mainly because the 12th residue in the FR1 is proline[244]. The full epitope of protein L, DVQMTQSPASLSVSVGETVTITC, was grafted into the FR1 of the light chain to allow for protein L detection. Grafting this sequence has been shown to have no effect on antigen binding[244]. Figure 3.8 shows the design of the 3E9B6 HL CAR. The CD8 leader sequence (LS) was added upstream to ensure expression and proper cellular membrane localization. A 3E9B6 scFv was designed by connecting the heavy chain to the modified light chain via a
(Gly4Ser)3 linker. CD8 hinge and transmembrane domains and the signaling domains of the CD137 and CD247 were added downstream. The 3E9B6 HL CAR was sub-cloned into a pDY lentiviral vector using EcoR1 and BamH1 restriction enzymes. A human elongation factor-1 α (EF1α) promoter was used to provide high 3E9B6 HL CAR expression. This construct was transfected into 293T cells with LV packaging plasmids to generate high titre LV particles for gene transfer of the 3E9B6 HL CAR into effector cells.
3E9B6 HL CAR design 57
CD8 Lin- CD8 Hinge and Heavy Chain Light Chain CD137 CD247 LS ker Transmembrane
cPPT 5’ 3E9B6 HL 3’ LTR EF1α IRES eGFP WPRE SIN/LTR CAR
Figure 3.7 3E9B6 HL CAR IRES eGFP construct
The CAR sequence was designed to have a CD8 leader sequence (LS) (amino acid 1-23), scFv grafted with the protein L binding sequence, DVQMTQSPASLSVSVGETVTITC, in the FR1 region, CD8 hinge domain (amino acid 117-183), CD8 transmembrane domain (amino acid 184- 203), CD137 (amino acid 214-255) signaling domain, and CD247 (amino acid 52-164) signaling domain. This sequence was synthesized by Genscript and then subcloned into a pDY vector already containing an IRES eGFP. The transgene is flanked by a 5’ long terminal repeat (LTR), and a central polypurine tract (cPPT) element, and by a 3’ self-inactivating (SIN) LTR, and a woodchuck hepatitis virus posttranscriptional regulatory element (WPRE).
58
3.9 The Generation of a Stable NK-92 Cell Line expressing the 3E9B6 CAR
The NK-92 cell line was chosen as the immune effector cell line to test the functionality of the 3E9B6 HL CAR. This allowed for the generation of a stable cytotoxic cell line that expresses the CAR removing the need repeatedly acquire and transduce primary cells for testing. The 3E9B6 HL CAR IRES eGFP was genetically engineered into the cytotoxic NK-92 cell line via high titre LV particles. Standard transduction protocols using a LV MOI of 100 had very poor transduction efficiency. An optimized transduction protocol that included BX-795, a TBK1/IKKε complex inhibitor, and a LV MOI of 25 resulted in a transduction efficiency of 35% (figure 3. 9 dashed blue line). The eGFP+ cells were sorted for via FACS, resulting in the stable expression of eGFP in greater than 99% of cells (figure 3. 9 green line). The expression of the CAR and its functionality can now be assessed in this stable cell line.
59
NK#92&3E9B6&HL&IRES&eGFP& NK#92&NT& NK#92&3E&HL&IRES&eGFP& unsorted& sorted& Percentage&Of&Cells&
eGFP&
Figure 3.10 Generation of a NK-92 3E9B6 HL IRES eGFP cells NK-92 cells were transduced with 3E9B6 HL IRES eGFP LV in the presence of protamine sulfate and BX-795. The expression of eGFP in the non-transduced (grey shaded), transduced unsorted (dashed blue) and transduced sorted (green) are compared.
60
3.10 Protein L Direct Detection of CAR
We have generated a 3E9B6 HL CAR IRES eGFP NK-92 cell line. The stable expression of eGFP throughout this population indicates that all of the NK-92 cells have had the 3E9B6 HL CAR IRES eGFP transgene inserted into their genome. The expression of 3E9B6 HL CAR on the cell surface was detected directly through FACS. As mentioned before we engineered the Protein L epitope into the 3E9B6 HL CAR. CAR expression was detected in the sorted NK-92 3E9B6 HL CAR IRES eGFP cell line by using a protocol with biotinylated Protein L and fluorescent streptavidin. Figure 3.10 shows that Protein L specifically binds to NK-92 3E9B6 HL CAR IRES eGFP cells compared to unmodified NK-92 cells. Therefore, the 3E9B6 HL CAR is stably expressed along with eGFP. This also indicates that is possible to graft this detection sequence into a CAR construct.
61
NK,92) NK,92)3EB96)HL)IRES)eGFP) Percentage)Of)Cells)
Phycoerythrin)(PE)))
Unstained) Protein)L+)) PE,)Streptavidin) PE,)Streptavidin)
Figure 3.10 Flow Cytometry analysis of protein L staining of NK-92 3E9B6 HL CAR cells NK-92 3E9B6(A) and unmodified NK-92 (B) cells were collected from in vitro cultures and 0.04 µg of protein L for 45 min at 4°C. in the dark. Cells were then incubate with 0.05 µg /mL of PE-streptavidin. Cell samples were run on an LSR Fortessa and analyzed on Flow Jo 9.2. Cells stained with protein L and PE-Streptavidin (green) were compared cells stained with only PE- Streptavidin (red) and unstained cells (grey shaded).
62
3.11 3E9B6 HL CAR enhances NK-92 cytotoxicity for CD138 positive Cells
The cytotoxicity of NK-92 3E9B6 HL CAR IRES eGFP cell line was compared to the cytotoxicity of the non-transduced NK-92 cell line by an adapted version of a flow based cellular cytotoxicity assay developed by Cao et al.[245]. It was adapted to use red CMPTX instead of CFSE as a target cell marker to allow testing of effector cells that are eGFP+. It was also adapted to use Annexin V, instead of 7-aminoactinmycin, because Annexin V has been shown to be more sensitive in detecting cell death[231]. Figure 3.11 shows the cytotoxicity of the two cell lines against the RPMI 8226 (A), MM1.R (B) U226 (C) and OCI-AML-1 (D). The NK-92 3E9B6 HL CAR IRES eGFP cell line showed significantly greater cytotoxicity than the NK-92 cell line against these CD138+ MM cell lines, RPMI 8226, MM1.R and U226 at different ratios of effector to target (E:T) cells. The cytotoxicity of NK-92 3E9B6 CAR IRES eGFP cells was not significantly different than the cytotoxicity of non-transduced NK-92 cells against this CD138- cell line, OCI AML-1. These results show that NK-92 3E9B6 HL CAR cells have an enhanced cytotoxicity that is specific for CD138+ cells. Therefore, we can conclude that the antigen detection domain is functional. It also indicates that grafting the protein L binding sequence did not eliminate the binding ability of the scFv and is a viable method to provide a mechanism for direct detection. The high cytolysis of target cells at low E:T cell ratios demonstrates the high in vitro potency of the 3E9B6 HL CAR NK-92 cells.
63
(A) RPMI 8226 (B) MM1.R 100 100 * * 80 * * 80 * 60 60
40 40 * Specific Lysis Specific Lysis 20 20
0 0 1 0.5 0.25 1 0.5 0.25 Effector Cells: Target Cells Effector Cells: Target Cells
(C) U226 (D) OCI AML-1 (CD138-) 100 100 * 80 * 80 60 * 60
40 40 Specific Lysis Specific Lysis 20 20
0 0 1 0.5 0.25 1 0.5 0.25 Effector Cells: Target Cells Effector Cells: Target Cells =NK-92 3E9B6 HL CAR =NK-92
Figure 3.11 In Vitro Cytotoxicity of NK-92 3E9B6 HL CAR and NK-92 Cells- Different number of NK-92 3E9B6 CAR HL IRES eGFP CAR (blue) and NK-92 NT(red)were co-cultured with a constant number of RPMI 8226(A), MM1.R(B), U226(C) and OCI AML-1(D) that were previously stained with 0.5 µM red CMPTX dye. Samples were run on the LSR Fortessa until 10,000 beads were collected. Dead cells were excluded by FSC/SSC and being positive for Annexin V staining.The percent cytolysis was determined by amount the formula (100%-(Live cells in sample/Total amount of target cells in minimum cell death control)*100). The percentage of specific lysis was then determined by the formula (%cytolysis sample-%cytolysis target minimum control)/(%cytolysis target maximum control-%cytolysis target minimum control)*100%. A two-tailed unpaired student’s t test was preformed comparing %cytolysis of different effector cells at the same ratio.
64
3.12 3E9B6 HL CAR Initiates Downstream ZAP70 signaling
In order to ensure that the signaling domains are functional, the phosphorylation of the protein directly downstream of CD3ζ, zeta-chain associated protein 70 (ZAP70) was analyzed. NK-92 3E9B6 CAR HL IRES eGFP and NK-92 cells were co-cultured at a 1:1 ratio for 4 h with Jurkat, Jurkat+CD138 an RPMI 8226 cells. In NK-92 3E9B6 HL CAR cells, phosphorylation of ZAP70 was only seen when co-cultured with the CD138+ cells. Furthermore, ZAP70 phosphorylation was not detected in any of the non-transduced NK-92 cell co-cultures. This indicates that ZAP70 signaling and the enhanced cytotoxicity is CAR-antigen binding dependent. Due to the inability to separate effector cells from target cells before cell lysates were prepared, it is possible that ZAP70 signaling was detected in the target cells and not the effector cells. However, this is unlikely because of the lack of ZAP70 signaling in the target cells when co-cultured with unmodified NK-92 cells. It is likely that if the ZAP70 pathway was activated in the target cells, it would be activated when co-cultured with both NK-92 3E9B6 HL CAR IRES eGFP and unmodified NK-92 cells. Furthermore, RPMI 8226 cells are ZAP70- and lysates prepared from co-cultures of NK-92 3E9B6 CAR IRES eGFP with RMPI 8226 cells showed of ZAP70 activation. We can conclude that the 3E9B6 HL CAR activates ZAP70 and that this is a unique activation pathway from the innate cell killing mechanisms of NK-92 cells because the cytotoxicity of unmodified NK-92 cells was independent of ZAP70 activation. Synergy between the unique pathways could be responsible for the high potency at low E:T ratios.
65
Figure 3.12. Western Blot of ZAP70 Phosphorylation In NK-92 3E9B6 HL CAR Cells NK-92 3E9B6 HL CAR cells and unmodified NK-92 cells were incubated for 4 hours by themselves, or at a 1:1 ratio with Jurkat, Jurkat+LV CD138 or RPMI 8226. Cells were lysed using a RIPA buffer with protease and phosphatase inhibitor cocktails. Lysates were normalized to the number of NK-92 3E cells and run on a 12% SDS gel. The gel was transferred to a PVDF membrane and then stained for phosphorylated ZAP70, ZAP70 and actin.
66
Chapter 4 Discussion 4 Discussion 4.1 The 3E9B6 HL CAR
The overall objective of this project was to design and engineer a functionally active CD138 specific CAR. We accomplished this by designing a CAR with a scFv that we identified from the generation and screening of novel hybridomas. Although several different hybridomas were identified, a scFv was designed from the 3E9B6 clone because it appeared to have the greatest avidity for the customized CD138 purified protein (figure 3.1) and full-length CD138 protein across a broad range of cells (figure 3.3). A 2nd generation CAR with CD137 and CD3ζ signaling domains was designed and tested. The 3E9B6 HL CAR was introduced into NK-92 cells. A stable cell line, NK-92 3E9B6 HL CAR IRES eGFP, was generated which showed enhanced cellular cytotoxicity compared to the unmodified NK-92 cell line against three CD138+ MM cell lines but not towards a CD138- cell line (Figure 3.11). This data shows that the 3E9B6 HL CAR enhanced the cytotoxicity of NK-92 cells specifically against CD138+ cells. Data from figure 3.12 indicates that 3E9B6 HL CAR is able to initiate downstream signaling in effector cells after antigen binding. We have thus accomplished the primary objective of this project and have shown that a CD138 CAR could mediate functional cytotoxic activity against CD138+ myeloma cells.
Multiple clones from our screening were determined to be specific for CD138. Further investigation into their cross-reactivity with other proteins is warranted. However, it is unlikely that they bind to other syndecan family proteins because only 10-20% of their ectodomain is shared with CD138’s[246] Furthermore, all of the mAbs showed no specificity for Jurkat cells that express syndecan-2 and 4. Other assays that could have been used to select the optimal clone include characterizing the cellular effect of scFv ligation, quantifying the binding affinity, pinpointing their specific epitopes, identifying any promiscuous activity, and detecting the difference in their ability to mediate CAR cytotoxicity towards cells with different expression levels of CD138. It would be useful to quantify the mAbs’ binding affinity for CD138 to help
67 understand their therapeutic window in different platforms. Enhancing the affinity and specificity of these antibodies through one of the established methods of affinity maturation is also worth exploration. Although the investigation of each clone would prove interesting, this project focused on understanding the utility of the 3E9B6 mAb.
4.2 3E9B6 HL CAR NK Cells
A unique feature of this research is the use of an NK cell line as the recipient of the CD138 specific CAR. NK cells were chosen for a number of reasons. From a practical perspective the NK-92 cell line was ideal for cell culture and generating stable expression of adoptive proteins. But equally or even more importantly, allogeneic NK cells and NK cell lines have shown the ability to efficiently and spontaneously kill cancer cells through multiple mechanisms. More to this point, endogenous NK cells have been shown to be important in controlling MM in the early stages but show increased dysfunction as the disease progresses [247]. For these reasons, NK cells might be superior to T cells for CAR therapy of MM. Figure 3.11, shows that 3E9B6 HL CAR NK-92 cells showed high potency against MM cell lines even at low E:T ratios. It would be interesting to compare this against 3E9B6 HL CAR T cells. Figures 3.11 and 3.12 show that non-transduced NK-92 cells showed the ability to kill 40% of RPMI 8226 cells at a 1:1 E:T ratio without the activation of ZAP70. This suggests that the high potency of 3E9B6 HL CAR NK-92 cells could be partially related to the CAR mediated and endogenous mechanisms for detection and activation working together. This could be an advantage over CAR T cells, where for the most part, CAR T cell therapy has relied on CAR specificity and signaling alone for T cell activation. There are examples of T cell therapies that utilize both CAR and endogenous TCR mechanisms for anti-cancer activity. Virus specific TCRs have been used as a mechanism to amplify CAR T cells in vivo and to provide an additional mechanism for detecting viral associated cancers[248, 249]. This strategy increases the specificity of T cells but the potency might be limited because both mechanisms converge on the CD3ζ pathway. CAR NK cells need to be further explored to understand their advantages and disadvantages. The best effector cell type for adoptive cell therapy of MM will be determined by the ability to efficiently kill cancer cells, enter the tumour microenvironment, overcome immunosuppression, persist in the host, and stimulate native immune cells. Even if CAR NK cellular therapies have superior killing ability,
68
CAR T cells might still be more effective because of their longer in vivo persistence. The greater clinical feasibility and cheaper cost of NK-92 therapy also needs to be considered. The 3E9B6 HL CAR can now be used in future studies as a tool to study the advantages of CAR therapy in primary T and NK cells, as well as in the NK-92 cell line to treat CD138+ malignancies.
4.3 In Vivo Models of Multiple Myeloma to test 3E9B6 HL CAR
Now that this CAR has been shown to be functional, it needs to be shown that CD138 CAR therapy is an effective way to treat MM in mouse models. There are two main types of MM mouse models that can be used to do this. One option is genetically engineered syngeneic mice. The Vκ*MYC mouse was shown to mimic the complete progression of MM[250]. This model was shown to have more realistic tumour microenvironments in the bone marrow, which would better recreate the obstacles that adoptive cell therapies might encounter. Furthermore, positive and negative interactions of adoptive cells with other immune cells could be evaluated in these immuno-competent mice. This model relies on a lifetime of DNA damage to induce the disease and, thus, a long observation period is required. On one hand, this would make testing therapies more time consuming. On the other hand, elderly mice might be more representative of the elderly demographic affected by this disease. Other disadvantages include the high variation in tumour growth and phenotype between mice and the need to use effector cells of murine origin. The interactions of murine effector cells with the tumour and other murine immune cells might not be consistent with how human ones would act. The cross-species reactivity of the 3E9B6 HL CAR with human and murine CD138 makes using this model possible. It also makes monitoring the on target toxicities from CAR therapy possible in any mouse model.
Using xenogeneic models that graft MM cell lines or patient derived samples into non-obese diabetic SCID gamma (NSG) mice is another possibility. Xenogeneic models have the innate problem of requiring immuno-compromised animals, making the complex interactions between the adoptive cell therapy and the host’s immune system impossible to recapitulate and study. Despite this major flaw, xenogeneic models are attractive because human effector cells can be directly tested against human cell lines or patient derived samples. It is also possible to perform large screening approaches in a reasonable amount of time. In the case of MM, xenogeneic
69 models have been improved by implanting fetal human or rabbit bone chips into SCID mice. These mice provide a more hospitable environment and a higher level of consistency for primary myeloma cell engraftment[251]. Furthermore, SCID mice implanted with human bone chips that were inoculated with bone marrow cells from patients with MM developed more typical manifestations of the disease such as plasmacytosis, high levels of M proteins, and severe bone lesions[251]. These models can be used to answer different questions about 3E9B6 HL CAR therapy.
4.4 CD138 as a Target For CAR Therapy
It still needs to be demonstrated if CD138 is a good target for MM therapies. The high expression of CD138 on MM cells and limited expression in healthy tissue is favourable. However, there is some debate about the identity of a MM initiating cell. Myeloma cells possess somatically hypermutated immunoglobulin gene sequences without intra-clonal variations, which suggests the existence of MM initiating cells from a post-germinal center B cell or a more differentiated cell[252]. There is conflicting data about the expression of CD138 on these initiating cells probably due to the instability of CD138 during ex vivo cell culture[253]. One study showed that initiating cells were CD19+ CD27+ CD138- cells with a memory B-cell phenotype[254]. Another study showed that both CD138+ and CD138- fractions of patient samples were able to engraft and recapitulate the disease in SCID mice with implanted rabbit bone chips[255]. Likewise, another group showed that the fraction with the highest ability to serially engraft into NSG mice was CD38+ CD138+ CD19-[256]. These varied results are either due to the inconsistencies in methodologies of these studies or because there exists a wide variety of MM initiating cells across patients. Being able to identify the genetic hierarchy of MM clones in patients could serve as a valuable biomarker for targeted therapies.
There are other CD138 specific CARs being developed. One group tested a novel CD138 CAR with a scFv from the 4B3 mAb in NK-92 cells[257, 258]. It is appears that the 3E9B6 HL CAR displays greater in vitro cytotoxicity, although the two CARs would have to be compared directly against each other in order to make this conclusion. CD138 CAR T cells are being tested
70 in a phase I/II trial [218]. So far the anti-tumour activity of these CAR T cells has been limited with the best clinical responses giving patients SD for 3-7 months[219]. Encouragingly no severe toxicities were associated with this treatment[219]. Further studies to improve the efficacy of CD138 specific CAR T cells are warranted. Combining drugs that enhance T cell activity, such as immune checkpoint inhibitors with CAR therapies is one way to improve their efficacy. Another interesting partner for CAR therapies are IMiDs, especially in the context of MM. The IMiD, lenalidomide has become an important part of standard and maintenance therapy for patients with MM. Lenalidomide has been used as a maintenance therapy after CD19 CAR or NY ESO-1 TCR specific T cells to treat MM[123, 155]. This combination was able to provide durable responses to some patients. Using these two therapies simultaneously could be even more effective. Lenalidomide has been shown to directly enhance the activity of CD19 CAR T cells preclinically in a B-NHL mouse model[259]. Given the proven efficacy of lenalidomide to treat MM and the evidence that it can directly boost CAR T cell activity, it could enhance the efficacy of CD138 CAR therapy. Additionally, there exists room for different CARs to the same target like in the case of CD19. So far determining the best epitope to target an antigen via CAR therapy needs to be determined empirically on a case-by-case basis and having multiple CARs could help to do so. On one hand, having epitopes more proximal to the membrane has been shown to increase the potency by bringing T cells closer to the target cell. Targeting proximal epitopes has also been shown to limit CAR-ligand clusters, which in turn prevents large phosphatase molecules such as CD45 from entering the synapse and inhibiting CD3ζ signaling[260]. On the other hand, the epitope is more accessible at distal locations on the protein, which is thought to be more important in proteins with complex interactions, such as CD138. Ideally, the 3E9B6 HL CAR would be compared to the other CD138 CARs to determine the most effective one. CD138 CARs could even work together to provide multiple cycles of therapy to avoid the anaphylaxis, immunogenicity and relapse that might be associated with therapy of a single CAR. In conclusion, 3E9B6 HL CAR has been shown to be functional and can now be used to answer questions about CD138 CAR efficacy in treating MM and other CD138+ cancers.
71
4.5 3E9B6 mAb enhanced MM cell growth
Monoclonals can have different cellular effects based on the nature of the interaction with their binding protein. It was shown in figure 3.4 that the 3E9B6 mAb enhanced the growth of RPMI 8226 and OCI AML-1 LV CD138 cells. Interestingly, another murine CD138 specific mAb, 4B3, was shown to inhibit the growth of MM cell lines, XG-1 and XG-2 [258]. This is not entirely surprising because the epitope, class and subclass of the mAb all play a role in determining how it will arouse, obstruct or alter the function of the protein. Furthermore, CD138 has been shown to have various functions that control proliferation, all of which are not completely understood. 3E9B6 could affect any one of these functions in order to stimulate growth or enhance survival. It has been shown that some anti-CD138 mAbs can induce endocytosis and that this is dependent on their epitope[261]. It is possible 3E9B6 induces endocytosis of CD138 along with its macromolecular cargo. This cargo could include intracellular ligands that stimulate growth and survival. It is unlikely that this is the case because CD138 mediates lipid raft dependent endocytosis, which requires ERK and subsequent Src signaling[262]. The results from a Proteome Profiler Human Phospho-Kinase Array Kit seen in Figure 3.5 show that phosphorylation of Src and ERK are downregulated in cells grown with 3E9B6. It is possible that this downregulation of Src and ERK is because 3E9B6 prevents the clustering of CD138 around multivalent ligands, which is necessary to form lipids rafts for endocytosis. The potential 3E9B6 hindrance of lipid raft formation and subsequent endocytosis is illustrated in figure 4.1A. Lipid rafts can also play a role in survival by mediating apoptosis through the recruitment of death receptors[263]. It is important to note that in my hands, RPMI 8226 cells grew consistently at 80% cell viability. It is possible that the increased number of cells at each time point was because of the increased survival through this 3E9B6 mediated impediment to apoptosis. In Figure 3.5, one of the master regulators of apoptosis, p53 was shown to have increased phosphorylation at S15, S46 and S392 in response to 3E9B6 binding. The phosphorylation of the S392 residue was confirmed by western blot in figure 3.6. It is possible that a 3E9B6-mediated obstruction to apoptosis leads to enhanced p53 activation to try an overcome this impediment. Since RMPI 8226 cells have an oncogenic mutation in their p53 gene, the activation of p53 would have an anti-apoptotic and proliferative effect instead. Figure 4.1B depicts how it is possible that by creating a barrier to apoptosis, 3E9B6 could activate mutant p53 and its growth and survival functions. Future work needs to be done to characterize
72 how 3E9B6 directly affects lipid raft formation, endocytosis and p53 phosphorylation and function. Although multiple kinases have been shown to phosphorylate S15, S46 and S392, inhibiting the most common ones, checkpoint kinase-2 (CHK-2), Homeodomain-interacting kinase 1 (HIPK1) and CK2, during 3E9B6 mediated growth will help uncover if the proliferation and survival benefits are p53 dependent. Further understanding the mechanism for 3E9B6 induced proliferation and survival would help uncover the complex role of CD138 in MM progression and ascertain some of the potential applications for this mAb.
73
A)
SrcK ERK ERK SrcK
B)
Apoptosis
p53 p53 p53 p53
Apoptosis
=Lipid Ra) =Endosome =Death Receptor =Death Effector =Procaspase 8 =CD138 =3E9B6 =MulBvalent Tetramer Domain Ligands
Figure 4.1. Shows how 3E9B6 could affect (A) endocytosis and (B) apoptosis by preventing CD138 clustering around a multi-valiant ligand and subsequent lipid raft formation.
74
4.6 Other Potential Therapeutic uses of 3E9B6
Even though 3E9B6 did not directly inhibit the in vitro growth of MM cells it could be used to modulate the immune system to help fight cancer. One strategy to provide utility to this mAb is to switch the subclass of 3E9B6 from IgG2 to IgG1 in order to give it the ability to trigger ADCC, CDC and ADCP upon CD138+ cells. This subclass switching might also remove the proliferative effect of this mAb as the IgG2 hinge has been shown to impart a superagonistic ability onto immunostimulatory mAbs[264]. Another strategy would be to embrace the immunostimulatory qualities of this mAb and use it to boost the activity of healthy plasma cells to help treat other cancers and diseases. The role of B cell lineages in cancer remains controversial. As mentioned earlier, B cells have been implicated in providing immune privilege to cancer cells by polarizing the Th response. However, in some solid cancers the presence of PCs and B cells along with T cells in tumours has been associated with higher survival rates, especially if they form tertiary lymphoid structures[265-267]. Tumour infiltrating plasma cells can supplement T and NK cell activity by shielding them from inhibitory cells, or producing tumour specific antibodies to direct CDC, ADCC, and ADCP and to facilitate antigen presentation to T cells via opsonization[268]. Strategies to recruit PCs to support tertiary lymphoid structure formation to boost anti-tumour immune responses are being tested, such as an oncolytic virus engineered with CXCL-13. It is possible that 3E9B6 could also enhance vaccines by augmenting the formation of tertiary lymphoid structures and function by stimulating the growth of healthy PCs. 3E9B6 could also be used in this fashion to mitigate some of the adverse effects of other cancer therapies. Rituximab has been shown to be effective in treating CD20+ malignancies but it leaves patients with hypogammaglobulinaemia[269]. Hypothetically, 3E9B6 could be used to help boost the amount of healthy PCs to try and reverse this side effect. The ability of 3E9B6 to stimulate growth of healthy PCs, as well as understanding how it affects PC function, specifically antibody production needs to be further understood before it can be tested for these therapeutic uses.
There is a lot of optimism around CD138 for an antibody drug conjugate target in MM because of its broad expression and function. It has been shown to mediate endocytosis, which can be
75 initiated by mAb binding[261]. This function could make a CD138 directed antibody drug conjugate effective in delivering cytotoxic drugs to the interior of MM cells. 3E9B6 is specific for CD138+ cells and may provide a good vehicle to target MM. Quantifying the avidity of this mAb for CD138 would be useful in estimating its maximum tolerable dose and therapeutic benefit as an antibody drug conjugate. It is also important to understand the consequences of the mAb-antigen interaction. The consequences of the 3E9B6-CD138 interactions were discussed above. The inhibition of Src and ERK activity suggest that 3E9B6 is inhibiting CD138 internalization, at least initially. The internalization of CD138-3E9B6 complexes needs to be further understood and quantified before the most effective linker and cytotoxic drug can be chosen for it. If 3E9B6 is internalized quickly, an antibody drug conjugate can be designed with a stable linker to efficiently deliver a highly cytotoxic drug to the interior of the cell. If the internalization rate is relatively slow, an antibody drug conjugate can be designed with an unstable linker to release a less toxic drug in the tumour microenvironment. This strategy would effectively deliver a toxic payload to the tumour microenvironment instead of directly to the interior of cancer cells. Although it has less specificity, this has the added bystander effect of killing all the cells in the tumour microenvironment, including CD138- malignant cells, Treg cells and MDSCs. The characteristics of 3E9B6 need to be better understood in order to use it as an antibody drug conjugate.
4.7 Conclusions
The main goal of this project was to generate novel mAbs to make a CD138 specific CAR. Hybridoma cells that produce CD138 specific antibodies were made by immunizing mice with a customized protein made of repeats of the distal portion of the exogenous protein to preferentially generate mAbs recognizing this region of the protein. The 3E9B6 mAb was chosen because it appeared to have the greatest avidity for the purified and full length CD138 protein expressed across a broad range of cells. The 3E9B6 mAb mediated proliferation of MM cells which gives insight into CD138’s role in tumour growth and progression. Further study is needed to understand the effects and potential applications of the 3E9B6 mAb. Finally, the main goal of this project was accomplished when a novel 2nd generation CAR named 3E9B6 HL CAR, was designed and shown to enhance the lytic ability of the NK-92 cell line against CD138+ cells
76 through the activation of the CD3ζ pathway. Now that this CAR has been shown to functional, additional research could focus on its enhancement, and the evaluation of its ability to direct different effector cell populations to treat MM and other CD138+ diseases. It is also very important characterize the safety and toxicity of 3E9B6 HL CAR therapy by understanding the potency and the cellular effects of CAR activation on the immune effector cells, monitoring the on target, off tumour toxicity and understanding any promiscuous binding the of the 3E9B6 HL scFv in a murine MM model. The 3E9B6 HL CAR can be used as a tool to find effective partners for a CD138 specific CAR in the context of MM that could enhance the safety and efficacy of CAR therapy. CAR T cell therapies have usually been paired with chemotherapeutic drugs, cyclophosphamide, pentostatin, bendamustine, and fludarabine. Unexpectedly three patients in the ROCKET trial died from cerebral anemia because of the combination of CD19 CAR T cells with a fludarabine preconditioning regime[270]. This emphasizes the fact that modulating the immune system with CAR therapy can have great potency and very serious consequences, which can both be heightened by the drugs and other immunotherapies that are paired with it. Finding partners for CD138 CAR therapy that boost immune activity could help increase its efficacy. Given the proven efficacy of lenalidomide to treat MM and the evidence that it can directly boost CAR T cell activity, exploring its use with 3E9B6 HL CAR therapy is very intriguing. In conclusion, the 3E9B6 HL CAR can enhance NK-92 cells’ ability to specific lyse CD138+ cells but its ability to safely and effectively treat MM still needs to be assessed. Furthermore, the efficacy and safety of the 3E9B6 HL CAR may be enriched by optimizing the binding of the scFv, choosing the optimal immune effector cell population and finding effective combination therapies.
.
References
1. Canadian Cancer Society. and National Cancer Institute of Canada. Advisory Committee on Records and Registries., Canadian cancer statistics 2015. 2015, Canadian Cancer Society: Toronto. p. v.
2. Hanahan, D. and R.A. Weinberg, The hallmarks of cancer. Cell, 2000. 100(1): p. 57-70.
3. Hanahan, D. and R.A. Weinberg, Hallmarks of cancer: the next generation. Cell, 2011. 144(5): p. 646-74.
4. Coley, W.B., The treatment of malignant tumors by repeated inoculations of erysipelas. With a report of ten original cases. 1893. Clin Orthop Relat Res, 1991(262): p. 3-11.
5. Burnet, M., Cancer: a biological approach. III. Viruses associated with neoplastic conditions. IV. Practical applications. Br Med J, 1957. 1(5023): p. 841-7.
6. Burnet, F.M., The concept of immunological surveillance. Prog Exp Tumor Res, 1970. 13: p. 1-27.
7. Van Snick, J., et al., Immunogenic variants obtained by mutagenesis of mouse masto cytoma p-815 5. h-2 associativity of variant specific antigens. European Journal of Immunology, 1982. 12(11): p. 905-908.
8. Urban, J.L., et al., Immunoselection of tumor cell variants by mice suppressed with ultraviolet radiation. J Exp Med, 1982. 156(4): p. 1025-41.
9. Dunn, G.P., et al., Cancer immunoediting: from immunosurveillance to tumor escape. Nat Immunol, 2002. 3(11): p. 991-8.
10. Algarra, I., A. Collado, and F. Garrido, Altered MHC class I antigens in tumors. Int J Clin Lab Res, 1997. 27(2): p. 95-102.
11. Garrido, F., et al., Implications for immunosurveillance of altered HLA class I phenotypes in human tumours. Immunol Today, 1997. 18(2): p. 89-95.
12. Ljunggren, H.G. and K. Karre, In Search of the Missing Self - Mhc Molecules and Nk Cell Recognition. Immunology Today, 1990. 11(7): p. 237-244.
13. Murphy, K.M. and S.L. Reiner, The lineage decisions of helper T cells. Nature Reviews Immunology, 2002. 2(12): p. 933-944.
14. Rosenberg, S.A., Progress in human tumour immunology and immunotherapy. Nature, 2001. 411(6835): p. 380-384.
15. Spaner, D.E., Amplifying cancer vaccine responses by modifying pathogenic gene programs in tumor cells. Journal of Leukocyte Biology, 2004. 76(2): p. 338-351.
77 78
16. Muranski, P., et al., Tumor-specific Th17-polarized cells eradicate large established melanoma. Blood, 2008. 112(2): p. 362-73.
17. Weaver, C.T., et al., Th17: an effector CD4 T cell lineage with regulatory T cell ties. Immunity, 2006. 24(6): p. 677-88.
18. Chalmin, F., et al., Stat3 and Gfi-1 transcription factors control Th17 cell immunosuppressive activity via the regulation of ectonucleotidase expression. Immunity, 2012. 36(3): p. 362-73.
19. Iwai, Y., et al., Involvement of PD-L1 on tumor cells in the escape from host immune system and tumor immunotherapy by PD-L1 blockade. Proceedings of the National Academy of Sciences of the United States of America, 2002. 99(19): p. 12293-12297.
20. Ishida, Y., et al., Induced Expression of Pd-1, a Novel Member of the Immunoglobulin Gene Superfamily, Upon Programmed Cell-Death. Embo Journal, 1992. 11(11): p. 3887- 3895.
21. Dong, H.D., et al., B7-H1, a third member of the B7 family, co-stimulates T-cell proliferation and interleukin-10 secretion. Nature Medicine, 1999. 5(12): p. 1365-1369.
22. Latchman, Y., et al., PD-L2, a novel B7 homologue, is a second ligand for PD-1 and inhibits T cell activation. Faseb Journal, 2001. 15(4): p. A345-A345.
23. Curti, A., et al., Modulation of tryptophan catabolism by human leukemic cells results in the conversion of CD25(-) into CD25(+) T regulatory cells. Blood, 2007. 109(7): p. 2871-2877.
24. Kryczek, I., et al., Relationship between B7-H4, regulatory T cells, and patient outcome in human ovarian carcinoma. Cancer Research, 2007. 67(18): p. 8900-8905.
25. Sica, G.L., et al., B7-H4, a molecule of the B7 family, negatively regulates T cell immunity. Immunity, 2003. 18(6): p. 849-61.
26. Sakaguchi, S., et al., Immunologic self-tolerance maintained by activated T cells expressing IL-2 receptor alpha-chains (CD25). Breakdown of a single mechanism of self- tolerance causes various autoimmune diseases. J Immunol, 1995. 155(3): p. 1151-64.
27. Chen, C., et al., Changes of CD4+CD25+FOXP3+ and CD8+CD28- regulatory T cells in non-small cell lung cancer patients undergoing surgery. Int Immunopharmacol, 2014. 18(2): p. 255-61.
28. Sayour, E.J., et al., Increased proportion of FoxP3+regulatory T cells in tumor infiltrating lymphocytes is associated with tumor recurrence and reduced survival in patients with glioblastoma. Cancer Immunology Immunotherapy, 2015. 64(4): p. 419- 427.
79
29. Curiel, T.J., et al., Specific recruitment of regulatory T cells in ovarian carcinoma fosters immune privilege and predicts reduced survival. Nature Medicine, 2004. 10(9): p. 942- 949.
30. Grossman, W.J., et al., Human T regulatory cells can use the perforin pathway to cause autologous target cell death. Immunity, 2004. 21(4): p. 589-601.
31. Chen, M.L., et al., Regulatory T cells suppress tumor-specific CD8 T cell cytotoxicity through TGF-beta signals in vivo. Proc Natl Acad Sci U S A, 2005. 102(2): p. 419-24.
32. Ostrand-Rosenberg, S. and P. Sinha, Myeloid-derived suppressor cells: linking inflammation and cancer. J Immunol, 2009. 182(8): p. 4499-506.
33. Rodriguez, P.C., et al., Arginase I production in the tumor microenvironment by mature myeloid cells inhibits T-cell receptor expression and antigen-specific T-cell responses. Cancer Res, 2004. 64(16): p. 5839-49.
34. Srivastava, M.K., et al., Myeloid-derived suppressor cells inhibit T-cell activation by depleting cystine and cysteine. Cancer Res, 2010. 70(1): p. 68-77.
35. Nagaraj, S., et al., Altered recognition of antigen is a novel mechanism of CD8+T cell tolerance in cancer. Proceedings of the American Association for Cancer Research Annual Meeting, 2007. 48: p. 377-378.
36. Baniyash, M., TCR zeta-chain downregulation: curtailing an excessive inflammatory immune response. Nat Rev Immunol, 2004. 4(9): p. 675-87.
37. Elkabets, M., et al., IL-1beta regulates a novel myeloid-derived suppressor cell subset that impairs NK cell development and function. Eur J Immunol, 2010. 40(12): p. 3347-57.
38. Huang, B., et al., Gr-1+CD115+ immature myeloid suppressor cells mediate the development of tumor-induced T regulatory cells and T-cell anergy in tumor-bearing host. Cancer Res, 2006. 66(2): p. 1123-31.
39. Sinha, P., et al., Cross-talk between myeloid-derived suppressor cells and macrophages subverts tumor immunity toward a type 2 response. Journal of Immunology, 2007. 179(2): p. 977-983.
40. Kohler, G. and C. Milstein, Continuous cultures of fused cells secreting antibody of predefined specificity. Nature, 1975. 256(5517): p. 495-7.
41. Morrison, S.L., et al., Chimeric Human-Antibody Molecules - Mouse Antigen-Binding Domains with Human Constant Region Domains. Proceedings of the National Academy of Sciences of the United States of America-Biological Sciences, 1984. 81(21): p. 6851- 6855.
42. Reichert, J.M., et al., Monoclonal antibody successes in the clinic. Nature Biotechnology, 2005. 23(9): p. 1073-1078.
80
43. Jones, P.T., et al., Replacing the Complementarity-Determining Regions in a Human- Antibody with Those from a Mouse. Nature, 1986. 321(6069): p. 522-525.
44. Cole, S.P.C., et al., A Strategy for the Production of Human Monoclonal-Antibodies Reactive with Lung-Tumor Cell-Lines. Cancer Research, 1984. 44(7): p. 2750-2753.
45. Smith, K.A., et al., T-cell growth factor-mediated T-cell proliferation. Ann N Y Acad Sci, 1979. 332: p. 423-32.
46. Lotze, M.T. and S.A. Rosenberg, Results of Clinical-Trials with the Administration of Interleukin-2 and Adoptive Immunotherapy with Activated Cells in Patients with Cancer. Immunobiology, 1986. 172(3-5): p. 420-437.
47. Rosenberg, S.A., et al., Use of Tumor-Infiltrating Lymphocytes and Interleukin-2 in the Immunotherapy of Patients with Metastatic Melanoma - a Preliminary-Report. New England Journal of Medicine, 1988. 319(25): p. 1676-1680.
48. Topalian, S.L., et al., Immunotherapy of Patients with Advanced Cancer Using Tumor- Infiltrating Lymphocytes and Recombinant Interleukin-2 - a Pilot-Study. Journal of Clinical Oncology, 1988. 6(5): p. 839-853.
49. Porter, D.L., et al., A phase 1 trial of donor lymphocyte infusions expanded and activated ex vivo via CD3/CD28 costimulation. Blood, 2006. 107(4): p. 1325-1331.
50. Levine, B.L., et al., Antiviral effect and ex vivo CD4(+) T cell proliferation in HIV- positive patients as a result of CD28 costimulation. Science, 1996. 272(5270): p. 1939- 1943.
51. Li, Y., et al., IL-15 activates telomerase and minimizes telomere loss and may preserve the replicative life span of memory CD8(+) T cells in vitiro. Journal of Immunology, 2005. 174(7): p. 4019-4024.
52. Klebanoff, C.A., et al., IL-15 enhances the in vivo antitumor activity of tumor-reactive CD8(+) T Cells. Proceedings of the National Academy of Sciences of the United States of America, 2004. 101(7): p. 1969-1974.
53. Hinrichs, C.S., et al., IL-2 and IL-21 confer opposing differentiation programs to CD8+ T cells for adoptive immunotherapy. Blood, 2008. 111(11): p. 5326-33.
54. Paulos, C.M., et al., The Inducible Costimulator (ICOS) Is Critical for the Development of Human T(H)17 Cells. Science Translational Medicine, 2010. 2(55).
55. Suhoski, M.M., et al., Engineering artificial antigen-presenting cells to express a diverse array of co-stimulatory molecules. Molecular Therapy, 2007. 15(5): p. 981-988.
56. Rosenberg, S.A., et al., Gene-transfer into humans - immunotherapy of patients with advanced melanoma, using tumor-infiltrating lymphocytes modified by retroviral gene transduction. New England Journal of Medicine, 1990. 323(9): p. 570-578.
81
57. Cavazzana-Calvo, M., et al., Gene therapy of human severe combined immunodeficiency (SCID)-X1 disease. Science, 2000. 288(5466): p. 669-72.
58. Hacein-Bey-Abina, S., et al., Efficacy of gene therapy for X-linked severe combined immunodeficiency. N Engl J Med, 2010. 363(4): p. 355-64.
59. Gaspar, H.B., et al., Long-term persistence of a polyclonal T cell repertoire after gene therapy for X-linked severe combined immunodeficiency. Sci Transl Med, 2011. 3(97): p. 97ra79.
60. Hacein-Bey-Abina, S., et al., Insertional oncogenesis in 4 patients after retrovirus- mediated gene therapy of SCID-X1. J Clin Invest, 2008. 118(9): p. 3132-42.
61. Howe, S.J., et al., Insertional mutagenesis combined with acquired somatic mutations causes leukemogenesis following gene therapy of SCID-X1 patients. J Clin Invest, 2008. 118(9): p. 3143-50.
62. Dull, T., et al., A third-generation lentivirus vector with a conditional packaging system. J Virol, 1998. 72(11): p. 8463-71.
63. Zufferey, R., et al., Multiply attenuated lentiviral vector achieves efficient gene delivery in vivo. Nat Biotechnol, 1997. 15(9): p. 871-5.
64. Zufferey, R., et al., Self-inactivating lentivirus vector for safe and efficient in vivo gene delivery. J Virol, 1998. 72(12): p. 9873-80.
65. Miyoshi, H., et al., Development of a self-inactivating lentivirus vector. J Virol, 1998. 72(10): p. 8150-7.
66. Cattoglio, C., et al., Hot spots of retroviral integration in human CD34+ hematopoietic cells. Blood, 2007. 110(6): p. 1770-8.
67. Ronen, K., et al., Distribution of lentiviral vector integration sites in mice following therapeutic gene transfer to treat beta-thalassemia. Mol Ther, 2011. 19(7): p. 1273-86.
68. Rittelmeyer, I., et al., Hepatic lentiviral gene transfer is associated with clonal selection, but not with tumour formation in serially transplanted mice. Human Gene Therapy, 2011. 22(10): p. A23-A23.
69. Rothe, M., et al., Hepatic Lentiviral Gene Transfer Is Associated with Mild Clonal Selection, but Not with Clonal Dominance or Tumour Formation in a Serial Transplantation Mouse Model. Molecular Therapy, 2012. 20: p. S161-S161.
70. Smee, D.F., et al., Anti-Herpesvirus Activity of the Acyclic Nucleoside 9-(1,3-Dihydroxy- 2-Propoxymethyl)Guanine. Antimicrobial Agents and Chemotherapy, 1983. 23(5): p. 676-682.
71. Bonini, C., et al., HSV-TK gene transfer into donor lymphocytes for control of allogeneic graft-versus-leukemia. Science, 1997. 276(5319): p. 1719-1724.
82
72. Berger, C., et al., Analysis of transgene-specific immune responses that limit the in vivo persistence of adoptively transferred HSV-TK-modified donor T cells after allogeneic hematopoietic cell transplantation. Blood, 2006. 107(6): p. 2294-2302.
73. Sato, T., et al., Engineered human tmpk/AZT as a novel enzyme/prodrug axis for suicide gene therapy. Mol Ther, 2007. 15(5): p. 962-70.
74. Neschadim, A., et al., Cell fate control gene therapy based on engineered variants of human deoxycytidine kinase. Mol Ther, 2012. 20(5): p. 1002-13.
75. Sunada, H., et al., Monoclonal-Antibody against Epidermal Growth-Factor Receptor Is Internalized without Stimulating Receptor Phosphorylation. Proceedings of the National Academy of Sciences of the United States of America, 1986. 83(11): p. 3825-3829.
76. Yang, X.D., et al., Development of ABX-EGF, a fully human anti-EGF receptor monoclonal antibody, for cancer therapy. Critical Reviews in Oncology Hematology, 2001. 38(1): p. 17-23.
77. Trotta, A.M., et al., Prospective Evaluation of Cetuximab-Mediated Antibody-Dependent Cell Cytotoxicity in Metastatic Colorectal Cancer Patients Predicts Treatment Efficacy. Cancer Immunol Res, 2016. 4(4): p. 366-74.
78. Van Cutsem, E., et al., Cetuximab and Chemotherapy as Initial Treatment for Metastatic Colorectal Cancer. New England Journal of Medicine, 2009. 360(14): p. 1408-1417.
79. Kuenen, B., et al., A phase I pharmacologic study of necitumumab (IMC-11F8), a fully human IgG1 monoclonal antibody directed against EGFR in patients with advanced solid malignancies. Clin Cancer Res, 2010. 16(6): p. 1915-23.
80. Weiner, L.M., et al., Dose and schedule study of panitumumab monotherapy in patients with advanced solid malignancies. Clin Cancer Res, 2008. 14(2): p. 502-8.
81. Chari, R.V., et al., Immunoconjugates containing novel maytansinoids: promising anticancer drugs. Cancer Res, 1992. 52(1): p. 127-31.
82. de Goeij, B.E. and J.M. Lambert, New developments for antibody-drug conjugate-based therapeutic approaches. Curr Opin Immunol, 2016. 40: p. 14-23.
83. Moskowitz, C.H., A. Nademanee, and T. Masszi, Brentuximab vedotin as consolidation therapy after autologous stem-cell transplantation in patients with Hodgkin's lymphoma at risk of relapse or progression (AETHERA): a randomised, double-blind, placebo- controlled, phase 3 trial (vol 385, pg 1853, 2015). Lancet, 2015. 386(9993): p. 532-532.
84. Verma, S., et al., Trastuzumab Emtansine for HER2-Positive Advanced Breast Cancer. New England Journal of Medicine, 2012. 367(19): p. 1783-1791.
85. Nurieva, R., et al., T-cell tolerance or function is determined by combinatorial costimulatory signals. Embo Journal, 2006. 25(11): p. 2623-2633.
83
86. Curtsinger, J.M., C.M. Johnson, and M.F. Mescher, CD8 T cell clonal expansion and development of effector function require prolonged exposure to antigen, costimulation, and signal 3 cytokine. Journal of Immunology, 2003. 171(10): p. 5165-5171.
87. Krummel, M.F. and J.P. Allison, Cd28 and Ctla-4 Have Opposing Effects on the Response of T-Cells to Stimulation. Journal of Experimental Medicine, 1995. 182(2): p. 459-465.
88. Walunas, T.L., et al., Ctla-4 Can Function as a Negative Regulator of T-Cell Activation. Immunity, 1994. 1(5): p. 405-413.
89. Wing, K., et al., CTLA-4 control over Foxp3(+) regulatory T cell function. Science, 2008. 322(5899): p. 271-275.
90. Read, S., V. Malmstrom, and F. Powrie, Cytotoxic T lymphocyte-associated antigen 4 plays an essential role in the function of CD25(+)CD4(+) regulatory cells that control intestinal inflammation. J Exp Med, 2000. 192(2): p. 295-302.
91. Matheu, M.P., et al., Imaging regulatory T cell dynamics and CTLA4-mediated suppression of T cell priming. Nature Communications, 2015. 6.
92. Hodi, F.S., et al., Improved Survival with Ipilimumab in Patients with Metastatic Melanoma. New England Journal of Medicine, 2010. 363(8): p. 711-723.
93. Robert, C., et al., Pembrolizumab versus Ipilimumab in Advanced Melanoma. New England Journal of Medicine, 2015. 372(26): p. 2521-2532.
94. Robert, C., et al., Anti-programmed-death-receptor-1 treatment with pembrolizumab in ipilimumab-refractory advanced melanoma: a randomised dose-comparison cohort of a phase 1 trial. Lancet, 2014. 384(9948): p. 1109-1117.
95. Brahmer, J.R., et al., Phase I Study of Single-Agent Anti-Programmed Death-1 (MDX- 1106) in Refractory Solid Tumors: Safety, Clinical Activity, Pharmacodynamics, and Immunologic Correlates. Journal of Clinical Oncology, 2010. 28(19): p. 3167-3175.
96. Powles, T., et al., MPDL3280A (anti-PD-L1) treatment leads to clinical activity in metastatic bladder cancer. Nature, 2014. 515(7528): p. 558-+.
97. Ansell, S.M., et al., PD-1 Blockade with Nivolumab in Relapsed or Refractory Hodgkin's Lymphoma. New England Journal of Medicine, 2015. 372(4): p. 311-319.
98. Larkin, J., F.S. Hodi, and J.D. Wolchok, Combined Nivolumab and Ipilimumab or Monotherapy in Untreated Melanoma REPLY. New England Journal of Medicine, 2015. 373(13): p. 1270-1271.
99. Rizvi, N.A., et al., Cancer immunology. Mutational landscape determines sensitivity to PD-1 blockade in non-small cell lung cancer. Science, 2015. 348(6230): p. 124-8.
84
100. Schoenbrunn, A., et al., A converse 4-1BB and CD40 ligand expression pattern delineates activated regulatory T cells (Treg) and conventional T cells enabling direct isolation of alloantigen-reactive natural Foxp3+ Treg. J Immunol, 2012. 189(12): p. 5985-94.
101. Shuford, W.W., et al., 4-1BB costimulatory signals preferentially induce CD8(+) T cell proliferation and lead to the amplification in vivo of cytotoxic T cell responses. Journal of Experimental Medicine, 1997. 186(1): p. 47-55.
102. Hurtado, J.C., Y.J. Kim, and B.S. Kwon, Signals through 4-1BB are costimulatory to previously activated splenic T cells and inhibit activation-induced cell death. Journal of Immunology, 1997. 158(6): p. 2600-2609.
103. Lee, H.W., et al., 4-1BB cross-linking enhances the survival and cell cycle progression of CD4 T lymphocytes. Cellular Immunology, 2003. 223(2): p. 143-150.
104. Melero, I., et al., NK1.1 cells express 4-1BB (CDw137) costimulatory molecule and are required for tumor immunity elicited by anti-4-1BB monoclonal antibodies. Cellular Immunology, 1998. 190(2): p. 167-172.
105. Kuang, Y.L., et al., Effects of 4-1BB signaling on the biological function of murine dendritic cells. Oncology Letters, 2012. 3(2): p. 477-481.
106. Smith, S.E., et al., Signals through 4-1BB inhibit T regulatory cells by blocking IL-9 production enhancing antitumor responses. Cancer Immunology Immunotherapy, 2011. 60(12): p. 1775-1787.
107. Chester, C., S. Ambulkar, and H.E. Kohrt, 4-1BB agonism: adding the accelerator to cancer immunotherapy. Cancer Immunol Immunother, 2016.
108. Herbst, R.S., et al., Predictive correlates of response to the anti-PD-L1 antibody MPDL3280A in cancer patients. Nature, 2014. 515(7528): p. 563-+.
109. Hamid, O., et al., A prospective phase II trial exploring the association between tumor microenvironment biomarkers and clinical activity of ipilimumab in advanced melanoma. Journal of Translational Medicine, 2011. 9.
110. Peng, W.Y., et al., Loss of PTEN Promotes Resistance to T Cell-Mediated Immunotherapy. Cancer Discovery, 2016. 6(2): p. 202-216.
111. Spranger, S., R. Bao, and T.F. Gajewski, Melanoma-intrinsic beta-catenin signalling prevents anti-tumour immunity. Nature, 2015. 523(7559): p. 231-5.
112. Kantoff, P.W., et al., Sipuleucel-T immunotherapy for castration-resistant prostate cancer. N Engl J Med, 2010. 363(5): p. 411-22.
113. Yang, J.C. and S.A. Rosenberg, Adoptive T-Cell Therapy for Cancer. Adv Immunol, 2016. 130: p. 279-94.
85
114. Rosenberg, S.A., et al., Durable Complete Responses in Heavily Pretreated Patients with Metastatic Melanoma Using T-Cell Transfer Immunotherapy. Clinical Cancer Research, 2011. 17(13): p. 4550-4557.
115. Dudley, M.E., et al., Cancer regression and autoimmunity in patients after clonal repopulation with antitumor lymphocytes. Science, 2002. 298(5594): p. 850-854.
116. Yannelli, J.R., et al., Growth of tumor-infiltrating lymphocytes from human solid cancers: Summary of a 5-year experience. International Journal of Cancer, 1996. 65(4): p. 413-421.
117. Dudley, M.E., et al., Generation of tumor-infiltrating lymphocyte cultures for use in adoptive transfer therapy for melanoma patients. Journal of Immunotherapy, 2003. 26(4): p. 332-342.
118. Cohen, C.J., et al., Enhanced antitumor activity of murine-human hybrid T-cell receptor (TCR) in human lymphocytes is associated with improved pairing and TCR/CD3 stability. Cancer Research, 2006. 66(17): p. 8878-8886.
119. Davis, J.L., et al., Development of Human Anti-Murine T-Cell Receptor Antibodies in Both Responding and Nonresponding Patients Enrolled in TCR Gene Therapy Trials. Clinical Cancer Research, 2010. 16(23): p. 5852-5861.
120. Johnson, L.A., et al., Gene therapy with human and mouse T-cell receptors mediates cancer regression and targets normal tissues expressing cognate antigen. Blood, 2009. 114(3): p. 535-546.
121. Chodon, T., et al., Adoptive Transfer of MART-1 T-Cell Receptor Transgenic Lymphocytes and Dendritic Cell Vaccination in Patients with Metastatic Melanoma. Clinical Cancer Research, 2014. 20(9): p. 2457-2465.
122. Robbins, P.F., et al., A Pilot Trial Using Lymphocytes Genetically Engineered with an NY-ESO-1-Reactive T-cell Receptor: Long-term Follow-up and Correlates with Response. Clinical Cancer Research, 2015. 21(5): p. 1019-1027.
123. Rapoport, A.P., et al., NY-ESO-1-specific TCR-engineered T cells mediate sustained antigen-specific antitumor effects in myeloma. Nature Medicine, 2015. 21(8): p. 914-921.
124. Kageyama, S., et al., Adoptive Transfer of MAGE-A4 T-cell Receptor Gene-Transduced Lymphocytes in Patients with Recurrent Esophageal Cancer. Clinical Cancer Research, 2015. 21(10): p. 2268-2277.
125. Morgan, R.A., et al., Cancer Regression and Neurological Toxicity Following Anti- MAGE-A3 TCR Gene Therapy. Journal of Immunotherapy, 2013. 36(2): p. 133-151.
126. Parkhurst, M.R., et al., T Cells Targeting Carcinoembryonic Antigen Can Mediate Regression of Metastatic Colorectal Cancer but Induce Severe Transient Colitis. Molecular Therapy, 2011. 19(3): p. 620-626.
86
127. Linette, G.P., et al., Cardiovascular toxicity and titin cross-reactivity of affinity-enhanced T cells in myeloma and melanoma. Blood, 2013. 122(6): p. 863-71.
128. Eshhar, Z., et al., Specific Activation and Targeting of Cytotoxic Lymphocytes through Chimeric Single Chains Consisting of Antibody-Binding Domains and the Gamma- Subunit or Zeta-Subunit of the Immunoglobulin and T-Cell Receptors. Proceedings of the National Academy of Sciences of the United States of America, 1993. 90(2): p. 720-724.
129. Moritz, D. and B. Groner, A Spacer Region between the Single-Chain Antibody-Chain and the Cd3 Zeta-Chain Domain of Chimeric T-Cell Receptor Components Is Required for Efficient Ligand-Binding and Signaling Activity. Gene Therapy, 1995. 2(8): p. 539- 546.
130. Carpenito, C., et al., Control of large, established tumor xenografts with genetically retargeted human T cells containing CD28 and CD137 domains. Proceedings of the National Academy of Sciences of the United States of America, 2009. 106(9): p. 3360- 3365.
131. Hombach, A.A., G. Rappl, and H. Abken, Arming Cytokine-induced Killer Cells With Chimeric Antigen Receptors: CD28 Outperforms Combined CD28 OX40 "Super- stimulation". Molecular Therapy, 2013. 21(12): p. 2268-2277.
132. Clinicaltrials.gov, NCT01853631. 2015, US National Library of Science.
133. Song, D.G., et al., CD27 costimulation augments the survival and antitumor activity of redirected human T cells in vivo. Blood, 2012. 119(3): p. 696-706.
134. Guedan, S., et al., ICOS-based chimeric antigen receptors program bipolar T(H)17/T(H)1 cells. Blood, 2014. 124(7): p. 1070-1080.
135. Curran, K.J., et al., Enhancing Antitumor Efficacy of Chimeric Antigen Receptor T Cells Through Constitutive CD40L Expression. Molecular Therapy, 2015. 23(4): p. 769-778.
136. Zhao, Z.G., et al., Structural Design of Engineered Costimulation Determines Tumor Rejection Kinetics and Persistence of CAR T Cells. Cancer Cell, 2015. 28(4): p. 415-428.
137. Pegram, H.J., et al., Tumor-targeted T cells modified to secrete IL-12 eradicate systemic tumors without need for prior conditioning. Blood, 2012. 119(18): p. 4133-4141.
138. Hoyos, V., et al., Engineering CD19-specific T lymphocytes with interleukin-15 and a suicide gene to enhance their anti-lymphoma/leukemia effects and safety. Leukemia, 2010. 24(6): p. 1160-1170.
139. Brentjens, R.J., et al., CD19-targeted T cells rapidly induce molecular remissions in adults with chemotherapy-refractory acute lymphoblastic leukemia. Sci Transl Med, 2013. 5(177): p. 177ra38.
140. Park, J., et al., Efficacy and Safety of Cd19-Targeted 19-28z Car Modified T Cells in Adult Patients with Relapsed or Refractory B-All. Haematologica, 2015. 100: p. 6-6.
87
141. Maude, S.L., et al., Chimeric Antigen Receptor T Cells for Sustained Remissions in Leukemia. New England Journal of Medicine, 2014. 371(16): p. 1507-1517.
142. Grupp, S.A., et al., Durable Remissions in Children with Relapsed/Refractory ALL Treated with T Cells Engineered with a CD19-Targeted Chimeric Antigen Receptor (CTL019). Blood, 2015. 126(23).
143. Porter, D.L., et al., Chimeric antigen receptor T cells persist and induce sustained remissions in relapsed refractory chronic lymphocytic leukemia. Sci Transl Med, 2015. 7(303): p. 303ra139.
144. Kochenderfer, J.N., et al., Chemotherapy-Refractory Diffuse Large B-Cell Lymphoma and Indolent B-Cell Malignancies Can Be Effectively Treated With Autologous T Cells Expressing an Anti-CD19 Chimeric Antigen Receptor. Journal of Clinical Oncology, 2015. 33(6): p. 540-U31.
145. Sauter, C.S., et al., Phase I trial of 19-28z chimeric antigen receptor modified T cells (19- 28z CAR-T) post-high dose therapy and autologous stem cell transplant (HDT-ASCT) for relapsed and refractory (rel/ref) aggressive B-cell non-Hodgkin lymphoma (B-NHL). Journal of Clinical Oncology, 2015. 33(15).
146. Sotillo, E., et al., Convergence of Acquired Mutations and Alternative Splicing of CD19 Enables Resistance to CART-19 Immunotherapy. Cancer Discovery, 2015. 5(12): p. 1282-1295.
147. Porter, D.L., et al., Chimeric Antigen Receptor-Modified T Cells in Chronic Lymphoid Leukemia. New England Journal of Medicine, 2011. 365(8): p. 725-733.
148. Grupp, S.A., et al., Chimeric Antigen Receptor-Modified T Cells for Acute Lymphoid Leukemia. New England Journal of Medicine, 2013. 368(16): p. 1509-1518.
149. Morgan, R.A., et al., Case report of a serious adverse event following the administration of T cells transduced with a chimeric antigen receptor recognizing ERBB2. Mol Ther, 2010. 18(4): p. 843-51.
150. Lamers, C.H., et al., Treatment of metastatic renal cell carcinoma with autologous T- lymphocytes genetically retargeted against carbonic anhydrase IX: first clinical experience. J Clin Oncol, 2006. 24(13): p. e20-2.
151. Wu, C.Y., et al., Remote control of therapeutic T cells through a small molecule-gated chimeric receptor. Science, 2015. 350(6258).
152. Kloss, C.C., et al., Combinatorial antigen recognition with balanced signaling promotes selective tumor eradication by engineered T cells. Nat Biotechnol, 2013. 31(1): p. 71-5.
153. Roybal, K.T., et al., Precision Tumor Recognition by T Cells With Combinatorial Antigen-Sensing Circuits. Cell, 2016. 164(4): p. 770-9.
88
154. Fedorov, V.D., M. Themeli, and M. Sadelain, PD-1- and CTLA-4-based inhibitory chimeric antigen receptors (iCARs) divert off-target immunotherapy responses. Sci Transl Med, 2013. 5(215): p. 215ra172.
155. Garfall, A.L., et al., Chimeric Antigen Receptor T Cells against CD19 for Multiple Myeloma. N Engl J Med, 2015. 373(11): p. 1040-7.
156. Clinicaltrials.gov, NCT02465983. 2015, US National Library of Science.
157. Bhat, R. and C. Watzl, Serial Killing of Tumor Cells by Human Natural Killer Cells - Enhancement by Therapeutic Antibodies. Plos One, 2007. 2(3).
158. Crouse, J., et al., NK cells regulating T cell responses: mechanisms and outcome. Trends Immunol, 2015. 36(1): p. 49-58.
159. Rosenberg, S.A., et al., Observations on the systemic administration of autologous lymphokine-activated killer cells and recombinant interleukin-2 to patients with metastatic cancer. N Engl J Med, 1985. 313(23): p. 1485-92.
160. Miller, J.S., et al., Successful adoptive transfer and in vivo expansion of human haploidentical NK cells in patients with cancer. Blood, 2005. 105(8): p. 3051-7.
161. Klingemann, H., Are natural killer cells superior CAR drivers? Oncoimmunology, 2014. 3: p. e28147.
162. Hermanson, D.L. and D.S. Kaufman, Utilizing chimeric antigen receptors to direct natural killer cell activity. Front Immunol, 2015. 6: p. 195.
163. Clinicaltrials.gov, NCT00995137. 2009, US National Library of Science.
164. Clinicaltrials.gov, NCT01974479. 2013, US National Library of Science.
165. Fujisaki, H., et al., Expansion of highly cytotoxic human natural killer cells for cancer cell therapy. Cancer Res, 2009. 69(9): p. 4010-7.
166. Gong, J.H., G. Maki, and H.G. Klingemann, Characterization of a human cell line (NK- 92) with phenotypical and functional characteristics of activated natural killer cells. Leukemia, 1994. 8(4): p. 652-8.
167. Arai, S., et al., Infusion of the allogeneic cell line NK-92 in patients with advanced renal cell cancer or melanoma: a phase I trial. Cytotherapy, 2008. 10(6): p. 625-32.
168. Tonn, T., et al., Treatment of patients with advanced cancer with the natural killer cell line NK-92. Cytotherapy, 2013. 15(12): p. 1563-70.
169. Cartron, G., et al., Therapeutic activity of humanized anti-CD20 monoclonal antibody and polymorphism in IgG Fc receptor FcgammaRIIIa gene. Blood, 2002. 99(3): p. 754-8.
89
170. Musolino, A., et al., Immunoglobulin G fragment C receptor polymorphisms and clinical efficacy of trastuzumab-based therapy in patients with HER-2/neu-positive metastatic breast cancer. J Clin Oncol, 2008. 26(11): p. 1789-96.
171. Klingemann, H., L. Boissel, and F. Toneguzzo, Natural Killer Cells for Immunotherapy - Advantages of the NK-92 Cell Line over Blood NK Cells. Front Immunol, 2016. 7: p. 91.
172. Klingemann, H.G., E. Wong, and G. Maki, A cytotoxic NK-cell line (NK-92) for ex vivo purging of leukemia from blood. Biol Blood Marrow Transplant, 1996. 2(2): p. 68-75.
173. Rollig, C., S. Knop, and M. Bornhauser, Multiple myeloma. Lancet, 2015. 385(9983): p. 2197-208.
174. Palumbo, A., et al., International Myeloma Working Group guidelines for the management of multiple myeloma patients ineligible for standard high-dose chemotherapy with autologous stem cell transplantation. Leukemia, 2009. 23(10): p. 1716-30.
175. Palumbo, A., M. Attal, and M. Roussel, Shifts in the therapeutic paradigm for patients newly diagnosed with multiple myeloma: maintenance therapy and overall survival. Clin Cancer Res, 2011. 17(6): p. 1253-63.
176. Harousseau, J.L., et al., Superior outcomes associated with complete response in newly diagnosed multiple myeloma patients treated with nonintensive therapy: analysis of the phase 3 VISTA study of bortezomib plus melphalan-prednisone versus melphalan- prednisone. Blood, 2010. 116(19): p. 3743-50.
177. Kagoya, Y., Y. Nannya, and M. Kurokawa, Thalidomide maintenance therapy for patients with multiple myeloma: meta-analysis. Leuk Res, 2012. 36(8): p. 1016-21.
178. Brinker, B.T., et al., Maintenance therapy with thalidomide improves overall survival after autologous hematopoietic progenitor cell transplantation for multiple myeloma. Cancer, 2006. 106(10): p. 2171-2180.
179. Wang, Y., et al., Maintenance Therapy With Immunomodulatory Drugs in Multiple Myeloma: A Meta-Analysis and Systematic Review. J Natl Cancer Inst, 2016. 108(3).
180. Attal, M., et al., Lenalidomide maintenance after stem-cell transplantation for multiple myeloma. N Engl J Med, 2012. 366(19): p. 1782-91.
181. McCarthy, P.L., et al., Lenalidomide after stem-cell transplantation for multiple myeloma. N Engl J Med, 2012. 366(19): p. 1770-81.
182. Palumbo, A., et al., Continuous lenalidomide treatment for newly diagnosed multiple myeloma. N Engl J Med, 2012. 366(19): p. 1759-69.
183. Funaro, A., et al., Involvement of the Multilineage Cd38 Molecule in a Unique Pathway of Cell Activation and Proliferation. Journal of Immunology, 1990. 145(8): p. 2390-2396.
90
184. Leo, R., et al., Multiparameter Analyses of Normal and Malignant Human Plasma-Cells - Cd38++, Cd56+, Cd54+, Cig+ Is the Common Phenotype of Myeloma Cells. Annals of Hematology, 1992. 64(3): p. 132-139.
185. de Weers, M., et al., Daratumumab, a Novel Therapeutic Human CD38 Monoclonal Antibody, Induces Killing of Multiple Myeloma and Other Hematological Tumors. Journal of Immunology, 2011. 186(3): p. 1840-1848.
186. Deckert, J., et al., SAR650984, A Novel Humanized CD38-Targeting Antibody, Demonstrates Potent Antitumor Activity in Models of Multiple Myeloma and Other CD38(+) Hematologic Malignancies. Clinical Cancer Research, 2014. 20(17): p. 4574- 4583.
187. Martin, T.G., et al., SAR650984, a CD38 Monoclonal Antibody In Patients With Selected CD38+Hematological Malignancies- Data From a Dose-Escalation Phase I Study. Blood, 2013. 122(21).
188. Lokhorst, H.M., et al., Targeting CD38 with Daratumumab Monotherapy in Multiple Myeloma. New England Journal of Medicine, 2015. 373(13): p. 1207-1219.
189. Martin, T.G., et al., A Phase Ib Dose Escalation Trial of SAR650984 (Anti-CD-38 mAb) in Combination with Lenalidomide and Dexamethasone in Relapsed/Refractory Multiple Myeloma. Blood, 2014. 124(21).
190. Plesner, T., et al., Safety and Efficacy of Daratumumab with Lenalidomide and Dexamethasone in Relapsed or Relapsed, Refractory Multiple Myeloma. Blood, 2014. 124(21).
191. Mihara, K., et al., Activated T-cell-mediated Immunotherapy With a Chimeric Receptor Against CD38 in B-cell Non-Hodgkin Lymphoma. Journal of Immunotherapy, 2009. 32(7): p. 737-743.
192. Westendorf, J.J., et al., Cd40 Expression in Malignant Plasma-Cells - Role in Stimulation of Autocrine Il-6 Secretion by a Human Myeloma Cell-Line. Journal of Immunology, 1994. 152(1): p. 117-128.
193. Tai, Y.T., et al., CD40 induces human multiple myeloma. cell migration via phosphatidylinositol 3-kinase/AKT/NF-kappa B signaling. Blood, 2003. 101(7): p. 2762- 2769.
194. Francisco, J.A., et al., Agonistic properties and in vivo antitumor activity of the anti- CD40 antibody SGN-14. Cancer Research, 2000. 60(12): p. 3225-3231.
195. Tai, Y.T., et al., Mechanisms by which SGN-40, a humanized anti-CD40 antibody, induces cytotoxicity in human multiple myeloma cells: Clinical implications. Cancer Research, 2004. 64(8): p. 2846-2852.
91
196. Hayashi, T., et al., Recombinant humanized anti-CD40 monoclonal antibody triggers autologous antibody-dependent cell-mediated cytotoxicity against multiple myeloma cells. British Journal of Haematology, 2003. 121(4): p. 592-596.
197. Hussein, M., et al., A phase I multidose study of dacetuzumab (SGN-40; humanized anti- CD40 monoclonal antibody) in patients with multiple myeloma. Haematologica, 2010. 95(5): p. 845-8.
198. Agura, E., et al., Dacetuzurmab (SGN-40), Lenalidomide, and Weekly Dexamethasone in Relapsed or Refractory Multiple Myeloma: Multiple Responses Observed in a Phase 1b Study. Blood, 2009. 114(22): p. 1120-1121.
199. Luqman, M., et al., The antileukemia activity of a human anti-CD40 antagonist antibody, HCD122, on human chronic lymphocytic leukemia cells. Blood, 2008. 112(3): p. 711- 720.
200. Bensinger, W., et al., A phase 1 study of lucatumumab, a fully human anti-CD40 antagonist monoclonal antibody administered intravenously to patients with relapsed or refractory multiple myeloma. British Journal of Haematology, 2012. 159(1): p. 58-66.
201. Vancamp, B., et al., Plasma-Cells in Multiple-Myeloma Express a Natural-Killer Cell- Associated Antigen - Cd56 (Nkh-1, Leu-19). Blood, 1990. 76(2): p. 377-382.
202. Tassone, P., et al., In vitro and in vivo activity of the maytansinoid immunoconjugate huN901-N-2 '-deacetyl-N-2 '-(3-mercapto-1-oxopropyl)-maytansine against CD56(+) multiple myeloma cells. Cancer Research, 2004. 64(13): p. 4629-4636.
203. Berdeja, J.G., et al., Phase I Study of Lorvotuzumab Mertansine (LM, IMGN901) in Combination with Lenalidomide (Len) and Dexamethasone (Dex) in Patients with CD56- Positive Relapsed or Relapsed/Refractory Multiple Myeloma (MM). Blood, 2012. 120(21).
204. Claesson, L., et al., Cdna Clone for the Human Invariant Gamma-Chain of Class-Ii Histocompatibility Antigens and Its Implications for the Protein-Structure. Proceedings of the National Academy of Sciences of the United States of America-Biological Sciences, 1983. 80(24): p. 7395-7399.
205. Stein, R., et al., CD74: A new candidate target for the immunotherapy of B-Cell neoplasms. Clinical Cancer Research, 2007. 13(18): p. 5556s-5563s.
206. Burton, J.D., et al., CD74 is expressed by multiple myeloma and is a promising target for therapy. Clinical Cancer Research, 2004. 10(19): p. 6606-6611.
207. Kaufman, J.L., et al., Phase I, multicentre, dose-escalation trial of monotherapy with milatuzumab (humanized anti-CD74 monoclonal antibody) in relapsed or refractory multiple myeloma. Br J Haematol, 2013. 163(4): p. 478-86.
208. Clinicaltrials.gov, NCT01101594. 2010, US National Library of Science.
92
209. Sanderson, R.D., et al., Fine structure of heparan sulfate regulates syndecan-1 function and cell behavior. J Biol Chem, 1994. 269(18): p. 13100-6.
210. Zimmermann, P. and G. David, The syndecans, tuners of transmembrane signaling. FASEB J, 1999. 13 Suppl: p. S91-S100.
211. Fuki, I.V., M.E. Meyer, and K.J. Williams, Transmembrane and cytoplasmic domains of syndecan mediate a multi-step endocytic pathway involving detergent-insoluble membrane rafts. Biochemical Journal, 2000. 351: p. 607-612.
212. Seidel, C., et al., Serum syndecan-1: a new independent prognostic marker in multiple myeloma. Blood, 2000. 95(2): p. 388-92.
213. Purushothaman, A., et al., Heparanase-enhanced shedding of syndecan-1 by myeloma cells promotes endothelial invasion and angiogenesis. Blood, 2010. 115(12): p. 2449-57.
214. Brockstedt, U., et al., Immunoreactivity to cell surface syndecans in cytoplasm and nucleus: tubulin-dependent rearrangements. Exp Cell Res, 2002. 274(2): p. 235-45.
215. Wijdenes, J., et al., A plasmocyte selective monoclonal antibody (B-B4) recognizes syndecan-1. British Journal of Haematology, 1996. 94(2): p. 318-323.
216. Lin, P., et al., Flow cytometric immunophenotypic analysis of 306 cases of multiple myeloma. American Journal of Clinical Pathology, 2004. 121(4): p. 482-488.
217. Kelly, K.R., et al., Indatuximab Ravtansine (BT062) in Combination with Lenalidomide and Low-Dose Dexamethasone in Patients with Relapsed and/or Refractory Multiple Myeloma: Clinical Activity in Patients Already Exposed to Lenalidomide and Bortezomib. Blood, 2014. 124(21).
218. Clinicaltrials.gov, NCT01886976
. 2013, US National Library of Science.
219. Guo, B., et al., CD138-directed adoptive immunotherapy of chimeric antigen receptor (CAR)-modified T cells for multiple myeloma. Journal of Cellular Immunotherapy, 2016. 2(1): p. 28-35.
220. Laabi, Y., et al., The Bcma Gene, Preferentially Expressed during B-Lymphoid Maturation, Is Bidirectionally Transcribed. Nucleic Acids Research, 1994. 22(7): p. 1147-1154.
221. Moreaux, J., et al., BAFF and APRIL protect myeloma cells from apoptosis induced by interleukin 6 deprivation and dexamethasone. Blood, 2004. 103(8): p. 3148-3157.
222. Tai, Y.T., et al., Novel anti-B-cell maturation antigen antibody-drug conjugate (GSK2857916) selectively induces killing of multiple myeloma. Blood, 2014. 123(20): p. 3128-3138.
93
223. Clinicaltrials.gov, NCT02064387. 2014, US National Library of Science.
224. Ali, S.A., et al., Remissions of Multiple Myeloma during a First-in-Humans Clinical Trial of T Cells Expressing an Anti-B-Cell Maturation Antigen Chimeric Antigen Receptor. Blood, 2015. 126(23).
225. Murphy, J.J., et al., A novel immunoglobulin superfamily receptor (19A) related to CD2 is expressed on activated lymphocytes and promotes homotypic B-cell adhesion. Biochemical Journal, 2002. 361: p. 431-436.
226. Hsi, E.D., et al., CS1, a potential new therapeutic antibody target for the treatment of multiple myeloma. Clinical Cancer Research, 2008. 14(9): p. 2775-2784.
227. Tai, Y.T., et al., Anti-CS1 humanized monoclonal antibody HuLuc63 inhibits myeloma cell adhesion and induces aritibody-dependent cellular cytotoxicity in the bone marrow mitieu. Blood, 2008. 112(4): p. 1329-1337.
228. Lonial, S., et al., Elotuzumab Therapy for Relapsed or Refractory Multiple Myeloma. New England Journal of Medicine, 2015. 373(7): p. 621-631.
229. Chu, J., et al., CS1-specific chimeric antigen receptor (CAR)-engineered natural killer cells enhance in vitro and in vivo antitumor activity against human multiple myeloma. Leukemia, 2014. 28(4): p. 917-927.
230. Chu, J.H., et al., CS1-Specific Chimeric Antigen Receptor (CAR)-Engineered NK Cells and T Cells Enhance In Vitro and In Vivo Anti-Tumor Activity Against Human Multiple Myeloma. Blood, 2013. 122(21).
231. Noonan, K.A., et al., Adoptive transfer of activated marrow-infiltrating lymphocytes induces measurable antitumor immunity in the bone marrow in multiple myeloma. Sci Transl Med, 2015. 7(288): p. 288ra78.
232. Bates, S. and K.H. Vousden, p53 in signaling checkpoint arrest or apoptosis. Curr Opin Genet Dev, 1996. 6(1): p. 12-8.
233. Hupp, T.R., et al., Regulation of the specific DNA binding function of p53. Cell, 1992. 71(5): p. 875-86.
234. Keller, D.M., et al., A DNA damage-induced p53 serine 392 kinase complex contains CK2, hSpt16, and SSRP1. Mol Cell, 2001. 7(2): p. 283-92.
235. Song, H., M. Hollstein, and Y. Xu, p53 gain-of-function cancer mutants induce genetic instability by inactivating ATM. Nat Cell Biol, 2007. 9(5): p. 573-80.
236. Strano, S., et al., Mutant p53: an oncogenic transcription factor. Oncogene, 2007. 26(15): p. 2212-9.
237. Strano, S., et al., Physical interaction with human tumor-derived p53 mutants inhibits p63 activities. J Biol Chem, 2002. 277(21): p. 18817-26.
94
238. Yap, D.B., et al., Ser392 phosphorylation regulates the oncogenic function of mutant p53. Cancer Res, 2004. 64(14): p. 4749-54.
239. Wang, Z., et al., Universal PCR amplification of mouse immunoglobulin gene variable regions: the design of degenerate primers and an assessment of the effect of DNA polymerase 3' to 5' exonuclease activity. J Immunol Methods, 2000. 233(1-2): p. 167-77.
240. Gill, S., et al., Preclinical targeting of human acute myeloid leukemia and myeloablation using chimeric antigen receptor-modified T cells. Blood, 2014. 123(15): p. 2343-54.
241. Jena, B., et al., Chimeric antigen receptor (CAR)-specific monoclonal antibody to detect CD19-specific T cells in clinical trials. PLoS One, 2013. 8(3): p. e57838.
242. Nilson, B.H., et al., Protein L from Peptostreptococcus magnus binds to the kappa light chain variable domain. J Biol Chem, 1992. 267(4): p. 2234-9.
243. Zheng, Z., N. Chinnasamy, and R.A. Morgan, Protein L: a novel reagent for the detection of chimeric antigen receptor (CAR) expression by flow cytometry. J Transl Med, 2012. 10: p. 29.
244. Muzard, J., et al., Grafting of protein L-binding activity onto recombinant antibody fragments. Anal Biochem, 2009. 388(2): p. 331-8.
245. Cao, L.F., et al., Development and application of a multiplexable flow cytometry-based assay to quantify cell-mediated cytolysis. Cytometry A, 2010. 77(6): p. 534-45.
246. David, G., Integral membrane heparan sulfate proteoglycans. FASEB J, 1993. 7(11): p. 1023-30.
247. Godfrey, J. and D.M. Benson, Jr., The role of natural killer cells in immunity against multiple myeloma. Leuk Lymphoma, 2012. 53(9): p. 1666-76.
248. Savoldo, B., et al., Epstein Barr virus specific cytotoxic T lymphocytes expressing the anti-CD30zeta artificial chimeric T-cell receptor for immunotherapy of Hodgkin disease. Blood, 2007. 110(7): p. 2620-30.
249. Wang, X., et al., CMVpp65 Vaccine Enhances the Antitumor Efficacy of Adoptively Transferred CD19-Redirected CMV-Specific T Cells. Clin Cancer Res, 2015. 21(13): p. 2993-3002.
250. Chesi, M., et al., AID-dependent activation of a MYC transgene induces multiple myeloma in a conditional mouse model of post-germinal center malignancies. Cancer Cell, 2008. 13(2): p. 167-80.
251. Yaccoby, S., B. Barlogie, and J. Epstein, Primary myeloma cells growing in SCID-hu mice: a model for studying the biology and treatment of myeloma and its manifestations. Blood, 1998. 92(8): p. 2908-13.
95
252. Bakkus, M.H.C., et al., Evidence that multiple-myeloma ig heavy-chain vdj-genes contain somatic mutations but show no intraclonal variation. Blood, 1992. 80(9): p. 2326-2335.
253. Frigyesi, I., et al., Robust isolation of malignant plasma cells in multiple myeloma. Blood, 2014. 123(9): p. 1336-40.
254. Matsui, W., et al., Clonogenic multiple myeloma progenitors, stem cell properties, and drug resistance. Cancer Res, 2008. 68(1): p. 190-7.
255. Hosen, N., Multiple myeloma-initiating cells. Int J Hematol, 2013. 97(3): p. 306-12.
256. Kim, D., et al., CD19-CD45 low/- CD38 high/CD138+ plasma cells enrich for human tumorigenic myeloma cells. Leukemia, 2012. 26(12): p. 2530-7.
257. Jiang, H., et al., Transfection of chimeric anti-CD138 gene enhances natural killer cell activation and killing of multiple myeloma cells. Mol Oncol, 2014. 8(2): p. 297-310.
258. Sun, W.P., et al., A novel anti-human syndecan-1 (CD138) monoclonal antibody 4B3: characterization and application. Cell Mol Immunol, 2007. 4(3): p. 209-14.
259. Otahal, P., et al., Lenalidomide enhances antitumor functions of chimeric antigen receptor modified T cells. Oncoimmunology, 2016. 5(4): p. e1115940.
260. James, J.R. and R.D. Vale, Biophysical mechanism of T-cell receptor triggering in a reconstituted system. Nature, 2012. 487(7405): p. 64-9.
261. Wittrup, A., et al., ScFv antibody-induced translocation of cell-surface heparan sulfate proteoglycan to endocytic vesicles: evidence for heparan sulfate epitope specificity and role of both syndecan and glypican. J Biol Chem, 2009. 284(47): p. 32959-67.
262. Chen, K. and K.J. Williams, Molecular mediators for raft-dependent endocytosis of syndecan-1, a highly conserved, multifunctional receptor. J Biol Chem, 2013. 288(20): p. 13988-99.
263. Gajate, C., et al., Intracellular triggering of Fas aggregation and recruitment of apoptotic molecules into Fas-enriched rafts in selective tumor cell apoptosis. J Exp Med, 2004. 200(3): p. 353-65.
264. White, A.L., et al., Conformation of the human immunoglobulin G2 hinge imparts superagonistic properties to immunostimulatory anticancer antibodies. Cancer Cell, 2015. 27(1): p. 138-48.
265. Richards, C.H., et al., The relationships between cellular components of the peritumoural inflammatory response, clinicopathological characteristics and survival in patients with primary operable colorectal cancer. British Journal of Cancer, 2012. 106(12): p. 2010- 2015.
96
266. Schmidt, M., et al., A Comprehensive Analysis of Human Gene Expression Profiles Identifies Stromal Immunoglobulin kappa C as a Compatible Prognostic Marker in Human Solid Tumors. Clinical Cancer Research, 2012. 18(9): p. 2695-2703.
267. Nielsen, J.S., et al., CD20(+) Tumor-Infiltrating Lymphocytes Have an Atypical CD27(-) Memory Phenotype and Together with CD8(+) T Cells Promote Favorable Prognosis in Ovarian Cancer. Clinical Cancer Research, 2012. 18(12): p. 3281-3292.
268. Kroeger, D.R., K. Milne, and B.H. Nelson, Tumor-Infiltrating Plasma Cells Are Associated with Tertiary Lymphoid Structures, Cytolytic T-Cell Responses, and Superior Prognosis in Ovarian Cancer. Clin Cancer Res, 2016.
269. Shortt, J. and A. Spencer, Adjuvant rituximab causes prolonged hypogammaglobulinaemia following autologous stem cell transplant for non-Hodgkin's lymphoma. Bone Marrow Transplant, 2006. 38(6): p. 433-6.
270. Lowe, D. CAR-T Deaths Cannot Be Good. 2016.
97