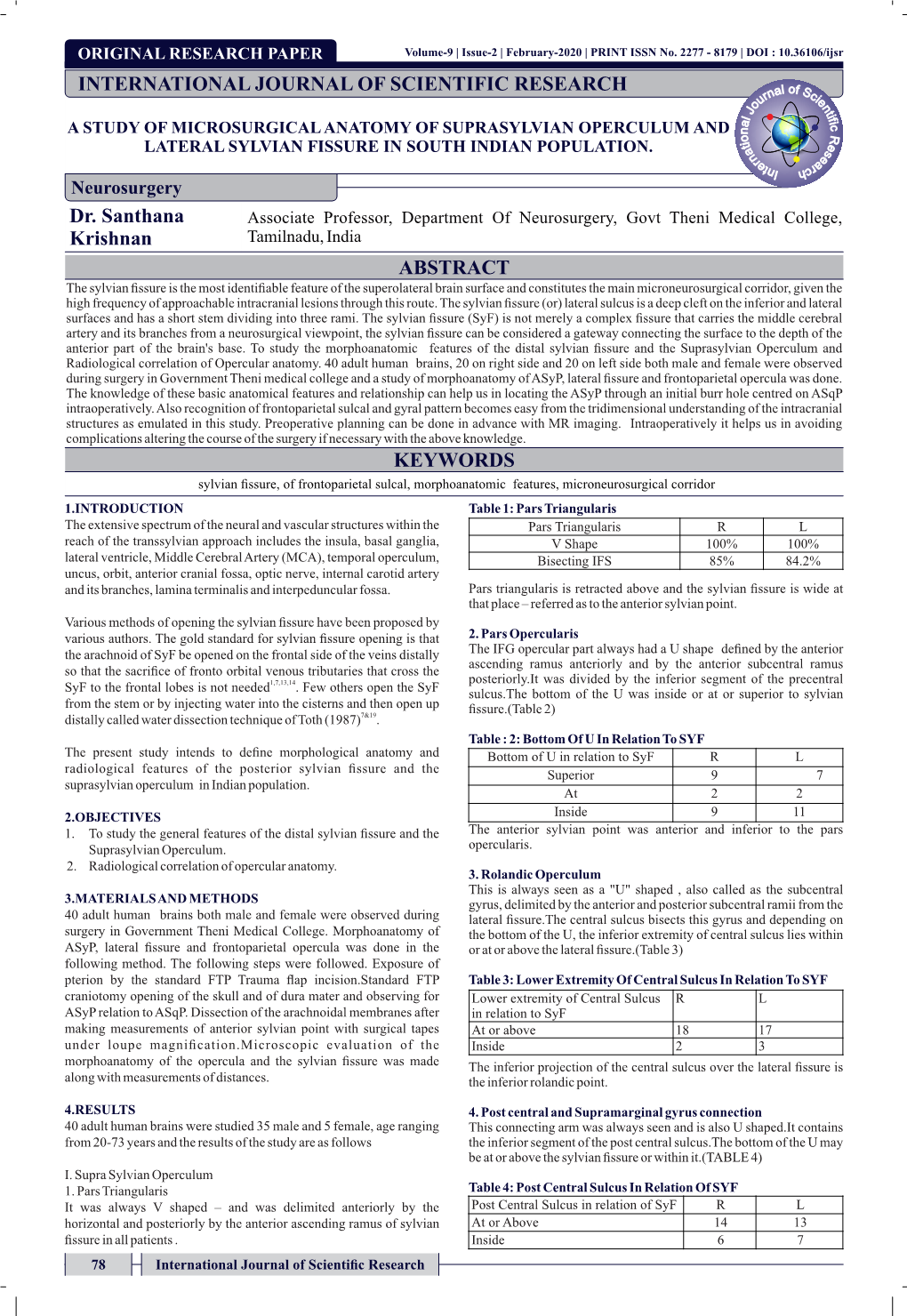
Dr. Santhana Krishnan INTERNATIONAL JOURNAL OF
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Awareness Among Diabetic Patients
IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-ISSN: 2279-0853, p-ISSN: 2279-0861.Volume 15, Issue 10 Ver. VII (October. 2016), PP 39-41 www.iosrjournals.org A Prospective Study -Awareness among Diabetic Patients Dr.S.M.Thirunaukkarasu.M.D1, Dr.S.Sopna Jothi,M.D2, DR.P.Purushothaman,M.D3. Dr.S.Ganesh Babu.M.S4, Dr.T.Ravikumar.M.D5, Dr.P.Saravananm.D6, Dr.Malini,M.D7, Dr.Indhu M.D8. 1Associate Professor Of Medicine Govt Theni Medical College Theni , 2Asst Professor Of Medicine Govt Theni Medical College Theni , 3Professor And. HOD of Medicine Govt Theni Medical College Theni, 4 Professor Of Surgery Govt Theni Medical College Theni , 5Professor and Hod of Medicine, Govt Medical College And ESI HospitalCoimbatore, 6Asst.Professor-of Medicine Madurai Medical College Madurai, 7Asst.Professer Govt Medical College and ESI hospital coimbatore. Abstract: Morbidity and mortality due diabetes in all over world is alarming .We submit a study done over 3 months in the tertiary care hospital in southern part of Tamil nadu Aim Of The Study: The aim of the study is to check the knowledge of the patients prove that educating will improve the outcome. Material And Methods: This is a prospective observational study in a tertiary medical care hospital , in southern part of Tamil Nadu , south India, during september 2016with in 50 patients all are presented with diabetes, on regular treatment (type1 and type 2 on insulin) Results: many patients aware of their disease and management. Majority of them know when to adjust the dose of insulin and our aim is to provide100 percent knowledge Conclusion:. -
Research Methodology and Biostatistics” for Affiliated Institutions of the Tamil Nadu Dr.M.G.R Medical University As Per the Given Schedule
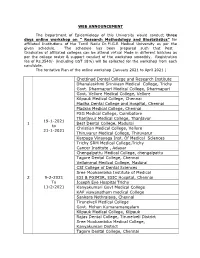
WEB ANNOUNCEMENT The Department of Epidemiology of this University would conduct three days online workshop on “ Research Methodology and Biostatistics” for affiliated Institutions of the Tamil Nadu Dr.M.G.R Medical University as per the given schedule. The schedule has been prepared such that Post Graduates of affiliated colleges can be attend virtual Mode in different batches as per the college roster & support conduct of the workshop smoothly. Registration fee of Rs.3540/- (including GST 18%) will be collected for the workshop from each candidate. The tentative Plan of the online workshop (January 2021 to April 2021 ) Chettinad Dental College and Research Institute Dhanalaskhmi Srinivasn Medical College, Trichy Govt. Dharmapuri Medical College, Dharmapuri Govt. Vellore Medical College, Vellore Kilpauk Medical College, Chennai Madha Dental College and Hospital, Chennai Madras Medical College, Chennai PSG Medical College, Coimbatore Thanjavur Medical College, Thanjavur 19-1-2021 1 Best Dental College, Madurai to Christian Medical College, Vellore 21-1-2021 Thiruvarur Medical College, Thiruvarur Karpaga Vinayaga Inst. Of Medical Sciences Trichy SRM Medical College,Trichy Cancer Institute , Adayar Chengalpattu Medical College, chengalpattu Tagore Dental College, Chennai Vellammal Medical College, Madurai CSI College of Dental Sciences Sree Mookambika Institute of Medical 29-2-2021 ESI & PGIMSR, ESIC Hospital, Chennai To Joseph Eye Hospital Trichy 11-2-2021 Kanyakumari Govt Medical College KAP viswanatham medical College Sankara Nethralaya, Chennai Tirunelveli Medical College Govt. Mohan Kumaramangalam Kilpauk Medical College, Kilpauk Rajas Dental College, Tirunelveli District Sree Mookambika Medical College, Kanyakumari District Tagore Dental College, Chennai Trichy SRM Medical College,Trichy Vivekanandha Dental College for Women, Namakkal Christian medical College, Vellore Govt. -

Directorate of Medical Education
1 Directorate of Medical Education Hand Book on Right to Information Act - 2005 2 CHAPT ER DETAILS PAGE NO NO. 1. INTRODUCTION 3 2 PARTICULARS OF ORGANISATION, FUNCTIONS AND DUTIES 5 3 POWERS AND DUTIES OF OFFICERS AND EMPLOYEES 80 4 RULES, REGULATIONS,INSTRUCTIONS, MANUAL AND RECORDS 91 FOR DISCHARGING FUNCTIONS 5 PARTICULARS OF ANY ARRANGEMENT THAT EXISTS FOR 93 CONSULTATION WITH OR REPRESENTATION BY THE MEMBERS OF THE PUBLIC IN RELATION TO THE FORMULATION OF ITS POLICY OR IMPLEMENTATION THEREOF 6 A STATEMENT OF THE CATEGORIES OF DOCUMENTS THAT ARE 94 HELD BY IT OR UNDER ITS CONTROL 7 A STATEMENT OF BOARDS, COUNCIL, COMMITTEES AND OTHER 95 BODIES CONSTITUTED AS ITS PART 8 THE NAMES, DESIGNATION AND OTHER PARTICULARS OF THE 96 PUBLIC INFORMATION OFFICER 9 PROCEDURE FOLLOWED IN DECISION MAKING PROCESS 107 10 DIRECTORY OF OFFICERS AND EMPLOYEES 108 11 THE MONTHLY REMUNERATION RECEIVED BY EACH OF ITS 110 OFFICERS AND EMPLOYEES INCLUDING THE SYSTEM OF COMPENSATION AS PROVIDED IN REGULATIONS. 12 THE BUDGET ALLOCATED TO EACH AGENCY/OFFICERS 111 (PARTICULARS OF ALL PLANS, PROPOSED EXPENDITURES AND REPORTS ON DISBURSEMENT MADE 116 13 THE MANNER OF EXECUTION OR SUBSIDY PROGRAMME 14 PARTICULARS OF RECEIPIENTS OF CONCESSIONS, PERMITS OR 117 AUTHORISATION GRANTED BY IT 15 NORMS SET BY IT FOR THE DISCHARGE OF ITS FUNCTIONS 118 16 INFORMATION AVAILABLE IN AN ELECTRONIC FORM 119 17 PARTICULARS OF THE FACILITIES AVAILABLE TO CITIZENS FOR 120 OBTAINING THE INFORMATION 18 OTHER USEFUL INFORMATION 121 3 CHAPTER-1 - INTRODUCTION 1.1This handbook is brought out by the Directorate of Medical Education (Government of Tamil Nadu) , Chennai as required by the Right to Information Act, 2005. -

CTRI Trial Data
PDF of Trial CTRI Website URL - http://ctri.nic.in Clinical Trial Details (PDF Generation Date :- Fri, 01 Oct 2021 19:42:24 GMT) CTRI Number CTRI/2020/06/025874 [Registered on: 15/06/2020] - Trial Registered Prospectively Last Modified On 15/06/2020 Post Graduate Thesis No Type of Trial Interventional Type of Study Siddha Study Design Randomized, Parallel Group Trial Public Title of Study To observe the effect of Siddha formulation Kabasura kudineer in COVID 19 patients Scientific Title of A randomized open labeled clinical study to compare the effectiveness of Kabasura kudineer and Study Vitamin-C Zinc supplementation in the management of asymptomatic SARS-CoV-2 patients Secondary IDs if Any Secondary ID Identifier NIL NIL Details of Principal Details of Principal Investigator Investigator or overall Name Dr P Sankararaj Trial Coordinator (multi-center study) Designation Assistant Medical Officer Siddha Affiliation Government Theni Medical College and Hospital Address Siddha wing Government Theni Medical College and Hospital Kochi - Madurai - Dhanushkodi Rd, Theni Allinagaram, Tamil Nadu 625531 Kochi - Madurai - Dhanushkodi Rd, Theni Allinagaram, Tamil Nadu 625531 Theni TAMIL NADU 625531 India Phone 9965897075 Fax Email [email protected] Details Contact Details Contact Person (Scientific Query) Person (Scientific Name Dr P Sankararaj Query) Designation Assistant Medical Officer Siddha Affiliation Government Theni Medical College and Hospital Address Siddha wing Government Theni Medical College and Hospital Kochi - Madurai - Dhanushkodi -

Para Medical Courses - 2019 - 2020 Session List of Candidates Allotted on 10.09.2019
PARA MEDICAL COURSES - 2019 - 2020 SESSION LIST OF CANDIDATES ALLOTTED ON 10.09.2019 COLLEGE : Madras Medical College, Chennai SNO RANK ARNO NAME TOTAL COMM. COURSE JOIN DATE MARKS 1 1 16111 LUBNA SHERIN 196.50 BCM B.A.S.L.P 2 2 15841 ABDUL RAHMAN S 195.00 BCM B.Pharm 3 4 792 HAMSSIKA S 194.50 OC B.A.S.L.P 4 14 7915 JAYASHREE E 190.75 BC B.Pharm 5 15 139 SURYA PRIYA B 190.50 OC B.Pharm 6 16 644 BOOMIKA T 190.00 BC B.Pharm 7 19A 13725 ANUSHA S 189.50 BC B.Sc.(Nursing) 8 21 9499 RAGUPATHI R 189.50 MBC/DNC B.Pharm 9 23 16586 MOHAN K 189.00 BC B.Sc. Cardio-Pulmonary 10 25 13420 A.ROHINI 189.00 BC B.Sc.(Nursing) 11 26 5613 MUKILAN K 189.00 BC B.A.S.L.P 12 32 14740 SINDHU J A 188.00 MBC/DNC B.Sc. Cardio-Pulmonary 13 34 1394 JEYA SHREE N 187.50 BC B.Sc.(Nursing) 14 36 21067 RANJITHAM M 187.50 MBC/DNC B.Pharm 15 44 2249 VISAKA E M 186.50 MBC/DNC B.Sc. Cardio-Pulmonary 16 46 6664 VENGATESH K G 186.50 MBC/DNC B.Pharm 17 49 21373 ABITHA T 186.25 BC B.Sc.(Nursing) 18 51 1533 AYSHA YASMEEN S 186.00 BCM B.Pharm 19 52 2731 HARI KRISHNAN P 186.00 MBC/DNC B.Pharm 20 56 1416 THAMIL SELVAN R 186.00 BC B.Pharm 21 58 6663 SNEKA S 185.75 BC B.Sc. -

Pg Degree/Diploma Courses 2017 - 2018 Session - on 24.05.2017 List of Candidates Relieved From
PG DEGREE/DIPLOMA COURSES 2017 - 2018 SESSION - ON 24.05.2017 LIST OF CANDIDATES RELIEVED FROM NAME OF THE INSTITUTION : CHENGALPATTU MEDICAL COLLEGE, CHENGALPATTU COMMUNI SERVICE TOTAL ALLOTTED TO PREVIOUS RELIEVED SNO RANK AR.NO NAME TY STATUS MARKS SPECIALITY DATE CURRENT SPECIALITY CURRENT COLLEGE 1 74 52537 Dr.CHILAMBARASAN V BC SERV 1301.945320 M.D. Paediatrics THANJAVUR MEDICAL M.D. Paediatrics COLLEGE, THANJAVUR 2 82 53545 Dr.VEERAMANI C BC SERV 1295.744320 M.D. General GOVT. MOHAN M.D. Paediatrics Medicine KUMARAMANGALAM MEDICAL 3 119 53262 Dr.B PRIYANKA OC SERV 1273.930680 M.S. Obstetrics MADRAS MEDICAL COLLEGE, M.S. Obstetrics and and Gynaecology CHENNAI Gynaecology 4 158 51494 Dr.ISHWARYA R OC SERV 1245.083280 M.D. General KILPAUK MEDICAL COLLEGE M.D. General Medicine , CHENNAI Medicine 5 253 53623 Dr.SIDDHARTHAN R BC SERV 1208.677920 M.D. General CHENGALPATTU MEDICAL M.S. General Medicine COLLEGE, CHENGALPATTU Surgery 6 264 53620 Dr.L LALITHKUMAR BC SERV 1204.666450 M.S. General STANLEY MEDICAL COLLEGE M.S. General Surgery , CHENNAI Surgery 7 281 54539 Dr.KALAIYARASI BC SERV 1198.640640 M.S. Obstetrics GOVT. MOHAN M.S. Obstetrics and and Gynaecology KUMARAMANGALAM MEDICAL Gynaecology 8 369 52105 Dr.NIRMAL THEJRAJ OC SERV 1167.247510 M.D. MADRAS MEDICAL COLLEGE, M.D. Anaesthesiology CHENNAI Anaesthesiology 9 388 53137 Dr.SENTHIL RAJA V MBC/DNC SERV 1163.340490 M.S. General THANJAVUR MEDICAL M.S. General Surgery COLLEGE, THANJAVUR Surgery 10 429 51471 Dr.THENDRALARASI R BC SERV 1153.893780 M.D. STANLEY MEDICAL COLLEGE M.D. -

COVID-19 Testing Labs
भारतीय आयु셍वज्ञि ान अनुसधं ान पररषद वा्य अनुसंधान 셍वभाग, वा्य और पररवार क쥍याण मंत्रालय, भारत सरकार Date: 20/05/2020 Total Operational (initiated independent testing) Laboratories reporting to ICMR: Government laboratories : 396 Private laboratories : 173 - Real-Time RT PCR for COVID-19 : 437 (Govt: 294 + Private: 143) - TrueNat Test for COVID-19 : 81 (Govt: 76 + Private: 05) - CBNAAT Test for COVID-19 : 51 (Govt: 26 + Private: 25) Total No. of Labs : 569 *CSIR/DBT/DST/DAE/ICAR/DRDO Laboratories. #Laboratories approved for both Real-Time RT-PCR and TrueNat/CBNAAT $Laboratories approved for both TrueNAT and CBNAAT S. Names of Test Names of Government Institutes Names of Private Institutes No. States Category 1. Andhra RT-PCR 1. Sri Venkateswara Institute of Medical Pradesh (52) Sciences, Tirupati 2. Sri Venkateswara Medical College, Tirupati 1 | P a g e भारतीय आयु셍वज्ञि ान अनुसधं ान पररषद वा्य अनुसंधान 셍वभाग, वा्य और पररवार क쥍याण मंत्रालय, भारत सरकार S. Names of Test Names of Government Institutes Names of Private Institutes No. States Category 3. Rangaraya Medical College, Kakinada 4. #Sidhartha Medical College, Vijaywada 5. Govt. Medical College, Ananthpur 6. Guntur Medical College, Guntur 7. Rajiv Gandhi Institute of Medical Sciences, Kadapa 8. Andhra Medical College, Visakhapatnam 9. Govt. Kurnool Medical College, Kurnool 10. Govt. Medical College, Srikakulam TrueNat 11. Damien TB Research Centre, Nellore 12. SVRR Govt. General Hospital, Tirupati 13. Community Health Centre, Gadi Veedhi Saluru, Vizianagaram 14. Community Health Centre, Bhimavaram, West Godavari District 15. -

GOVERNMENT COLLEGES the TAMIL NADU Dr. M.G.R. Medical
THE TAMIL NADU Dr. M.G.R. Medical University, Chennai M.B.B.S. Affiliated Colleges/Institutions for the Academic Year 2020‐21 GOVERNMENT COLLEGES Sl.No. Inst. Code Name of the Institution Sanctioned Intake 1 006 Chengalpattu Medical College, Chengalpattu 100 2 007 Coimbatore Medical College, Coimbatore 150 3 495 Esic Medical College, Chennai 100 4 244 Government Dharmapuri Medical College, Dharmapuri 100 5 013 Government Erode Medical College & Hospital, Perundurai 100 6 656 Government Medical College & Esic Hospital, Coimbatore 100 7 638 Government Medical College Omandurar, Chennai 100 8 673 Government Medical College Pudukkottai 150 9 400 Government Medical College Thiruvarur 100 10 773 Government Medical College, Karur 150 11 399 Government Medical College,Villupuram 100 12 010 Government Mohan Kumaramangalam Medical College, Salem 100 13 572 Government Sivagangai Medical College,Sivagangai 100 14 240 Government Theni Medical College, Theni 100 15 221 Government Vellore Medical College, Vellore 100 16 134 K A P Viswanatham Government Medical College,Trichy 150 17 087 Kanyakumari Government Medical College, Kanyakumari 150 18 004 Kilpauk Medical College, Chennai 150 19 001 Madras Medical College, Chennai 250 20 003 Madurai Medical College, Madurai 250 21 002 Stanley Medical College, Chennai 250 22 005 Thanjavur Medical College, Thanjavur 150 23 603 Thiruvannamalai Government Medical College & Hospital, Thiruvannamalai 100 24 160 Thoothukudi Government Medical College,Thoothukudi 150 25 008 Tirunelveli Medical College, Tirunelveli 250 -

S.No College Name 1 Madras Medical College 2 Stanley Medical College
S.no College Name 1 Madras Medical College 2 Stanley Medical College 3 Madurai Medical College 4 Thanjavur Medical College 5 Kilpauk Medical College 6 Chengalpet Medical College 7 Tirunelveli Medical College 8 Coimbatore Medical College 9 Govt. Mohan Kumaramangalam Medical college 10 Govt. K.A.P. Viswanathan Medical College Tiruchi 11 Thoothukudi Medical College 12 Kanyakumari Medical College 13 Vellore Medical College 14 Theni Medical College 15 Dharmapuri Govt. Medical College 16 Villupuram Govt. Medical College 17 Sivagangai Govt. Medical College 18 Thiruvarur Govt. Medical College 19 Karpagam Faculty of Medical Sciences & Research 20 Christian Medical College (CMC), Vellore 21 IRT Perundurai Medical college PSG Institute of Medical Sciences 22 and Research Coimbatore Sree Moogambigai Medical College, Kulasekharam 23 Adiparasakthi Institute of Medical Sciences, Melmaruvatur 24 25 Tagore Medical College Chennai 26 Annapoorna Medical college, Salem 27 Chennai Medical College (SRM), Trichy KarpagaVinayagam Medical College, Madhuranthagam 28 Dhanalakshmi Srinivasan Medical College Perambalur 29 Sree Muthukumaran Medical College, Chennai 30 31 Madha Medical college Chennai Rajah Muthiah Medical College, Annamalai Nagar – 32 Annamalai University Sree Balaji Medical College & Hospital, Chennai – 33 Bharath University ACS Medical College & Hospital, Chennai – Dr MGR 34 Educational & Research Institute (University). Meenakshi Medical College & Research Institute, 35 Kancheepuram – Meenakshi University. Saveetha Medical College & Hospital – Kanchipuram -

Sno Rank Ar No Name Community Service Total Marks Speciality College
POST GRADUATE MEDICAL (GOVERNMENT QUOTA) 2020-2021 SESSION RESULT OF FIRST PHASE COUNSELLING ON 08-05-2020 SNO RANK AR_NO NAME COMMUNITY SERVICE TOTAL SPECIALITY COLLEGE MARKS 1 1 5709 Dr. BHUVANANDHINI K BC Service 1035.05 M.D. D.V.L MADRAS MEDICAL COLLEGE, CHENNAI 2 2 5272 Dr. SHIVA A MBC/DNC Service 1002.3 M.D. Radio Diagnosis MADRAS MEDICAL COLLEGE, CHENNAI 3 3 4624 Dr. B KIRUBAKARAN BC Service 991.2 M.D. Radio Diagnosis MADRAS MEDICAL COLLEGE, CHENNAI 4 5 3713 Dr. SIDDHARTH P BC Service 940 M.D. Radio Diagnosis COIMBATORE MEDICAL COLLEGE, COIMBATORE 5 6 3634 Dr. LENINPRABHU P MBC/DNC Service 934.72 M.D. Radio Diagnosis STANLEY MEDICAL COLLEGE , CHENNAI 6 7 4294 Dr. ELANGO M MBC/DNC Service 931.5 M.D. D.V.L STANLEY MEDICAL COLLEGE , CHENNAI 7 9 6403 Dr. RAGAVI MBC/DNC Service 930.91 M.D. Radio Diagnosis STANLEY MEDICAL COLLEGE , CHENNAI 8 10 5180 Dr. SHYAMALA M BC Service 930.35 M.D. Radio Diagnosis STANLEY MEDICAL COLLEGE , CHENNAI 9 16 5772 Dr. ANTONY SHERLY ROSE M BC Service 918.21 M.D. General Medicine MADURAI MEDICAL COLLEGE, MADURAI 10 17 5323 Dr. C ADITHYAN BC Service 914.4 M.D. General Medicine MADRAS MEDICAL COLLEGE, CHENNAI 11 18 5887 Dr. SHIVA N K BC Service 913.9 M.D. General Medicine COIMBATORE MEDICAL COLLEGE, COIMBATORE 12 20 5650 Dr. VASANTHAKUMAR S BC Service 908.4 M.D. Radio Diagnosis MADRAS MEDICAL COLLEGE, CHENNAI 13 21 1425 Dr. VINOTH KUMAR S BC Service 906.78 M.D. -

Mbbs - 2020 - 2021 Session Vacancy Position in Government Colleges, As on 11/01/2021 11:52:01 Am
MBBS - 2020 - 2021 SESSION VACANCY POSITION IN GOVERNMENT COLLEGES, AS ON 11/01/2021 11:52:01 AM COLLEGE OC BC BCM MBC SC SCA ST TOTAL MADRAS MEDICAL COLLEGE, CHENNAI. STANLEY MEDICAL COLLEGE, CHENNAI. KILPAUK MEDICAL COLLEGE, CHENNAI. MADURAI MEDICAL COLLEGE, MADURAI. THANJAVUR MEDICAL COLLEGE, THANJAVUR. CHENGALPATTU MEDICAL COLLEGE, CHENGALPATTU. TIRUNELVELI MEDICAL COLLEGE, TIRUNELVELI. COIMBATORE MEDICAL COLLEGE, COIMBATORE. GOVT. MOHAN KUMARAMANGALAM MEDICAL COLLEGE, SALEM. GOVT. K.A.P.V MEDICAL COLLEGE, TRICHY. THOOTHUKUDI MEDICAL COLLEGE, THOOTHUKUDI. KANYAKUMARI MEDICAL COLLEGE, KANYAKUMARI. VELLORE MEDICAL COLLEGE, VELLORE. THENI MEDICAL COLLEGE, THENI. Page 1 of 2 MBBS - 2020 - 2021 SESSION VACANCY POSITION IN GOVERNMENT COLLEGES, AS ON 11/01/2021 11:52:01 AM COLLEGE OC BC BCM MBC SC SCA ST TOTAL DHARMAPURI MEDICAL COLLEGE, DHARMAPURI. VILLUPURAM MEDICAL COLLEGE, VILLUPURAM. THIRUVARUR MEDICAL COLLEGE, THIRUVARUR. SIVAGANGAI MEDICAL COLLEGE, SIVAGANGAI. TIRUVANNAMALAI MEDICAL COLLEGE, TIRUVANNAMALAI. GOVT. MEDICAL COLLEGE, OMANDURAR ESTATE,CHENNAI GOVT.MEDICAL COLLEGE,ESIC HOSPITAL, COIMBATORE. GOVT. KARUR MEDICAL COLLEGE, KARUR GOVT.MEDICAL COLLEGE & HOSPITAL,PUDUKOTTAI ESIC MEDICAL COLLEGE, K.K. NAGAR, CHENNAI. RAJAH MUTHIAH MEDICAL COLLEGE & HOSPITAL (ANNAMALAI UNIV.) GOVERNMENT ERODE MEDICAL COLLEGE AND HOSPITAL,PERUNDURAI TOTAL Page 2 of 2 MBBS - 2020 - 2021 SESSION VACANCY POSITION IN SELF FINANCING COLLEGES, AS ON 11/01/2021 11:52:09 AM COLLEGE OC BC BCM MBC SC SCA ST TOTAL PSG INSTITUTE OF MEDICAL SCIENCES , COIMBATORE. SREE MOOGAMBIGAI INSTITUTE OF MEDICAL SCIENCES, KANYAKUMARI KARPAGA VINAYAKA INSTITUTE OF MEDICAL SCIENCES VELAMMAL MEDICAL COLLEGE HOSPITAL & RESEARCH INSTITUTE , MADURAI TRICHY(SRM) MEDICAL COLLEGE , HOSPITAL & RESEARCH CENTRE, TRICHY TAGORE MEDICAL COLLEGE & HOSPITAL, CHENNAI DHANALAKSHMI SRINIVASAN MEDICAL COLLEGE & HOSPITAL , PERAMBALUR MELMARUVATHUR ADHIPARASAKTHI INSTITUTE OF MEDICAL SCIENCES & RESEARCH, KANCHEEPURAM KARPAGAM FACULTY OF MEDICAL SCIENCES & RESEARCH, COIMBATORE. -

“Comparison of Nalbuphine with 0.125% Bupivacaine and Plain 0.125% Bupivacaine in Thoracic Epidural for Post Operative Analge
“COMPARISON OF NALBUPHINE WITH 0.125% BUPIVACAINE AND PLAIN 0.125% BUPIVACAINE IN THORACIC EPIDURAL FOR POST OPERATIVE ANALGESIA IN UPPER ABDOMINAL SURGERY” Dissertation Submitted in Partial fulfilment of the University regulations for M.D. DEGREE EXAMINATION -MAY 2019 MD DEGREE IN ANAESTHESIOLOGY (BRANCH X) GOVERNMENT THENI MEDICAL COLLEGE, THENI THE TAMIL NADU DR. M.G.R. MEDICAL UNIVERSITY CHENNAI, TAMILNADU CERTIFICATE This is to certify that the dissertation titled “Comparison Of Nalbuphine With 0.125% Bupivacaine And Plain 0.125% Bupivacaine In Thoracic Epidural For Post Operative Analgesia In Upper Abdominal Surgery” is a Bonafide original work done by DR.M.SUBHASHINI during May 2016-May 2019 in partial fulfilment of the requirements for M.D. (Anaesthesiology) Branch X- Examination of the Tamilnadu Dr.M.G.R. Medical University to be held in May 2019. Prof. DR.S.VIJAYA, Prof. DR.S.VIJAYARAGAVAN, M.D., M.D., D.A., Professor and Guide, Professor and HOD, Department of Anaesthesiology, Department of Anaesthesiology, Govt. Theni Medical College, Govt. Theni Medical College, Theni. Theni. Prof. DR.K.RAJENDRAN, M.S.,D.Ortho., Dean, Govt. Theni Medical College, Theni. DECLARATION I DR.M.SUBHASHINI solemnly declare that this dissertation, titled “Comparison Of Nalbuphine With 0.125% Bupivacaine And Plain 0.125% Bupivacaine In Thoracic Epidural For Post Operative Analgesia In Upper Abdominal Surgery” is a Bonafide record of work done by me in the Department of Anaesthesiology, Govt. Theni Medical College and Hospital, Theni under the guidance of Prof. DR.S.VIJAYA, M.D., Professor of Anaesthesiology, Govt. Theni Medical College & Hospital, Theni.