Ablation for Pancreatic Carcinoma Changing the Paradigm of Treatment Options for One of the Most Lethal Cancers
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Interventional Radiology in the Diagnosis and Treatment of Solid Tumors
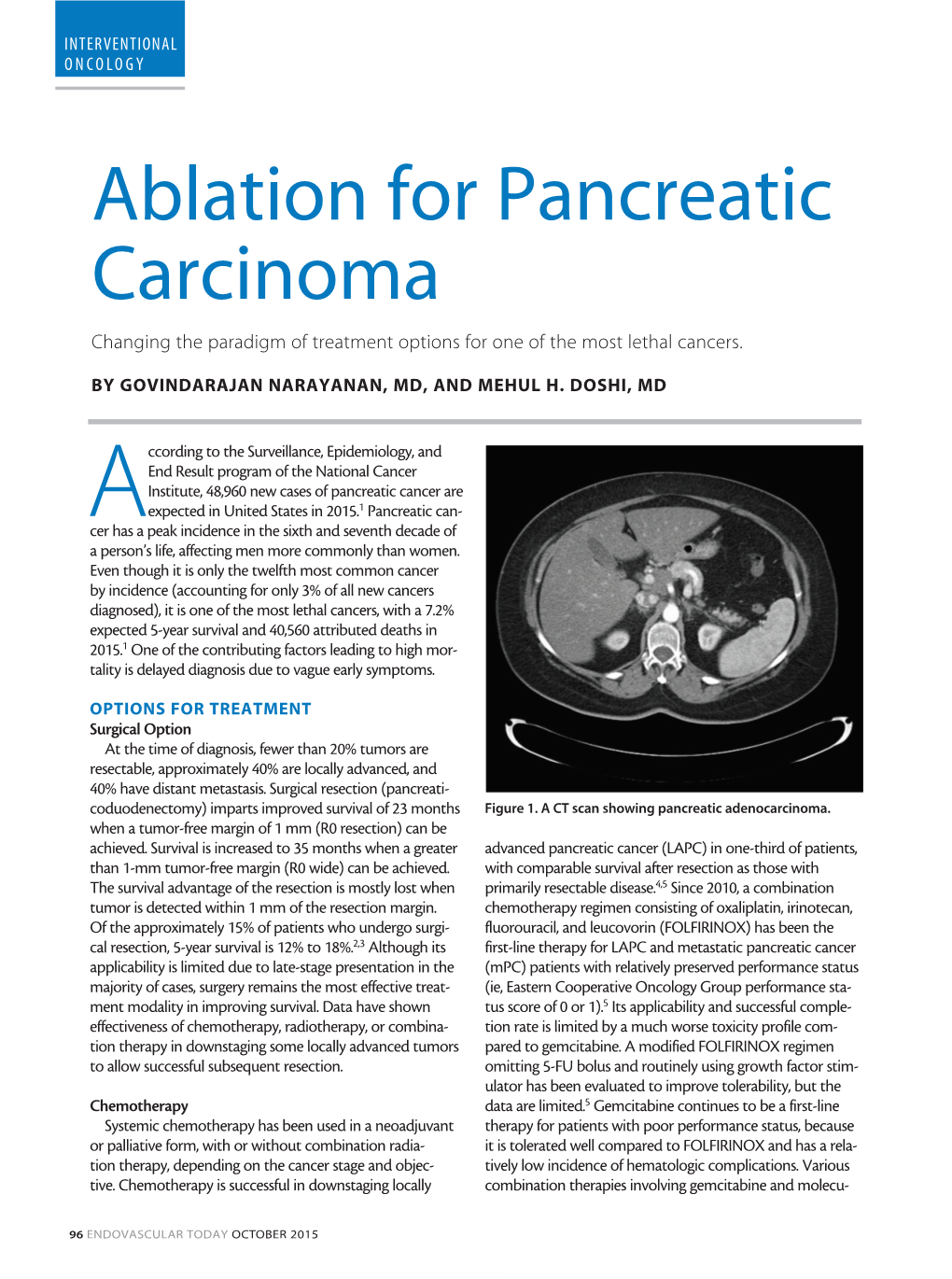
THE ROLE OF INTERVENTIONAL RADIOLOGY IN THE DIAGNOSIS AND TREATMENT OF SOLID TUMORS Victoria L. Anderson, MSN, CRNP, FAANP OBJECTIVES •Using Case Studies and Imaging examples: 1) Discuss the role interventional (IR) procedures to aid in diagnosing malignancy 2) Current and emerging techniques employed in IR to cure and palliate solid tumor malignancies will be explored Within 1 and 2 will be a discussion of research in the field of IR Q+A NIH Center for Interventional Oncology WHAT IS INTERVENTIONAL RADIOLOGY? • Considered once a subspecialty of Diagnostic Radiology • Now its own discipline, it serves to offer minimally invasive procedures using state-of- the-art modern medical advances that often replace open surgery (Society of Interventional Radiology) NIH Center for Interventional Oncology CHARLES T. DOTTER M.D. (1920-1985) • Father of Interventional Radiologist • Pioneer in the Field of Minimally Invasive Procedures (Catheterization) • Developed Continuous X-Ray Angio- Cardiography • Performed First If a plumber can do it to pipes, we can do it to blood vessels.” Angioplasty (PTCA) Charles T. Dotter M.D. Procedure in 1964. • Treated the first THE ROOTS OF patient with catheter assisted vascular INTERVENTIONAL dilation RADIOLOGY NIH Center for Interventional Oncology THE “DO NOT FIX” CONSULT THE DO NOT FIX PATIENT SCALES MOUNT HOOD WITH DR. DOTTER 1965 NIH Center for Interventional Oncology •FIRST EMBOLIZATION FOR GI BLEEDING •ALLIANCE WITH •FIRST BALLOON BILL COOK •HIGH SPEED PERIPHERAL DEVELOPED RADIOGRAPHY ANGIOPLASTY-- NUMEROUS -

Is Interventional Oncology Ready to Stand on Its Own? Interventional Oncology Sets Aim on Becoming the Fourth Pillar in the Treatment of Cancer
INTERVENTIONAL ONCOLOGY Point/Counterpoint: Is Interventional Oncology Ready to Stand on Its Own? Interventional oncology sets aim on becoming the fourth pillar in the treatment of cancer. Yes, it is! LEADING GROWTH IN IR FOR 20 YEARS The economic engine of IR for the past 2 decades has BY MICHAEL C. SOULEN, MD, FSIR, FCIRSE been IO, outstripping growth in other vascular and non- vascular IR disciplines. Furthermore, IO procedures have have been practicing interventional oncology (IO) for higher revenue per relative value unit than vascular inter- almost 25 years (most interventional radiologists prob- ventions, so a full-time equivalent in IO is more valuable ably have to a greater or lesser extent). The treatment of than one focusing on arterial diseases. IO is also a driver cancer by interventional radiologists dates back to the of growth for industry—interventional oncologists I1950s, even before interventional radiology (IR) was rec- consume 10 times more product than interventional ognized as a discipline.1 Our “founding fathers” published radiologists from the same group who do not have an extensively on minimally invasive, image-guided cancer oncologic practice (Figure 1). IO is spurring the surge of therapy through the 1960s and ‘70s.2-4 Tumor emboliza- interest in IR among medical students and residents. tion has been a standard of care for 3 decades, and tumor ablation has been common practice for the past 15 years. A Fortuitous Convergence Palliative procedures for management of cancer-related The evolution of IO from “something we do” into a obstruction, pain management, and provision of enteral full clinical discipline was born from the convergence of and venous access are routine IR practice. -

Ablation in Pancreatic Cancer: Past, Present and Future
cancers Review Ablation in Pancreatic Cancer: Past, Present and Future Govindarajan Narayanan 1,2,3,*, Dania Daye 4, Nicole M. Wilson 3, Raihan Noman 3, Ashwin M. Mahendra 5 and Mehul H. Doshi 6,7 1 Miami Cancer Institute, Baptist Health South Florida, Miami, FL 33176, USA 2 Miami Cardiac and Vascular, Baptist Health South Florida, Miami, FL 33176, USA 3 Herbert Wertheim College of Medicine, Florida International University, Miami, FL 33199, USA; nwils027@med.fiu.edu (N.M.W.); rnoma001@med.fiu.edu (R.N.) 4 Division of Vascular and Interventional Radiology, Department of Radiology, Massachusetts General Hospital, Harvard Medical School, Harvard University, Boston, MA 02114, USA; [email protected] 5 Pratt School of Engineering, Duke University, Durham, NC 27708, USA; [email protected] 6 Department of Radiology, Cleveland Clinic Florida, Weston, FL 33331, USA; [email protected] 7 Charles E. Schmidt College of Medicine, Florida Atlantic University, Boca Raton, FL 33431, USA * Correspondence: [email protected] Simple Summary: Despite advancements in surgical oncology and chemoradiation therapies, pancre- atic cancer still has one of the lowest 5-year survival rates in the United States. The silent progression of this disease often leads to it being identified after it has already reached an advanced and often unresectable stage. The field of interventional oncology has yielded ablation strategies with the potential to downstage and increase survival rates in patients suffering from locally advanced pan- creatic cancer. This review examines the treatment strategies for locally advanced pancreatic cancer, discussing current results and future directions. Citation: Narayanan, G.; Daye, D.; Abstract: The insidious onset and aggressive nature of pancreatic cancer contributes to the poor Wilson, N.M.; Noman, R.; Mahendra, treatment response and high mortality of this devastating disease. -

Technical Update on Transcatheter Arterial Chemoembolization
Puppala. Hepatoma Res 2019;5:44 Hepatoma Research DOI: 10.20517/2394-5079.2019.28 Review Open Access Technical update on transcatheter arterial chemoembolization Sapna Puppala Department of Radiology, Leeds Teaching Hospital, Leeds LS1 3EX, UK. Correspondence to: Dr. Sapna Puppala, Consultant vascular interventional radiologist, Leeds Teaching Hospital NHS Trust, Great George street Leeds, Leeds LS1 3EX, UK. E-mail: [email protected] How to cite this article: Puppala S. Technical update on transcatheter arterial chemoembolization. Hepatoma Res 2019;5:44. http://dx.doi.org/10.20517/2394-5079.2019.28 Received: 5 Nov 2019 First Decision: 2 Dec 2019 Revised: 12 Dec 2019 Accepted: 16 Dec 2019 Published: 31 Dec 2019 Science Editor: Dalbir Sandhu Copy Editor: Jing-Wen Zhang Production Editor: Jing Yu Abstract Transcatheter arterial chemoembolization has become an established drug delivery system for palliative or bridging Received: First Decision: Revised: Accepted: Published: treatment of hepatocellular carcinoma. Over the last two decades, various research and developments have taken place to improve the transcatheter arterial chemoembolization procedure from both a clinical and a technical Science Editor: Copy Editor: Production Editor: Jing Yu perspective. This review article aims to provide an update on the technical developments over the last decade. Keywords: Transcatheter arterial chemoembolization, Doxorubicin, bead, cisplatin INTRODUCTION Since its first introduction in the late 1970s, transcatheter arterial chemoembolization (TACE) has become an established drug delivery system for palliative or bridging treatment of hepatocellular carcinoma (HCC)[1,2]. Randomized controlled trials have shown a survival benefit in patients treated with TACE, compared to transcatheter arterial embolization (TAE) using bland agents with no additional chemotherapy[3-5]. -

Interventional Oncology
Kidney Cancer: Renal Cell Carcinoma Cancer that arises in the kidneys comes from either Interventional the functional tissue of the kidney or from the lining and Vascular Interventional of the collecting system. Renal cell carcinoma (RCC) arises from the functional tissue of the kidney and is far Consultants Oncology more common than the other types of kidney cancer. Frequently, RCC is found incidentally on imaging for other reasons. Interventional and Vascular Consultants is a comprehensive medical practice specializing in minimally invasive endovascular solutions to diagnose and treat diseases of the blood vessels. Our unique approach to vascular care is recognized for its commitment to clinical excellence and outstanding patient satisfaction. The minimally invasive techniques used by interventional radiologists often replace open surgical procedures because there are no large incisions, less risk, reduced pain, and shorter recovery times for patients. Our state-of-the-art endovascular suites are equipped with the newest devices to assist in performing minimally invasive procedures. Stage I RCC (measuring less than 7 cm in diameter) can potentially be cured with minimally invasive How to make an appointment: treatments such as percutaneous ablation with or without transcatheter embolization. This treatment Physician Referrals largely avoids the added risk of open surgical procedures Call or fax a request to our office. Please include any and is the treatment most likely to preserve the most pertinent X-rays, labs and chart notes you have. These kidney function. will be reviewed and a consultation appointment will be scheduled with your patient. We can provide your Treatment Options office with referral forms as well. -

In Interventional Oncology for Liver Cancer: How to Reduce the Risk for Complications?
life Review “Primum Non Nocere” in Interventional Oncology for Liver Cancer: How to Reduce the Risk for Complications? Roberto Iezzi 1,* , Tiago Bilhim 2 , Laura Crocetti 3, Bora Peynircioglu 4 , Shraga Goldberg 5,6, Josè Ignacio Bilbao 7, Ahmed Sami 8, Okan Akhan 4, Paola Scalise 3, Felice Giuliante 9, Maurizio Pompili 10, Vincenzo Valentini 11, Antonio Gasbarrini 10, Cesare Colosimo 1 and Riccardo Manfredi 1 1 Dipartimento di Diagnostica per Immagini, Radioterapia Oncologica ed Ematologia, Fondazione Policlinico Universitario A. Gemelli-IRCCS, Università Cattolica del Sacro Cuore, L.go A. Gemelli 8, 00168 Rome, Italy; [email protected] (C.C.); [email protected] (R.M.) 2 Nova Medical School, Interventional Radiology Unit, Saint Louis Hospital and Curry Cabral Hospital, Centro Hospitalar Universitário de Lisboa (CHULC), 1069-166 Lisbon, Portugal; [email protected] 3 Division of Interventional Radiology, Department of Diagnostic and Interventional Radiology and Nuclear Medicine, Cisanello University Hospital, 56126 Pisa, Italy; [email protected] (L.C.); [email protected] (P.S.) 4 Department of Radiology, Faculty of Medicine, Hacettepe University, 06100 Ankara, Turkey; [email protected] (B.P.); [email protected] (O.A.) 5 Image-Guided Therapy and Interventional Oncology Unit, Department of Radiology, Hadassah Hebrew University Medical Center Ein Karem, 91120 Jerusalem, Israel; [email protected] 6 Minimally Invasive Tumor Therapy Laboratory Section of Interventional Radiology, Department of Radiology Beth Israel Deaconess Medical Center/Harvard Medical School, 330 Brookline Ave Boston, Boston, MA 02215, USA 7 Department of Radiology, Clínica Universidad de Navarra, Avenida Pio XII, no. 36, 31008 Pamplona, Spain; [email protected] 8 Department of Radiology, Cairo University, Cairo 12613, Egypt; [email protected] 9 Hepatobiliary Surgery Unit, Fondazione Policlinico Universitario A. -

WHAT IS the FUTURE of INTERVENTIONAL ONCOLOGY? Interventional Radiologists Discuss Current and Future Needs to Make IR the Next Pillar in Cancer Treatment
Supplement to Sponsored by Boston Scientific Corporation September 2016 WHAT IS THE FUTURE OF INTERVENTIONAL ONCOLOGY? Interventional radiologists discuss current and future needs to make IR the next pillar in cancer treatment. Theresa Jin-Wook Ryan Kelvin Edward Caridi, MD Chung, MD Hickey, MD Hong, MD Kim, MD Edward David Sam Manfred Sarah Wolfgang Lee, MD Liu, MD Mouli, MD Spanger, MD White, MD DIREXION™ Torqueable Microcatheter REPOSITION WITHOUT THE WIRE With best-in-class torque and four tip shape options, the Direxion Microcatheter allows you to re-position the distal tip without a guidewire and facilitate navigation to additional treatment sites. DIREXION™ DIREXION HI-FLO™ CAUTION: Federal law (USA) restricts this device to sale by or on the order of a physician. Rx only. Prior to use, please see the complete “Directions for Use” for more information on Indications, Contraindications, Warnings, Precautions, Adverse Events, and Operator’s Instructions. INTENDED USE/INDICATIONS FOR USE: The Direxion and Direxion HI-FLO Torqueable Microcatheters are intended for peripheral vascular use. The pre-loaded Fathom and Transend Guidewires can be used to selectively introduce and position the microcatheter in the peripheral vasculature. The microcatheter can be used for controlled and selective infusion of diagnostic, embolic, or therapeutic materials into the vessel. CONTRAINDICATIONS: None known. WARNINGS: • Never advance or withdraw an intravascular device against resistance until the cause of resistance is determined by fl uoroscopy. Movement of the microcatheter or guidewire against resistance may result in damage or separation of the microcatheter or guidewire tip, or vessel perforation. • This Direxion Microcatheter family is not intended for use in the coronary vasculature or neurovasculature. -

Submitted By: Jack Jennings, MD, Phd, Associate Professor
Submitted by: Jack Jennings, MD, PhD, Associate Professor, Washington University Sean Tutton, MD, FSIR, Professor of Radiology, Medical College of Wisconsin Anil Nick Kurup, MD, Radiologist, Mayo Clinic Organization: Society of Interventional Oncology 2025 M St NW #800, Washington, DC 20036 Phone: (202) 367-1164 Email: [email protected] September 16, 2019 NCCN Guidelines Panel: Adult Cancer Pain On behalf of the Society of Interventional Oncology, we respectfully request the NCCN Adult Cancer Pain Guideline panel review the enclosed data for inclusion in the management of adult cancer pain. Specific Change 1: Pain-D 20/99 Regarding local bone pain, consider local RT, nerve block….vertebral augmentation, or percutaneous thermal ablation (e.g. radiofrequency ablation, cryoablation, microwave, MR guided high intensity frequency ultrasound) or just percutaneous ablation replacing radiofrequency ablation. References: • Callstrom MR, Dupuy DE, Solomon SB, et al. Percutaneous image-guided cryoablation of painful metastases involving bone: multicenter trial. Cancer 2013;119:1033–1041 22. • Wallace AN ,McWilliams SR, Connolly SE, et al. Percutaneous Image-Guided Cryoablation of Musculoskeletal Metastases: Pain Palliation and Local Tumor Control. J Vasc Interv Radiol.2016 ;27(12):1788-1796. • Anchala PR, Irving WD, Hillen TJ, et al. Treatment of Metastatic Spinal Lesions with a Navigational Bipolar Radiofrequency Ablation Device: A Multicenter Retrospective Study. Pain Physician. 2014;17:317–27 • Bagla S, Sayed D, Smirniotopoulos J, et al. Multicenter Prospective Clinical Series Evaluating Radiofrequency Ablation in the Treatment of Painful Spine Metastases. Cardiovasc Intervent Radiol. 2016;39(9):1289-97. • Deib G, Deldar B, Hui F, Barr JS, Khan MA. Percutaneous Microwave Ablation and Cementoplasty: Clinical Utility in the Treatment of Painful Extraspinal Osseous Metastatic Disease and Myeloma. -
Interventional Oncology: a Key Part of Mainstream Cancer Care
Published online: 2021-03-26 Editorial Interventional Oncology: A Key Part of Mainstream Cancer Care Thank you very much indeed for that generous introduction. chest. After the operation, he developed a fistula between I am grateful to the organizing committee for including me the stomach and the right main bronchus and his life was in the excellent program for this meeting. I shall talk to miserable because every time he had anything to eat or drink you about interventional oncology this afternoon and why some of the food or drink went into the lungs, which is I consider it to be an important part of modern cancer care. why you are looking at bilateral pneumonia. It would have However before that, I thought you might be interested in been difficult to deal with this surgically in a frail patient, a few remarks on the names and locations of some London but it was straightforward to sort it out radiologically. We hospitals: I work at St. Thomas’s, which is opposite Big introduced a self-expanding stent covered with plastic, Ben on the south bank of the Thames. However, was which sealed the fistula quite effectively. An esophagogram not always there: until the mid-1800s, it was a couple of demonstrated flow in the remnant of the esophagus and miles away, in the London borough of Southwark, in St. into the small bowel without any of the contrast medium Thomas’s Street. However, the hospital currently of St. entering the lungs. This procedure transformed the patient’s Thomas’s street is Guy’s Hospital. -
Safety and Efficacy of Cryoablation of Renal Tumors in a High‑Risk Patient Population at a Community Hospital
Published online: 2021-03-26 Original Article Safety and Efficacy of Cryoablation of Renal Tumors in a High‑Risk Patient Population at a Community Hospital Abstract Martin Oselkin1,2, Purpose: The purpose of the study was to evaluate the safety and efficacy of percutaneous Nathan Cornish1, cryoablation for the treatment of renal masses in a high surgical risk population stratified by Peter Homel3, Charlson Comorbidity Index treated at a community hospital and to determine parameters associated 1,4 with higher complication rates. Materials and Methods: A retrospective chart review of patients Shaun Honig , 5 with renal masses treated with image-guided percutaneous cryoablation between 2007 and 2013 David Silver , was performed. Results: A total of 121 tumors were ablated in 105 patients. The mean patient age Sergei Sobolevsky1,6 was 70 years old. Comorbidities included morbid obesity, hypertension, diabetes mellitus, coronary Departments of 1Radiology and artery disease, pulmonary disease, cigarette use, and renal insufficiency. Mean tumor size treated 5Urology, Maimonides Medical was 3.15 cm in largest diameter, ranging from 1.4 to 6.5 cm. Complications were observed in Center, Brooklyn, 2Department 16 cases. The most common complication was perinephric and/or pararenal hemorrhage. Procedures of Radiology‑Neuroradiology, with >3.5 probes, hemoglobin >12.5 g/dl, tumor size >3.55 cm, and age >75 years were all St. Luke’s University Hospital, 3 associated with greater likelihood of complications. Conclusions: Our experience with percutaneous Bethlehem, PA, Department of Medicine, Albert Einstein cryoablation of small renal masses offers similar results in efficacy to published data in patients with College of Medicine, Bronx, significant comorbidities. -
Interventional Oncology in the Management of Metastatic Colorectal Cancer
Interventional Oncology in the Management of Metastatic Colorectal Cancer Citation for published version (APA): Kurilova, I. (2020). Interventional Oncology in the Management of Metastatic Colorectal Cancer. Gildeprint en Universitaire Pers Maastricht. https://doi.org/10.26481/dis.20200707ik Document status and date: Published: 01/01/2020 DOI: 10.26481/dis.20200707ik Document Version: Publisher's PDF, also known as Version of record Please check the document version of this publication: • A submitted manuscript is the version of the article upon submission and before peer-review. There can be important differences between the submitted version and the official published version of record. People interested in the research are advised to contact the author for the final version of the publication, or visit the DOI to the publisher's website. • The final author version and the galley proof are versions of the publication after peer review. • The final published version features the final layout of the paper including the volume, issue and page numbers. Link to publication General rights Copyright and moral rights for the publications made accessible in the public portal are retained by the authors and/or other copyright owners and it is a condition of accessing publications that users recognise and abide by the legal requirements associated with these rights. • Users may download and print one copy of any publication from the public portal for the purpose of private study or research. • You may not further distribute the material or use it for any profit-making activity or commercial gain • You may freely distribute the URL identifying the publication in the public portal. -

Douglas M. Coldwell, Ph.D., M.D. 530 S
Douglas M. Coldwell, Ph.D., M.D. 530 S. Jackson Street C07 Louisville, KY 40202 (502) 852-5875 [email protected] 01AUG2018 EDUCATION 1967-1971 B.A. Materials Science, Rice University, Houston, TX 1972-1975 Ph.D. Materials Science, Rice University, Houston, TX Dissertation: Thermodynamics of Fe-Cr-H Ternary Interstitial Solid Solutions 1980-1983 M.D. Medicine, University of Texas Medical Branch, Galveston, TX 1980-1983 Residency, Diagnostic Radiology, Pennsylvania State University, Hershey Medical Center, Hershey, PA 1983-1984 Fellowship, Interventional Radiology, University of Texas System Cancer Center, M.D. Anderson Hospital and Tumor Institute, Houston, TX ACADEMIC APPOINTMENTS 1984-1987 Assistant Professor Radiology and Medical Oncology George Washington University Washington, DC 1987-1995 Director of Interventional Radiology, Professor of Radiology University of Washington Seattle, WA 1995-1998 Director of Interventional Radiology and Chair, Radiology Denver Health Medical Ctr, Professor of Radiology and Surgery University of Colorado Denver, CO 1998-2001 Director of Interventional Radiology Professor of Radiology and Surgery University of Maryland Medical System Baltimore, MD 2001-2002 Director of Interventional Radiology Professor of Radiology Wake Forest University Medical Center Winston-Salem, NC 2002-2003 Professor Interventional Radiology Fox Chase Cancer Center Philadelphia, PA 2003-2005 Director of Interventional Radiology Professor of Radiology and Radiation Oncology University of Mississippi Medical Center Jackson,