Please Check the Program That You Are Applying For: _____ Post-Shalhevet _____ Moreshet
Total Page:16
File Type:pdf, Size:1020Kb

Load more
Recommended publications
-

Jointorah Education Revolution
the JOIN TORAH EDUCATION REVOLUTION Afikei Torah • Ahavas Torah • Ahava V'achva • Aish HaTorah of Cleveland • Aish HaTorah of Denver • Aish HaTorah of Detroit • Aish HaTorah of Jerusalem • Aish HaTorah of Mexico • Aish HaTorah of NY • Aish HaTorah of Philadelphia • Aish HaTorah of St Louis • Aish HaTorah of Thornhill • Ateres Yerushalayim • Atlanta Scholars Kollel • AZ Russian Programs • Bais Yaakov of Boston • Bais Yaakov of LA • Bar Ilan University • Batya Girls / Torah Links • Bay Shore Jewish Center Be'er Miriam • Belmont Synagogue • Beth Din • Beth Jacob • Beth Jacob Congregation • Beth Tfiloh Upper School Library • Bnei Shalom Borehamwood & • Elstree Synagogue • Boston's Jewish Community Day School • Brandywine Hills Minyan • Calabasas Shul • Camp Bnos Agudah • Chabad at the Beaches • Chabad Chabad of Montreal • Chai Center of West Bay • Chaye Congregation Ahavat Israel Chabad Impact of Torah Live Congregation Beth Jacob of Irvine • Congregation Light of Israel Congregation Derech (Ohr Samayach) Organizations that have used Etz Chaim Center for Jewish Studies Hampstead Garden Suburb Synagogue • Torah Live materials Jewish Community Day Jewish FED of Greater Atlanta / Congregation Ariel • Jewish 600 Keneseth Beth King David Linksfield Primary and High schools • King 500 Mabat • Mathilda Marks Kennedy Jewish Primary School • Me’or 400 Menorah Shul • Meor Midreshet Rachel v'Chaya 206 MTA • Naima Neve Yerushalayim • 106 Ohab Zedek • Ohr Pninim Seminary • 77 Rabbi Reisman Yarchei Kalla • Rabbi 46 Shapell's College • St. John's Wood Synagogue • The 14 Tiferes High Machon Shlomo 1 Me’or HaTorah Meor • Me'or Midreshet Rachel v'Chaya College • Naima Neve Yerushalayim • Ohab Zedek • Ohr Pninim Seminary • Rabbi Reisman Yarchei Kalla • Rabbi 2011 2014 2016 2010 2015 2013 2012 2008 2009 Shapell's College St. -

T S Form, 990-PF Return of Private Foundation
t s Form, 990-PF Return of Private Foundation OMB No 1545-0052 or Section 4947(a)(1) Nonexempt Charitable Trust Department of the Treasury Treated as a Private Foundation Internal Revenue service Note. The foundation may be able to use a copy of this return to satisfy state report! 2006 For calendar year 2006, or tax year beginning , and ending G Check all that a Initial return 0 Final return Amended return Name of identification Use the IRS foundation Employer number label. Otherwise , HE DENNIS BERMAN FAMILY FOUNDATION INC 31-1684732 print Number and street (or P O box number if mail is not delivered to street address) Room/suite Telephone number or type . 5410 EDSON LANE 220 301-816-1555 See Specific City or town, and ZIP code C If exemption application is pending , check here l_l Instructions . state, ► OCKVILLE , MD 20852-3195 D 1. Foreign organizations, check here Foreign organizations meeting 2. the 85% test, ► H Check type of organization MX Section 501(c)(3) exempt private foundation check here and attach computation = Section 4947(a)(1) nonexempt chartable trust 0 Other taxable private foundation E If private foundation status was terminated I Fair market value of all assets at end of year J Accounting method 0 Cash Accrual under section 507(b)(1)(A), check here (from Part ll, col (c), line 16) 0 Other (specify) F If the foundation is in a 60-month termination $ 5 010 7 3 9 . (Part 1, column (d) must be on cash basis) under section 507 (b)( 1 ► )( B ) , check here ► ad 1 Analysis of Revenue and Expenses ( a) Revenue and ( b) Net investment (c) Adjusted net ( d) Disbursements (The total of amounts in columns (b), (c), and (d) may not for chartable purposes necessary equal the amounts in column (a)) expenses per books income income (cash basis only) 1 Contributions , gifts, grants , etc , received 850,000 . -
2015 Do Not Enter Social Security Numbers on This Form As It May Be Made Public
l efile GRAPHIC p rint - DO NOT PROCESS I As Filed Data - I DLN: 93491315003346 OMB No 1545-0052 Form 990-PF Return of Private Foundation or Section 4947 ( a)(1) Trust Treated as Private Foundation Department of the Treasury 2015 Do not enter social security numbers on this form as it may be made public. Internal Revenue Service ► ► Information about Form 990- PF and its instructions is at www. irs.gov /form99Opf . • • ' For calendar year 2015 , or tax year beginning 01-01 - 2015 , and ending 12-31-2015 Name of foundation A Employer identification number THE EDDIE AND RACHELLE BETESH FAMILY FOUNDATION INC 13-3981963 EDDIE BETESH Number and street ( or P 0 box number if mail is not delivered to street address) BTelephone number (see instructions) C/O SARAMAX-1372 BROADWAY-FL 7 (212) 481-8550 City or town, state or province, country, and ZIP or foreign postal code C If exemption application is pending, check here ► NEW YORK, NY 10018 P G Check all that apply [Initial return [Initial return former public charity of a D 1. Foreign organizations , check here ► F-Final return F-A mended return P F-Address change F-Name change 2. Foreign organizations meeting the 85% test, check here and attach computation ► E If private foundation status was terminated H Check type of organization [Section 501( c)(3) exempt private foundation under section 507(b)(1)(A), check here ► F Section 4947( a)(1) nonexempt charitable trust Other taxable private foundation IFair market value of all assets at end ] Accounting method [Cash F-Accrual F If the foundation -

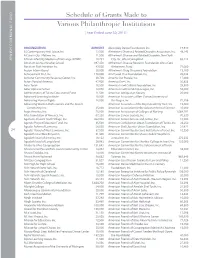
Schedule of Grants Made to Various Philanthropic Institutions
2011 ANNUAL REPORT 2011 ANNUAL Schedule of Grants Made to Grants Various Philanthropic Institutions American Folk Art Museum 127,350 American Friends of the College of American Friends of Agudat Shetile Zetim, Inc. 10,401 Management, Inc. 10,000 [ Year ended June 30, 2011 ] American Friends of Aish Hatorah - American Friends of the Hebrew University, Inc. 77,883 Western Region, Inc. 10,500 American Friends of the Israel Free Loan American Friends of Alyn Hospital, Inc. 39,046 Association, Inc. 55,860 ORGANIZATION AMOUNT All 4 Israel, Inc. 16,800 American Friends of Aram Soba 23,932 American Friends of the Israel Museum 1,053,000 13 Plus Chai, Inc. 82,950 Allen-Stevenson School 25,000 American Friends of Ateret Cohanem, Inc. 16,260 American Friends of the Israel Philharmonic 52nd Street Project, Inc. 125,000 Alley Pond Environmental Center, Inc. 50,000 American Friends of Batsheva Dance Company, Inc. 20,000 Orchestra, Inc. 320,850 A.B.C., Inc. of New Canaan 10,650 Alliance for Cancer Gene Therapy, Inc. 44,950 The American Friends of Beit Issie Shapiro, Inc. 70,910 American Friends of the Jordan River A.J. Muste Memorial Institute 15,000 Alliance for Children Foundation, Inc. 11,778 American Friends of Beit Morasha 42,360 Village Foundation 16,000 JEWISH COMMUNAL FUND JEWISH COMMUNAL Aaron Davis Hall, Inc. d/b/a Harlem Stage 125,000 Alliance for School Choice, Inc. 25,000 American Friends of Beit Orot, Inc. 44,920 American Friends of the Old City Cheder in Abingdon Theatre Company 30,000 Alliance for the Arts, Inc. -
Come and Learn
T HE R OBERT A. AND S ANDRA S. BORNS J EWISH S TUDIES P ROGRAM C OME A ND L EARN Jewish culture has long recognized the classroom as a special place—indeed a sacred place akin to the Temple. When the prophet Ezekiel spoke of a “little sanctuary” among the exiles, explains one rabbinic commentator, he was referring to houses of study. The core of the Robert A. and Sandra S. Borns Jewish Studies Program (JSP), its holy of holies as it were, is the classroom. Our faculty is at the cutting edge of humanistic and social scientific research, in fields that include anthropology, linguistics, history, A NNUAL N EWSLETTER V OLUME 23 FALL 2004 2 Indiana University literary study, philosophy, and political science. In the classroom, they introduce their students to all these approaches, helping them to come to a deeper and more complex understanding of Jewish culture and experience. While our mission is a secular one, I nonetheless think of what my colleagues and I do in the classroom, the education of our students, as a kind of sacred activity, a tremendous responsibility requiring great devotion, vigilance, and care. What gives me great confidence in our ability to fulfill this responsibility is our outstanding faculty, including long-time veterans widely recognized for their contributions to scholarship and the university, and new additions to our faculty. To focus on the latter, in 2003-2004, we welcomed Dr. Mark Roseman as the Pat M. Glazer Chair of JS. Professor Roseman is internationally recognized for his scholarship on the Holocaust and post-war Europe, and is a riveting lecturer and engaging teacher, offering important courses on the Holocaust and the history of antisemitism. -

Passion for Learning PREPARATION for LIFE
Yeshiva of Greater Washington–Tiferes Gedaliah Passion for Learning PREPARATION FOR LIFE MEET OUR MENAHEL & GS PRINCIPAL RABBI ZEV KATZ MENAHEL GIRLS DIVISION Rabbi Zev Katz has been leading YGW’s Girls Division for 35 years. His work is guided by the legacy of his uncle, Rabbi Gedaliah Anemer z”tl, as well as by his own commitment and compassion. Rabbi Katz is a master educator, with a gift for understanding each student and knowing the right thing to say at just the right time. His goal is to nurture the potential for greatness in every student, and he does so with patience, trusting that the lessons and ideas imparted between seventh and twelfth grade will bear fruit when it matters later in life. Rabbi Katz’s involvement in his students’ chinuch does not end at graduation; some of his most important work is done quietly - in phone conversations, meetings, and correspondence - years, and even decades, after graduates leave Linden Lane – for a YGW graduate remains his talmida, his responsibility, and his concern. MRS. YAEL CORTELL PRINCIPAL GENERAL STUDIES Mrs. Yael Cortell joined the YGW staff six years ago as the Principal of General Studies. She came to us from the Berman Academy where she taught Chumash and English, formally mentored new teachers, and co-chaired the English Department. Mrs. Cortell has been teaching for 18 years in a variety of schools and adult education programs, including Bais Yaakov of Baltimore, Maalot Seminary, Women’s Institute of Torah, and Mesorah Women’s Learning Institute. Mrs. Cortell has a master’s degree in Secondary English Education from Johns Hopkins University and certification in teacher mentorship and administrative leadership. -
Schedule of Grants Made to Various
Schedule of Grants Made to Various Philanthropic Institutions [ Year Ended June 30, 2015 ] ORGANIZATION AMOUNT Alvin Ailey Dance Foundation, Inc. 19,930 3S Contemporary Arts Space, Inc. 12,500 Alzheimer’s Disease & Related Disorders Association, Inc. 46,245 A Cure in Our Lifetime, Inc. 11,500 Alzheimer’s Disease and Related Disorders, New York A Torah Infertility Medium of Exchange (ATIME) 20,731 City, Inc. d/b/a CaringKind 65,215 Abraham Joshua Heschel School 397,450 Alzheimer’s Disease Research Foundation d/b/a Cure JEWISH COMMUNAL FUND JEWISH COMMUNAL Abraham Path Initiative, Inc. 42,500 Alzheimer’s Fund 71,000 Accion International 30,000 Alzheimer’s Drug Discovery Foundation 15,100 Achievement First, Inc. 170,000 Am Yisroel Chai Foundation, Inc. 25,036 Achiezer Community Resource Center, Inc. 20,728 Ameinu Our People, Inc. 17,000 Actors Fund of America 47,900 America Gives, Inc. 30,856 Adas Torah 16,500 America-Israel Cultural Foundation, Inc. 25,500 Adler Aphasia Center 14,050 America-Israel Friendship League, Inc. 55,000 Administrators of Tulane Educational Fund 11,500 American Antiquarian Society 25,000 Advanced Learning Institute 10,000 American Associates of Ben-Gurion University of Advancing Human Rights 18,000 the Negev, Inc. 71,386 Advancing Women Professionals and the Jewish American Associates of the Royal Academy Trust, Inc. 15,000 Community, Inc. 25,000 American Association for the Advancement of Science 35,000 Aegis America, Inc. 75,000 American Association of Colleges of Nursing 1,064,797 Afya Foundation of America, Inc. 67,250 American Cancer Society, Inc. -
Cal Eration New Unds, Eir and in D
UJA-FEDERATION OF NEW YORK OF NEW UJA-FEDERATION UJA-FEDERATION OF NEW YORK LEADERSHIP President Executive Committee At Large Alisa R. Doctoroff* Amy A. B. Bressman* The world’s largest local Michael Olshan* Chair of the Board Marcia Riklis* Linda Mirels* philanthropy, UJA-Federation David A. Sterling* Executive Vice President Pamela P. Wexler* REPORT OF & CEO of New York cares for John S. Ruskay Special Advisor to the President David Valger Chair, Caring Commission Jews everywhere and New Jeffrey A. Schoenfeld* Senior Vice President Financial Resource Development Yorkers of all backgrounds, STRATEGIC Chair, Commission on Mark D. Medin Jewish Identity and Renewal Sara E. Nathan* Senior Vice President connects people to their Strategic Planning & Chair, Commission on Organizational Resources Jewish communities, and the Jewish People Alisa Rubin Kurshan DIRECTIONS Alisa F. Levin* Senior Vice President responds to crises — in Chair, Jewish Communal Agency Relations Network Commission Roberta Marcus Leiner Fredric W. Yerman* New York, in Israel, and Chief Financial Officer General Chair, AND GRANTS Irvin A. Rosenthal 2014 Campaign around the world. STRATEGIC DIRECTIONS AND GRANTS DIRECTIONS STRATEGIC Jeffrey M. Stern* General Counsel Chief Compliance Officer Campaign Chairs & Secretary Wayne K. Goldstein* Ellen R. Zimmerman 2014 – 15 Cindy R. Golub* Executive Vice Presidents Emeriti William L. Mack Ernest W. Michel Treasurer Stephen D. Solender John A Herrmann, Jr.* *Executive Committee member Main Office Regional Offices New York Long Island 130 East 59th Street 6900 Jericho Turnpike, Suite 302 New York, NY 10022 Syosset, NY 11791 212.980.1000 516.677.1800 Overseas Office Westchester Israel 701 Westchester Avenue Suite 203E 48 King George Street White Plains, NY 10604 Jerusalem, Israel 91071 914.761.5100 011.972.2.620.2053 Northern Westchester 27 Radio Circle Drive 2014 – 15 Mt. -

The Baal Teshuva Movement
TAMUZ, 57 40 I JUNE, 19$0 VOLUME XIV, NUMBER 9 $1.25 ' ' The Baal Teshuva Movement Aish Hatorah • Bostoner Rebbe: Rabbi Levi Yitzchak Horowitz• CHABAD • Dvar Yerushalayim • Rabbi Shlomo · Freifeld • Gerrer Rebbe • Rabbi Baruch ·.. Horowitz • Jewish Education Progra . • Kosel Maarovi • Moreshet Avot/ El HaMekorot • NCSY • Neve Yerushalayim •Ohr Somayach . • P'eylim •Rabbi Nota Schiller• Sh' or Yashuv •Rabbi Meir Shuster • Horav Elazar Shach • Rabbi Mendel Weinbach •Rabbi Noach Weinberg ... and much much more. THE JEWISH BSERVER In this issue ... THE BAAL TESHUVA MOVEMENT Prologue . 1 4 Chassidic Insights: Understanding Others Through Ourselves, Rabbi Levi Yitzchok Horowitz. 5 A Time to Reach Out: "Those Days Have Come," Rabbi Baruch Horovitz 8 The First Step: The Teshuva Solicitors, Rabbi Hillel Goldberg 10 Teaching the Men: Studying Gemora-The Means and the Ends of the Teshuva Process, Rabbi Nola Schiller . 13 Teaching the Women: How to Handle a Hungry Heart, Hanoch Teller 16 THE JEWISH OBSERVER (ISSN Watching the Airplanes, Abraham ben Shmuel . 19 0(121-6615) is published monthly, Kiruv in Israel: except Ju!y and August. by the Bringing Them to our Planet, Ezriel Hildesheimer 20 Agudath Israel of America, 5 Beekman Street, New York, N.Y The Homecoming Ordeal: 10038. Second class postage paid Helping the Baal Teshuva in America, at New York, N.Y. Subscription Rabbi Mendel Weinbach . 25 $9.00 per year; two years. $17.50; three years, $25.00; outside of the The American Scene: United States, $10.00 per year. A Famine in the Land, Avrohom Y. HaCohen 27 Single copy, $1.25 Printed in the U.S.A. -

How to Prevent an Intermarriage
How To Prevent an Intermarriage A guide for preventing broken hearts How To Prevent an Intermarriage A guide for preventing broken hearts Rabbi Kalman Packouz © 2004 by Rabbi Kalman Packouz First edition, 1976; Second edition, 1982 Third revised and expanded edition, 2004 Aish HaTorah P.O.B. 14149 Jerusalem, Israel Tel. 9722-628-5666 To contact Rabbi Packouz: 3150 Sheridan Avenue Miami Beach, Fl. 33140 Telephone: (305) 535-2474 Fax: (305) 531-9334 E-mail: [email protected] For a free internet subscription to Rabbi Packouz's Shabbat Shalom Weekly -- Insights into life, personal growth and Torah which is read each week by over 200,000 people – either subscribe from www.shabbatshalom.org or at aish.com/torahportion/shalomweekly Go to www.preventintermarriage.com for more information and free downloads Permission is granted to photocopy whatever sections of this book you may need to communicate with someone you love the benefits of marrying someone Jewish and/or the problems facing an intermarriage. ISBN: 0-87306-371-6 Typeset by: Rosalie Lerch Intermarriage is a recognized threat to the survival of the Jewish people. There is a sore need to meet this threat. After reading How to Stop an Intermarriage twenty years ago before it was published, I wrote, "I am very much encouraged. As the first book in its field, it is more than a beginning. It is excellently done, with cogent arguments, effective suggestions, and positive approaches. It will definitely be an invaluable aid for those who want to know what they can do at this time of crisis." Now the book has proven itself as an effective tool which has helped thousands of parents in their time of need. -

Application for Admission
NEVE YERUSHALAYIM SCHOOL OF GENERAL JEWISH STUDIES Year Program Application Procedure Thank you for your interest in attending the Neve School of General Jewish Studies. • Download the application form and save it to your computer. • Complete the application form and email it to [email protected] • Attach a passport style photo to the email. • Pay an application fee of $30.00 USD. This is a required fee and is non-refundable. To pay by credit card: Please visit our secure website at: www.nevey.org/application/neapplications.php. To pay by check: Please make your check payable to Neve Yerushalayim Inc. and mail it to our admissions office When your completed form is received, it will be evaluated within approximately 10 working days, and you will receive a reply from the admissions office. Important! Flight plans should not be finalized before acceptance to the program is confirmed. For help or more information, please contact the Neve Admissions office: In Jerusalem at [email protected] or call *9722-654-4531; in the USA [email protected] or call 212-422-1110 NEVE SCHOOL of GENERAL JEWISH STUDIES Year Program Application I am applying for: Neve (multilevel) Mechina Shalhevet If you are applying to a summer program, please fill out the appropriate summer application on the site!! Last Name First & Middle Name _ __ ______ Nick Name_________________ Date of Birth ___________________________________ Place of Birth ______ _ (MM/DD/YYYY) Intended Date of Arrival___________________________ Length of Stay (estimate) ______________________ (MM/DD/YYYY) Citizenship_____________________________________ Passport No._________________________________ Marital Status: Single Married Divorced / Separated Widowed Social Security No. -

Beth David Synagogue • Chabad of Oneonta •
July 17-30, 2020 Published by the Jewish Federation of Greater Binghamton Volume XLVIX Number 28 BINGHAMTON, NEW YORK Area Synagogues: Beth David Synagogue • Chabad of Oneonta • Con- gregation Tikkun v'Or, Ithaca Reform Temple • Kol Haverim: Fin- gerlakes Community for Humanistic Judaism • Norwich Jewish Center • Penn-York Jewish Community • Rohr Chabad Center of Binghamton • Roitman Chabad Center at Cornell • Temple Beth-El, Ithaca • Temple Beth El, Oneonta • Temple Brith Sholom, Cortland • Temple Concord • Temple Israel • Binghamton Hadassah • Board of Rabbis • B'Yachad Ithaca Jewish Preschool • College of Jewish Studies • Community Relations Committee • Hillel Academy • In- ternational Jewish Film Fest of Greater Binghamton • Ithaca Area United Jewish Community • Jewish Community Center • Jewish Family Service • Jewish Federation of Greater Binghamton • The Reporter Group • William H. Seigel Lodge of B'nai B'rith • Uni- versities: Binghamton University Zionist2020 Organization • Center for Israel Studies at Binghamton University • Center for Jewish Living, Cornell University • Cornell University Hillel – Yudow- itz Center for Jewish Life • Hillel at Binghamton • Hillel at Ithaca College • Hillel at SUNY College of Oneonta • Jewish Studies Program at Cornell University • Judaic Studies Depart- ment, Binghamton University • MEOR Upstate • SUNY Cortland Hillel Area Synagogues: Beth David Synagogue • Chabad of Oneonta • Congregation Tikkun v'Or, Ithaca Reform Temple • Kol Haverim: Fingerlakes Community for Hu- manistic Judaism • Norwich