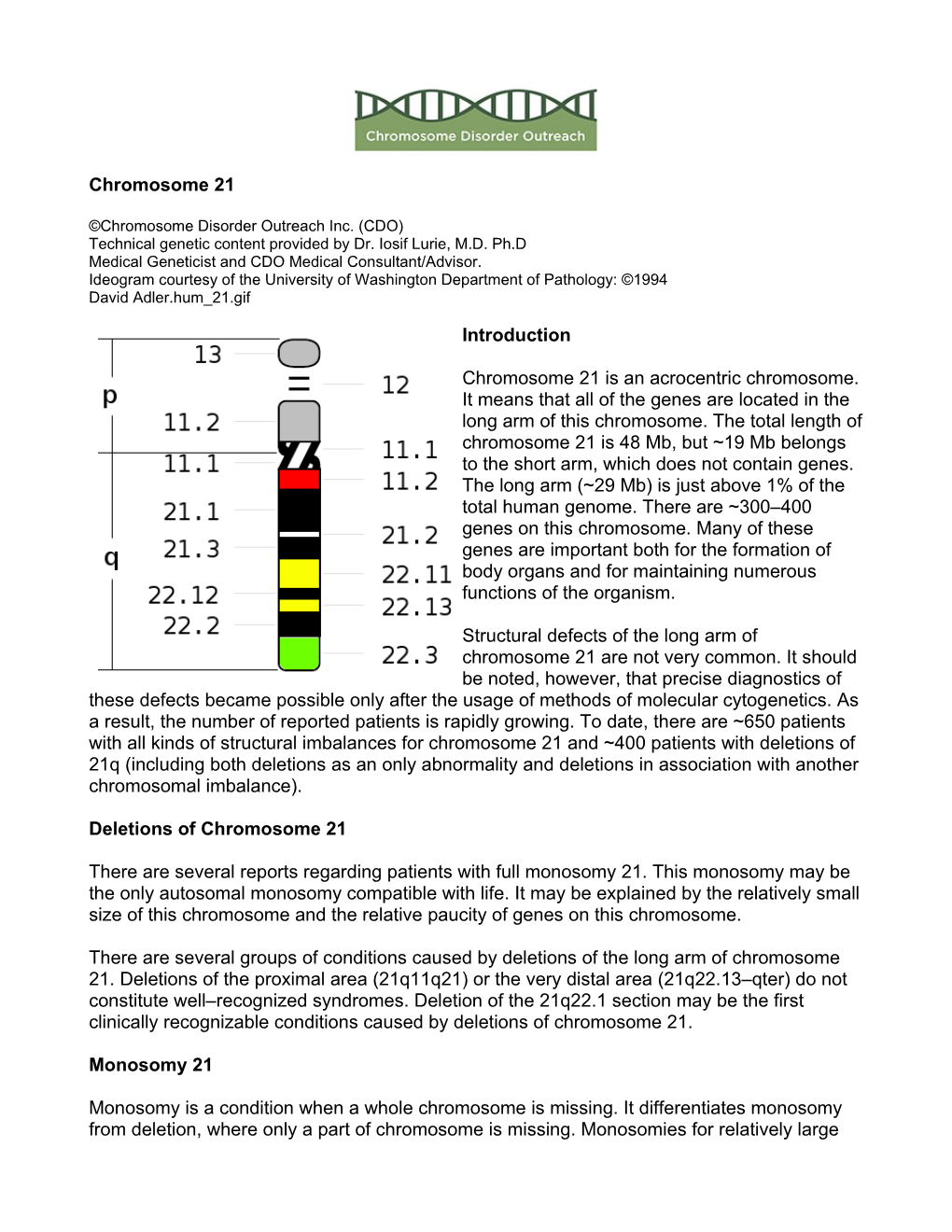
Chromosome 21 Introduction Chromosome 21 Is an Acrocentric Chromosome. It Means That All of the Genes Are Located in the Long Ar
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Ring 21 FTNW
Ring 21 rarechromo.org Sources Ring 21 The information Ring 21 is a rare genetic condition caused by having a in this leaflet ring-shaped chromosome. comes from the Almost half of the people with ring 21 chromosomes medical literature described in the medical literature are healthy and and from develop normally. Their unusual chromosomes are Unique’s discovered by chance, during tests for infertility or after members with repeated miscarriages or after having an affected baby. Ring 21 In other people the ring 21 chromosome affects (referenced U), development and learning and can also cause medical who were problems. In most of these people these effects are surveyed in slight but in some people they can be severe. The 2004. Unique is effects can even vary between different members of the very grateful to same family. The reason for these differences is not yet the families who fully understood. took part in the survey. What is a chromosome? The human body is made up of cells. Inside most cells is References a nucleus where genetic information is stored in genes which are grouped along chromosomes. Chromosomes The text contains are large enough to be studied under a microscope and references to come in different sizes, each with a short (p) and a long articles published (q) arm. They are numbered from largest to smallest in the medical according to their size, from number 1 to number 22, in press. The first- addition to the sex chromosomes, X and Y. A normal, named author healthy cell in the body has 46 chromosomes, 23 from and publication the mother and 23 from the father, including one date are given to chromosome 21 from each parent. -

Epigenetic Control of Mammalian Centromere Protein Binding: Does DNA Methylation Have a Role?
Journal of Cell Science 109, 2199-2206 (1996) 2199 Printed in Great Britain © The Company of Biologists Limited 1996 JCS3386 Epigenetic control of mammalian centromere protein binding: does DNA methylation have a role? Arthur R. Mitchell*, Peter Jeppesen, Linda Nicol†, Harris Morrison and David Kipling MRC Human Genetics Unit, Western General Hospital, Crewe Road, Edinburgh EH4 2XU, UK *Author for correspondence (internet [email protected]) †Present address: MRC Reproductive Biology Unit, Edinburgh, UK SUMMARY Chromosome 1 of the inbred mouse strain DBA/2 has a block of minor satellite DNA sequences on chromosome 1. polymorphism associated with the minor satellite DNA at The binding of the CENP-E protein does not appear to be its centromere. The more terminal block of satellite DNA affected by demethylation of the minor satellite sequences. sequences on this chromosome acts as the centromere as We present a model to explain these observations. This shown by the binding of CREST ACA serum, anti-CENP- model may also indicate the mechanism by which the B and anti-CENP-E polyclonal sera. Demethylation of the CENP-B protein recognises specific sites within the arrays minor satellite DNA sequences accomplished by growing of minor satellite DNA on mouse chromosomes. cells in the presence of the drug 5-aza-2′-deoxycytidine results in a redistribution of the CENP-B protein. This protein now binds to an enlarged area on the more terminal Key words: Centromere satellite DNA, Demethylation, Centromere block and in addition it now binds to the more internal antibody INTRODUCTION A common feature of many mammalian pericentromeric domains is that they contain families of repetitive DNA The centromere of mammalian chromosomes is recognised at sequences (Singer, 1982). -

The 50Th Anniversary of the Discovery of Trisomy 21: the Past, Present, and Future of Research and Treatment of Down Syndrome
REVIEW The 50th anniversary of the discovery of trisomy 21: The past, present, and future of research and treatment of Down syndrome Andre´Me´garbane´, MD, PhD1,2, Aime´ Ravel, MD1, Clotilde Mircher, MD1, Franck Sturtz, MD, PhD1,3, Yann Grattau, MD1, Marie-Odile Rethore´, MD1, Jean-Maurice Delabar, PhD4, and William C. Mobley, MD, PhD5 Abstract: Trisomy 21 or Down syndrome is a chromosomal disorder HISTORICAL REVIEW resulting from the presence of all or part of an extra Chromosome 21. Clinical description It is a common birth defect, the most frequent and most recognizable By examining artifacts from the Tumaco-La Tolita culture, form of mental retardation, appearing in about 1 of every 700 newborns. which existed on the border between current Colombia and Although the syndrome had been described thousands of years before, Ecuador approximately 2500 years ago, Bernal and Briceno2 it was named after John Langdon Down who reported its clinical suspected that certain figurines depicted individuals with Tri- description in 1866. The suspected association of Down syndrome with somy 21, making these potteries the earliest evidence for the a chromosomal abnormality was confirmed by Lejeune et al. in 1959. existence of the syndrome. Martinez-Frias3 identified the syn- Fifty years after the discovery of the origin of Down syndrome, the term drome in a terra-cotta head from the Tolteca culture of Mexico “mongolism” is still inappropriately used; persons with Down syn- in 500 patients with AD in which the facial features of Trisomy drome are still institutionalized. Health problems associated with that 21 are clearly displayed. -

Biol 1020: Chromosomal Genetics
Ch. 15: Chromosomal Abnormalities Abnormalities in Chromosomal Number Abnormalities in Chromosomal Structure: Rearrangements Fragile Sites . • Define: – nondisjunction – polyploidy – aneupoidy – trisomy – monosomy . Abnormalities in chromosomal number How does it happen? . Abnormalities in chromosomal number nondisjunction - mistake in cell division where chromosomes do not separate properly in anaphase usually in meiosis, although in mitosis occasionally in meiosis, can occur in anaphase I or II . Abnormalities in chromosomal number polyploidy – complete extra sets (3n, etc.) – fatal in humans, most animals aneuploidy – missing one copy or have an extra copy of a single chromosome three copies of a chromosome in your somatic cells: trisomy one copy of a chromosome in your somatic cells: monosomy most trisomies and monosomies are lethal well before birth in humans; exceptions will be covered . Abnormalities in chromosomal number generally, in humans autosomal aneuploids tend to be spontaneously aborted over 1/5 of human pregnancies are lost spontaneously after implantation (probably closer to 1/3) chromosomal abnormalities are the leading known cause of pregnancy loss data indicate that minimum 10-15% of conceptions have a chromosomal abnormality at least 95% of these conceptions spontaneously abort (often without being noticed) . • Define: – nondisjunction – polyploidy – aneupoidy – trisomy – monosomy . • Describe each of the aneuploidies that can be found in an appreciable number of human adults (chromosomal abnormality, common name of the syndrome if it has one, phenotypes) . aneuploidy in human sex chromosomes X_ female (Turner syndrome) short stature; sterile (immature sex organs); often reduced mental abilities about 1 in 2500 human female births XXY male (Klinefelter syndrome) often not detected until puberty, when female body characteristics develop sterile; sometimes reduced mental abilities; testosterone shots can be used as a partial treatment; about 1 in 500 human male births . -

Evolution on the X Chromosome: Unusual Patterns and Processes
REVIEWS Evolution on the X chromosome: unusual patterns and processes Beatriz Vicoso and Brian Charlesworth Abstract | Although the X chromosome is usually similar to the autosomes in size and cytogenetic appearance, theoretical models predict that its hemizygosity in males may cause unusual patterns of evolution. The sequencing of several genomes has indeed revealed differences between the X chromosome and the autosomes in the rates of gene divergence, patterns of gene expression and rates of gene movement between chromosomes. A better understanding of these patterns should provide valuable information on the evolution of genes located on the X chromosome. It could also suggest solutions to more general problems in molecular evolution, such as detecting selection and estimating mutational effects on fitness. Haldane’s rule Sex-chromosome systems have evolved independently the predictions of theoretical models of X-chromosome The disproportionate loss of many times, and have attracted much attention from evolution will shed light on the assumptions on which fitness to the heterogametic evolutionary geneticists. This work has mainly focused the models are based, such as the degree of dominance of sex in F1 hybrids between on the steps leading to the initial evolution of sex chro- mutations and the existence of opposing forces species. mosomes, and the genetic degeneration of Y and W of selection on males and females, leading to a better 1 Clade chromosomes . Here, we discuss the evolution of the understanding of the forces that shape the evolution of A group of species which share X chromosome in long-established sex-chromosome eukaryotic genomes. a common ancestor. -

Dr. Fern Tsien, Dept. of Genetics, LSUHSC, NO, LA Down Syndrome
COMMON TYPES OF CHROMOSOME ABNORMALITIES Dr. Fern Tsien, Dept. of Genetics, LSUHSC, NO, LA A. Trisomy: instead of having the normal two copies of each chromosome, an individual has three of a particular chromosome. Which chromosome is trisomic determines the type and severity of the disorder. Down syndrome or Trisomy 21, is the most common trisomy, occurring in 1 per 800 births (about 3,400) a year in the United States. It is one of the most common genetic birth defects. According to the National Down Syndrome Society, there are more than 400,000 individuals with Down syndrome in the United States. Patients with Down syndrome have three copies of their 21 chromosomes instead of the normal two. The major clinical features of Down syndrome patients include low muscle tone, small stature, an upward slant to the eyes, a single deep crease across the center of the palm, mental retardation, and physical abnormalities, including heart and intestinal defects, and increased risk of leukemia. Every person with Down syndrome is a unique individual and may possess these characteristics to different degrees. Down syndrome patients Karyotype of a male patient with trisomy 21 What are the causes of Down syndrome? • 95% of all Down syndrome patients have a trisomy due to nondisjunction before fertilization • 1-2% have a mosaic karyotype due to nondisjunction after fertilization • 3-4% are due to a translocation 1. Nondisjunction refers to the failure of chromosomes to separate during cell division in the formation of the egg, sperm, or the fetus, causing an abnormal number of chromosomes. As a result, the baby may have an extra chromosome (trisomy). -

Continuous Variation in Y-Chromosome Structure of Rumex Acetosa
Heredity 57 (1986) 247-254 The Genetical Society of Great Britain Received 16 December 1985 Continuous variation in Y-chromosome structure of Rumex acetosa A. S. Wilby and School of Biological Sciences, J. S. Parker Queen Mary College, Mile End Road, London El 4NS. The dioecious angiosperm Rumex acetosa has an XXIXY1Y2sex-chromosomesystem. Each V-chromosome is heterochromatic except for a minute terminal euchromatic pairing segment. The Vs are constant in size but have a variable centromere position. The centromeres can be located anywhere within the central 40 per cent of the chromosome but are excluded from the two distal 30 per cent regions. In a sample of 270 males from 18 different populations 68 distinct variants have been identified on the basis of V-morphology. All populations are highly polymorphic with a minimum of four variants in a sample of ten males. The origin and significance of this massive variability is considered in this paper. Increased mutation rate of the Ys may be implicated in maintenance of this variation. I NTRO DUCTI ON these "inert" Ys has been described (Vana, 1972) variation in their structure has been overlooked. Sex-determinationin animals is usually genic and Extensive heterochroinatic content is a charac- frequently associated with visibly-differentiated teristic of many Y- and W-chromosomes. Indeed, sex-chromosomes. Sex expression in plants, some have argued that the process of hetero- however, is usually more plastic, and is subject to chromatinisation itself was implicated in the initial environmental influences such as temperature and phase of sex-chromosome differentiation (Jones, photoperiod (Heslop-Harrison, 1957). -

Cytogenetics, Chromosomal Genetics
Cytogenetics Chromosomal Genetics Sophie Dahoun Service de Génétique Médicale, HUG Geneva, Switzerland [email protected] Training Course in Sexual and Reproductive Health Research Geneva 2010 Cytogenetics is the branch of genetics that correlates the structure, number, and behaviour of chromosomes with heredity and diseases Conventional cytogenetics Molecular cytogenetics Molecular Biology I. Karyotype Definition Chromosomal Banding Resolution limits Nomenclature The metaphasic chromosome telomeres p arm q arm G-banded Human Karyotype Tjio & Levan 1956 Karyotype: The characterization of the chromosomal complement of an individual's cell, including number, form, and size of the chromosomes. A photomicrograph of chromosomes arranged according to a standard classification. A chromosome banding pattern is comprised of alternating light and dark stripes, or bands, that appear along its length after being stained with a dye. A unique banding pattern is used to identify each chromosome Chromosome banding techniques and staining Giemsa has become the most commonly used stain in cytogenetic analysis. Most G-banding techniques require pretreating the chromosomes with a proteolytic enzyme such as trypsin. G- banding preferentially stains the regions of DNA that are rich in adenine and thymine. R-banding involves pretreating cells with a hot salt solution that denatures DNA that is rich in adenine and thymine. The chromosomes are then stained with Giemsa. C-banding stains areas of heterochromatin, which are tightly packed and contain -

Down's Syndrome Phenotype and Autosomal Gene Inactivation in a Child with Presumed
J Med Genet: first published as 10.1136/jmg.19.2.144 on 1 April 1982. Downloaded from 144 Case reports Down's syndrome phenotype and Case report autosomal gene inactivation in a The proband, a 3 2-year-old white female, was referred for evaluation of developmental delay and child with presumed (X;21) de novo dysmorphic features. She was the 1790 g,. 39 week translocation gestation product of a gravida 1, para 0, 15-year-old female. The pregnancy was complicated with SUMMARY A 32-year-old female with clinical recurrent urinary tract infections. The mother used features of Down's syndrome was found to have alcohol and tobacco in small quantities during the extra chromosome material on the long arm of pregnancy. The labour lasted ten hours and the one of the X chromosomes, 46,XXq+. The delivery was vaginal with vertex presentation. The parental karyotypes were normal. In the light baby breathed and cried spontaneously. Her of the clinical features of the proband and the immediate neonatal course was uneventful, but her subsequent weight gain was poor. She had several banding characteristics of the extra chromosome admissions to hospital for repeated diarrhoea, otitis material, the patient was thought to have a de media, and pneumonia. She had two 'febrile' seizures novo (X;21) translocation. The results of late for which she was placed on phenobarbital. Her replication studies with BUdR and enzyme development was markedly delayed. She smiled at superoxide dismutase (SOD) assays in the 4 months, turned over at 7 months, walked at 18 proband suggest that: (1) the presumed (X;21) months, and was not yet toilet trained. -

Amplified Fragments of an Autosome-Borne Gene
G C A T T A C G G C A T genes Article Amplified Fragments of an Autosome-Borne Gene Constitute a Significant Component of the W Sex Chromosome of Eremias velox (Reptilia, Lacertidae) Artem Lisachov 1,2,* , Daria Andreyushkova 3, Guzel Davletshina 2,3, Dmitry Prokopov 3 , Svetlana Romanenko 3 , Svetlana Galkina 4 , Alsu Saifitdinova 5 , Evgeniy Simonov 1, Pavel Borodin 2,6 and Vladimir Trifonov 3,6 1 Institute of Environmental and Agricultural Biology (X-BIO), University of Tyumen, Lenina str. 23, 625003 Tyumen, Russia; [email protected] 2 Institute of Cytology and Genetics SB RAS, Acad. Lavrentiev Ave. 10, 630090 Novosibirsk, Russia; [email protected] (G.D.); [email protected] (P.B.) 3 Institute of Molecular and Cellular Biology SB RAS, Acad. Lavrentiev Ave. 8/2, 630090 Novosibirsk, Russia; [email protected] (D.A.); [email protected] (D.P.); [email protected] (S.R.); [email protected] (V.T.) 4 Department of Genetics and Biotechnology, Saint Petersburg State University, Universitetskaya Emb. 7–9, 199034 Saint Petersburg, Russia; [email protected] 5 Department of Human and Animal Anatomy and Physiology, Herzen State Pedagogical University of Russia, Moyka Emb. 48, 191186 Saint Petersburg, Russia; saifi[email protected] 6 Novosibirsk State University, Pirogova str. 3, 630090 Novosibirsk, Russia Citation: Lisachov, A.; * Correspondence: [email protected] Andreyushkova, D.; Davletshina, G.; Prokopov, D.; Romanenko, S.; Abstract: Heteromorphic W and Y sex chromosomes often experience gene loss and heterochroma- Galkina, S.; Saifitdinova, A.; Simonov, tinization, which is frequently viewed as their “degeneration”. -

Comprehensive Chromosomal and Mitochondrial Copy Number Profiling in Human IVF Embryos
ARTICLE IN PRESS 1bs_bs_query Q2 Article 2bs_bs_query 3bs_bs_query Comprehensive chromosomal and mitochondrial copy 4bs_bs_query 5bs_bs_query number profiling in human IVF embryos 6bs_bs_query Q1 a,1, a,1 a a 7bs_bs_query Wei Shang *, Yunshan Zhang , Mingming Shu , Weizhou Wang , a a b b, b b 8bs_bs_query Likun Ren , Fu Chen , Lin Shao , Sijia Lu *, Shiping Bo , Shujie Ma , b 9bs_bs_query Yumei Gao a 10bs_bs_query Assisted Reproductive Centre of the Department of Gynaecology and Obstetrics, PLA Naval General Hospital, 11 bs_bs_query Haidian District, Beijing 100048, China b 12bs_bs_query Yikon Genomics, Fengxian District, Shanghai 201400, China 13bs_bs_query 14bs_bs_query 15bs_bs_query Wei Shang has been the Associate Chief Physician at the Department of Gynaecology and Obstetrics, PLA Naval 16bs_bs_query General Hospital, Beijing, since 2005. Her research interests focus on assisted reproduction technology, repro- 17bs_bs_query ductive endocrinology and ovary dysfunction. 18bs_bs_query 19bs_bs_query KEY MESSAGE 20bs_bs_query Using a validated approach called MALBAC-NGS, a comprehensive chromosomal and mitochondrial copy number 21bs_bs_query profiling in human embryos was conducted, and correlations of mitochondria quantity with maternal age and 22bs_bs_query embryo stage were observed. The strategy might be used to perform an advanced PGS targeting both chro- 23bs_bs_query mosomal and mitochondria copy numbers. 24bs_bs_query 25bs_bs_query ABSTRACT 26bs_bs_query 27bs_bs_query Single cell whole genome sequencing helps to decipher the genome -

Molecular Evolution of a Y Chromosome to Autosome Gene Duplication in Drosophila Research Article
Molecular Evolution of a Y Chromosome to Autosome Gene Duplication in Drosophila Kelly A. Dyer,*,1 Brooke E. White,1 Michael J. Bray,1 Daniel G. Pique´,1 and Andrea J. Betancourt* ,2 1Department of Genetics, University of Georgia 2Institute of Evolutionary Biology, University of Edinburgh, Ashworth Labs, Edinburgh, United Kingdom Present address: Institute for Population Genetics, University of Veterinary Medicine Vienna, Vienna 1210, Austria *Corresponding author: [email protected], [email protected]. Associate editor: Jody Hey Abstract In contrast to the rest of the genome, the Y chromosome is restricted to males and lacks recombination. As a result, Research article Y chromosomes are unable to respond efficiently to selection, and newly formed Y chromosomes degenerate until few genes remain. The rapid loss of genes from newly formed Y chromosomes has been well studied, but gene loss from highly degenerate Y chromosomes has only recently received attention. Here, we identify and characterize a Y to autosome duplication of the male fertility gene kl-5 that occurred during the evolution of the testacea group species of Drosophila. The duplication was likely DNA based, as other Y-linked genes remain on the Y chromosome, the locations of introns are conserved, and expression analyses suggest that regulatory elements remain linked. Genetic mapping reveals that the autosomal copy of kl-5 resides on the dot chromosome, a tiny autosome with strongly suppressed recombination. Molecular evolutionary analyses show that autosomal copies of kl-5 have reduced polymorphism and little recombination. Importantly, the rate of protein evolution of kl-5 has increased significantly in lineages where it is on the dot versus Y linked.