Chemical Muscle Enhancement (The BDR) by Author L
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Ranvet's Filybol
Ranvet's Filybol Ranvet Chemwatch Hazard Alert Code: 2 Chemwatch: 4787-83 Issue Date: 08/02/2016 Version No: 5.1.1.1 Print Date: 10/28/2016 Safety Data Sheet according to WHS and ADG requirements S.GHS.AUS.EN SECTION 1 IDENTIFICATION OF THE SUBSTANCE / MIXTURE AND OF THE COMPANY / UNDERTAKING Product Identifier Product name Ranvet's Filybol Chemical Name peanut oil Synonyms Not Available Other means of Not Available identification Relevant identified uses of the substance or mixture and uses advised against Relevant identified Non-virilising anabolic combination for fillies, mares, colts and stallions. uses Details of the supplier of the safety data sheet Registered company Ranvet name Address 10-12 Green Street Banksmeadow NSW 2019 Australia Telephone +61 2 9666 1744 Fax +61 2 9666 1755 Website https://www.ranvet.com.au/other_msds.htm Email [email protected] Emergency telephone number Association / Not Available Organisation Emergency telephone +61 425 061 584 numbers Other emergency Not Available telephone numbers SECTION 2 HAZARDS IDENTIFICATION Classification of the substance or mixture Poisons Schedule S4 Carcinogenicity Category 2, Reproductive Toxicity Category 2, Acute Aquatic Hazard Category 2, Chronic Aquatic Hazard Classification [1] Category 2 1. Classified by Chemwatch; 2. Classification drawn from HSIS ; 3. Classification drawn from EC Directive 1272/2008 - Annex Legend: VI Label elements GHS label elements SIGNAL WORD WARNING Continued... Chemwatch: 4787-83 Page 2 of 10 Issue Date: 08/02/2016 Version No: 5.1.1.1 Ranvet's Filybol Print Date: 10/28/2016 Hazard statement(s) H351 Suspected of causing cancer. H361 Suspected of damaging fertility or the unborn child. -

Safety Data Sheet
SAFETY DATA SHEET SECTION 1: PRODUCT IDENTIFICATION PRODUCT NAME DHEA (Prasterone) (Micronized) PRODUCT CODE 0733 SUPPLIER MEDISCA Inc. Tel.: 1.800.932.1039 | Fax.: 1.855.850.5855 661 Route 3, Unit C, Plattsburgh, NY, 12901 3955 W. Mesa Vista Ave., Unit A-10, Las Vegas, NV, 89118 6641 N. Belt Line Road, Suite 130, Irving, TX, 75063 MEDISCA Pharmaceutique Inc. Tel.: 1.800.665.6334 | Fax.: 514.338.1693 4509 Rue Dobrin, St. Laurent, QC, H4R 2L8 21300 Gordon Way, Unit 153/158, Richmond, BC V6W 1M2 MEDISCA Australia PTY LTD Tel.: 1.300.786.392 | Fax.: 61.2.9700.9047 Unit 7, Heritage Business Park 5-9 Ricketty Street, Mascot, NSW 2020 EMERGENCY PHONE CHEMTREC Day or Night Within USA and Canada: 1-800-424-9300 NSW Poisons Information Centre: 131 126 USES Adjuvant; Androgen SECTION 2: HAZARDS IDENTIFICATION GHS CLASSIFICATION Toxic to Reproduction (Category 2) PICTOGRAM SIGNAL WORD Warning HAZARD STATEMENT(S) Reproductive effector, prohormone. Suspected of damaging fertility or the unborn child. May cause harm to breast-fed children. Causes serious eye irritation. Causes skin and respiratory irritation. Very toxic to aquatic life with long lasting effects. AUSTRALIA-ONLY HAZARDS Not Applicable. PRECAUTIONARY STATEMENT(S) Prevention Wash thoroughly after handling. Obtain special instructions before use. Do not handle until all safety precautions have been read and understood. Do not breathe dusts or mists. Do not eat, drink or smoke when using this product. Avoid contact during pregnancy/while nursing. Wear protective gloves, protective clothing, eye protection, face protection. Avoid release to the environment. Response IF ON SKIN (HAIR): Wash with plenty of water. -

Vargas KEA, Et Al. Hepatotoxicity Associated with Methylstenbolone and Copyright© Vargas KEA, Et Al
1. Medical Journal of Clinical Trials & Case Studies ISSN: 2578-4838 Hepatotoxicity Associated with Methylstenbolone and Stanozolol Abuse Vargas KEA*, Guaraná TA, Biccas BN, Agoglia LV, Carvalho ACG, Case Report Gismondi R and Esberard EBC Volume 2 Issue 5 Received Date: July 27, 2018 Department of Gastroenterology/Hepatology, Department of Clinical Medicine, and Published Date: September 03, 2018 Department of Pathology, Antônio Pedro University Hospital, Federal Fluminense DOI: 10.23880/mjccs-16000176 University, Rio de Janeiro, Brazil *Corresponding author: Vargas Karen Elizabeth Arce, Department of Gastroenterology/Hepatology, Department of Clinical Medicine, and Department of Pathology, Antônio Pedro University Hospital, Federal Fluminense University, Rio de Janeiro, Ernani do Amaral Peixoto Avenue, 935. Ap.901 / Cep.24020043, Brazil, Tel: 005521981584624; Email: [email protected] Abstract Background & Objectives: Drug hepatotoxicity is a major cause of liver disease. Many drugs are well known to induce liver damage. Some toxic products, like anabolic androgenic steroids, that are pharmaceutical preparations since they contain pharmaceutically active substance, are available as nutritional supplements. Many patients are used to consume these like dietary stuff. Methods: We introduce a case series of two patients who developed hepatic damage after the consumption of anabolic- androgenic steroids, accompanied by a detailed bibliographic research on this topic. Results: We present two young men who developed significant liver damage, both with hyperbilirubinemia pattern after consumption of anabolic-androgenic steroids. This was associated with considerable morbidity, although both recovered without liver transplantation. The two anabolic-androgenic steroids were being marketed as dietary supplements. Conclusions: Although not well controlled substances in Brazil, anabolic-androgenic steroids are cause of severe hepatotoxicity. -

New Zealand Data Sheet 1. Product Name
NEW ZEALAND DATA SHEET 1. PRODUCT NAME SUSTANON 250 (250 mg testosterone esters solution for injection) (SUSTANON) TESTOSTERONE ESTERS 250mg/mL for injection Presentations that are not currently available The vials are currently not available 2. QUALITATIVE AND QUANTITATIVE COMPOSITION Name and strength of the active substances - testosterone proprionate 30mg testosterone phenylpropionate 60mg testosterone isocaproate 60mg testosterone decanoate 100mg All four compounds are esters of the natural hormone testosterone. The total amount of testosterone per 1 mL is 176mg. List of excipients - 1 mL arachis oil and the solution also contains 10 per cent benzyl alcohol. For the full list of excipients, see section 6.1. 3. PHARMACEUTICAL FORM Oily solution for intramuscular use. A clear, pale yellow solution. Each clear glass ampoule or vial contains 1 mL in arachis oil. 4. CLINICAL PARTICULARS 4.1 Therapeutic indications Testosterone replacement therapy in males for conditions associated with primary and secondary hypogonadism, either congenital or acquired. In female to male transsexuals: • masculinization Moreover, in men testosterone therapy may be indicated in osteoporosis caused by androgen deficiency. 4.2 Dose and method of administration In general, the dose should be adjusted according to the response of the individual patient. Dose Adults (incl. elderly): Usually, one injection of 1ml per three weeks is adequate. Paediatric population: Safety and efficacy in children and adolescents, have not yet been established. Pre-pubertal children treated with SUSTANON should be treated with caution (see Warnings and Precautions). SUSTANON contains benzyl alcohol and is contraindicatedin children under 3 years of age. Method of administration SUSTANON should be administered by deep intramuscular injection. -

Records of Pharmaceutical and Biomedical Sciences
REVIEW ARTICLE RECORDS OF PHARMACEUTICAL AND BIOMEDICAL SCIENCES Effect of Exogenous Anabolic Androgenic Steroids on Testosterone/ Epitestosterone Ratio and its Application on Athlete Biological Passport in Egypt Hanem A. Khalil a, Dina M. Abo-Elmatty b, Rosa V. Alemany c, Noha M. Mesbah b a Egyptian Anti-Doping Organization, Cairo, Egypt. b Faculty of Pharmacy, Department of Biochemistry Suez Canal University, Ismailia, Egypt. C Catalonian Anti-Doping Laboratory of Fundacio IMIM, Barcelona, Spain. Abstract Received on: 01.09. 2018 Using the Anabolic Androgenic Steroid (AAS) agents is evident not only Revised on: 21. 10. 2018 within the competitive senior and junior athletes, but also in non-sporting contexts by individuals seeking to „improve‟ their physique. No accurate data Accepted on: 01. 11. 2018 is available for the prevalence of AAS misuse among athletes. Studies suggest that it may be 1–5% of the population; with the prevalence being higher in males. Many studies documented side effects and health hazards with the misuse of anabolic steroids, where these were accused as a cause of Correspondence Author: deaths among athletes. Intake of exogenous anabolic steroids disturbed the Testosterone / Epitestosterone (T/E) ratio causing its evaluation above the Tel:+201270206648. normal level. This review outlines the anabolic steroids, its side effects and E-mail address: health impacts in both the sporting and physique development contexts. It also provides a brief review of the history of AAS as doping agents and [email protected] athlete biological passport. Conclusion: Doping among athletes is a widespread public health and social problem. Many studies have shown that both short- and long-term health complications have consequences and dependencies. -
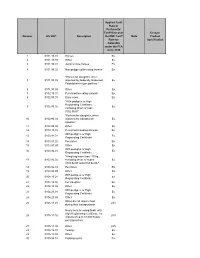
Number HS 2007 Description Applied Tariff Rate Or Preferential Tariff Rate
Applied Tariff Rate or Preferential Tariff Rate over Ex-out / Number HS 2007 Description the NMF Tariff Note Product Rate for Specification Colombia under the FTA since 2010 1 0101.10.01 Horses Ex. 2 0101.10.99 Other Ex. 3 0101.90.01 Jump or race horses Ex. 4 0101.90.02 Non pedigreed breeding horses Ex. "Horses for slaughter, when 5 0101.90.03 imported by Federally Inspected Ex. Establishment type packers." 6 0101.90.99 Other Ex. 7 0102.10.01 Pure-bred breeding animals Ex. 8 0102.90.01 Dairy cows Ex. "With pedigree or High Registrating Certificate, 9 0102.90.02 Ex. excluding those of code 0102.90.01" "Bovines for slaughter, when 10 0102.90.03 imported by Industrial de Ex. Abastos." 11 0102.90.99 Other Ex. 12 0103.10.01 Pure-bred breeding animals Ex. With pedigree or High 13 0103.91.01 Ex. Registrating Certificate. 14 0103.91.02 Peccaries Ex. 15 0103.91.99 Other Ex. With pedigree or High 16 0103.92.01 Ex. Registrating Certificate. "Weighing more than 110 kg., 17 0103.92.02 excluding those of codes Ex. 0103.92.01 and 0103.92.03." 18 0103.92.03 Peccaries Ex. 19 0103.92.99 Other Ex. With pedigree or High 20 0104.10.01 Ex. Registrating Certificate. 21 0104.10.02 For slaughter. Ex. 22 0104.10.99 Other Ex. With pedigree or High 23 0104.20.01 Ex. Registrating Certificate. 24 0104.20.99 Other Ex. When do not require food 25 0105.11.01 28% during their transportation Newly born breeding birds, with High Registrating Certificate, for 26 0105.11.02 28% imports of up to 18,000 heads per transaction. -

Reproductive DHEA
Reproductive DHEA Analyte Information - 1 - DHEA Introduction DHEA (dehydroepiandrosterone), together with other important steroid hormones such as testosterone, DHT (dihydrotestosterone) and androstenedione, belongs to the group of androgens. Androgens are a group of C19 steroids that stimulate or control the development and maintenance of male characteristics. This includes the activity of the male sex organs and the development of secondary sex characteristics. Androgens are also precursors of all estrogens, the female sex hormones. DHEA (dehydroepiandrosterone) is the aromatic C19-steroid composed of a 10,13-dimethyl, 3-hydroxy group and 17-ketone. Its chemical name is 3β-hydroxy-5-androsten-17-one, its summary formula is C19H28O2, and its molecular weight (Mr) is 288.4 Da. The structural formulas of DHEA and related androgens are shown in Fig.1 Fig.1: Structural formulas of the most important androgens DHEA Androstenedione Testosterone Dihydrotestosterone There are more than 40 other names used for DHEA, including: (+)-Dehydroisoandrosterone; (3beta, 16alpha)-3,16-dihydroxy-androst-5-en- 17-one; 5,6-Dehydroisoandrosterone; 17-Chetovis, 17-Hormoforin, Andrestenol, Diandron, Prasterone and so on. As DHEA is very closely connected with its sulfate form DHEA-S, both hormones are mentioned together in the following text. Biosynthesis DHEA is the steroid hormone belonging to the weak androgens. DHEA and DHEA-S are the major C19 steroids produced from cholesterol by the zona reticularis of the adrenal cortex (Fig.2). DHEA is also produced in small quantities in the gonads (testis and ovary3,8,14), in adipose tissue and in the brain. From this point of view DHEA belongs to the neurosteroids22. -

Steroids and Other Appearance and Performance Enhancing Drugs (Apeds) Research Report
Research Report Revised Febrero 2018 Steroids and Other Appearance and Performance Enhancing Drugs (APEDs) Research Report Table of Contents Steroids and Other Appearance and Performance Enhancing Drugs (APEDs) Research Report Introduction What are the different types of APEDs? What is the history of anabolic steroid use? Who uses anabolic steroids? Why are anabolic steroids misused? How are anabolic steroids used? What are the side effects of anabolic steroid misuse? How does anabolic steroid misuse affect behavior? What are the risks of anabolic steroid use in teens? How do anabolic steroids work in the brain? Are anabolic steroids addictive? How are anabolic steroids tested in athletes? What can be done to prevent steroid misuse? What treatments are effective for anabolic steroid misuse? Where can I get further information about steroids? References Page 1 Steroids and Other Appearance and Performance Enhancing Drugs (APEDs) Research Report Esta publicación está disponible para su uso y puede ser reproducida, en su totalidad, sin pedir autorización al NIDA. Se agradece la citación de la fuente, de la siguiente manera: Fuente: Instituto Nacional sobre el Abuso de Drogas; Institutos Nacionales de la Salud; Departamento de Salud y Servicios Humanos de los Estados Unidos. Introduction Appearance and performance enhancing drugs (APEDs) are most often used by males to improve appearance by building muscle mass or to enhance athletic performance. Although they may directly and indirectly have effects on a user’s mood, they do not produce a euphoric high, which makes APEDs distinct from other drugs such as cocaine, heroin, and marijuana. However, users may develop a substance use disorder, defined as continued use despite adverse consequences. -

Michigan Department of Community Health
Michigan Department 0f Community Health, Office of Drug Control Policy The Michigan Association of Community Mental Health March 27, 2009 NationalNational TrendsTrends andand DeterrentDeterrent StrategiesStrategies ForFor PrescriptionPrescription andand OTCOTC DrugDrug AbuseAbuse Joseph Rannazzisi Deputy Assistant Administrator Office of Diversion Control Drug Enforcement Administration IntroductionIntroduction BackgroundBackground andand StatisticsStatistics RegulatoryRegulatory ControlControl MethodsMethods ofof DiversionDiversion InternetInternet DiversionDiversion CommonlyCommonly DivertedDiverted PharmaceuticalsPharmaceuticals Steroids/Steroids/hGHhGH DietaryDietary SupplementsSupplements SalviaSalvia DivinorumDivinorum TheThe 19601960’’ss Marijuana Seconal LSD Dexedrine Meprobamate TheThe 19701970’’ss Heroin T’s and Blues 4’s and Doors (Talwin and Pyrabenzamine) TheThe 19801980’’ss Tylenol w/Codeine and Doriden Hydromorphone Cocaine TheThe 19901990’’ss Oxycodone Methamphetamine 20002000 Hydrocodone Ketamine Alprazolam Flunitrazapam MDMA (Rohypnol) Scope and Extent of Problem 2004 2007 0.30.3 millionmillion 0.35 million SedativesSedatives 1.21.2 millionmillion 1.11.1 millionmillion StimulantsStimulants 1.61.6 millionmillion 1.81.8 millionmillion Anti-Anxiety Medication 4.44.4 millionmillion 5.25.2 millionmillion NarcoticNarcotic PainPain RelieversRelievers Source: 2004 and 2007 National Survey on Drug Use and Health TeensTeens andand TheirTheir AttitudesAttitudes 1 in 5 teens report abusing Rx medications to get high 2 in -

A28 Anabolic Steroids
Anabolic SteroidsSteroids A guide for users & professionals his booklet is designed to provide information about the use of anabolic steroids and some of the other drugs Tthat are used in conjunction with them. We have tried to keep the booklet free from technical jargon but on occasions it has proven necessary to include some medical, chemical or biological terminology. I hope that this will not prevent the information being accessible to all readers. The first section explaining how steroids work is the most complex, but it gets easier to understand after that (promise). The booklet is not intended to encourage anyone to use these drugs but provides basic information about how they work, how they are used and the possible consequences of using them. Anabolic Steroids A guide for users & professionals Contents Introduction .........................................................7 Formation of Testosterone ...............................................................8 Method of Action ..............................................................................9 How Steroids Work (illustration).......................................................10 Section 1 How Steroids are Used ....................................... 13 What Steroid? ................................................................................ 14 How Much to Use? ......................................................................... 15 Length of Courses? ........................................................................ 15 How Often to Use Steroids? -

Pdf 86.39 Kb
“Detection of Testosterone Esters in Blood Sample” Dr. G. Gmeiner, Dr. G. Forsdahl, Dr. Erceg (Seibersdorf Labor GmbH, Austria) Project Summary Testosterone is still regarded as the major contributor to steroid doping world-wide. Among the most common forms of application are injections of different sorts of esters. State-of-the-Art detection of Testosterone doping includes the quantification of the Testosterone /Epitestosterone – Ratio (T/E – ratio) as well as subsequent Isotope ratio mass spectrometry (IRMS). Previous published studies of our research group have demonstrated that a comparably high percentage of testosterone preparations do not significantly differ from endogenous values of testosterone and markers of testosterone doping. Consequently when such preparations with endogenous – like 13CVPDB values are applied, IRMS - technology fails to detect testosterone doping. Direct detection of the testosterone ester leads to an unequivocal proof of doping with testosterone preparations, because such esters are not built endogenously. Previous studies indicate that a direct detection of testosterone esters in both hair and plasma is possible. Aim of the proposed project is the investigation and optimisation of the direct detection of testosterone esters in body fluids like serum, whole blood and stabilized blood with an already developed detection method using modern and sensitive technology. The project will gain information on diagnostic windows for detection of doping using testosterone esters and proper sampling conditions. Additional aim of the proposed project is to evaluate the suitability of already collected blood samples in doping control (e.g. samples collected for blood parameter measurement or growth hormone detection) for a possible reanalysis for testosterone esters. -

Neurologic Functions, Hormonal Regulation, and Psychological Factors Affect Sexual Desire and Arousal to Some Extent
Neurologic functions, hormonal regulation, and psychological factors affect sexual desire and arousal to some extent. Menopause, and the genitourinary symptoms associated with it, also affect sexual function. Understanding the pathogenesis of sexual dysfunction is key to management decisions. ILLUSTRATION: KIMBERLY MARTENS FOR OBG MANAGEMENT MARTENS KIMBERLY ILLUSTRATION: 34 OBG Management | September 2017 | Vol. 29 No. 9 obgmanagement.com UPDATE FEMALE SEXUAL DYSFUNCTION New and emerging treatment options hold promise for improving outcomes in this undertreated disorder ❯❯ Barbara S. Levy, MD Dr. Levy is Vice President for Health Policy at the American College of Obstetricians and Gynecologists, Washington, DC. The author reports no financial relationships relevant to this article. exual function is a complex, multifac- chronic conditions such as diabetes and S eted process mediated by neurologic back pain.4 functions, hormonal regulation, and psy- Understanding the pathogenesis of chological factors. What could possibly female sexual dysfunction helps to guide go wrong? our approach to its management. Indeed, IN THIS As it turns out, quite a lot. Female sex- increased understanding of its pathology has ARTICLE ual dysfunction is a common, vastly under- helped to usher in new and emerging treat- treated sexual health problem that can have ment options, as well as a personalized, bio- How hormones, wide-reaching effects on a woman’s life. psychosocial approach to its management. experience, These effects may include impaired body In this Update, I discuss the interplay of and behavior affect image, self-confidence, and self-worth. Sex- physiologic and psychological factors that the brain ual dysfunction also can contribute to rela- affect female sexual function as well as the page 36 tionship dissatisfaction and leave one feeling latest options for its management.