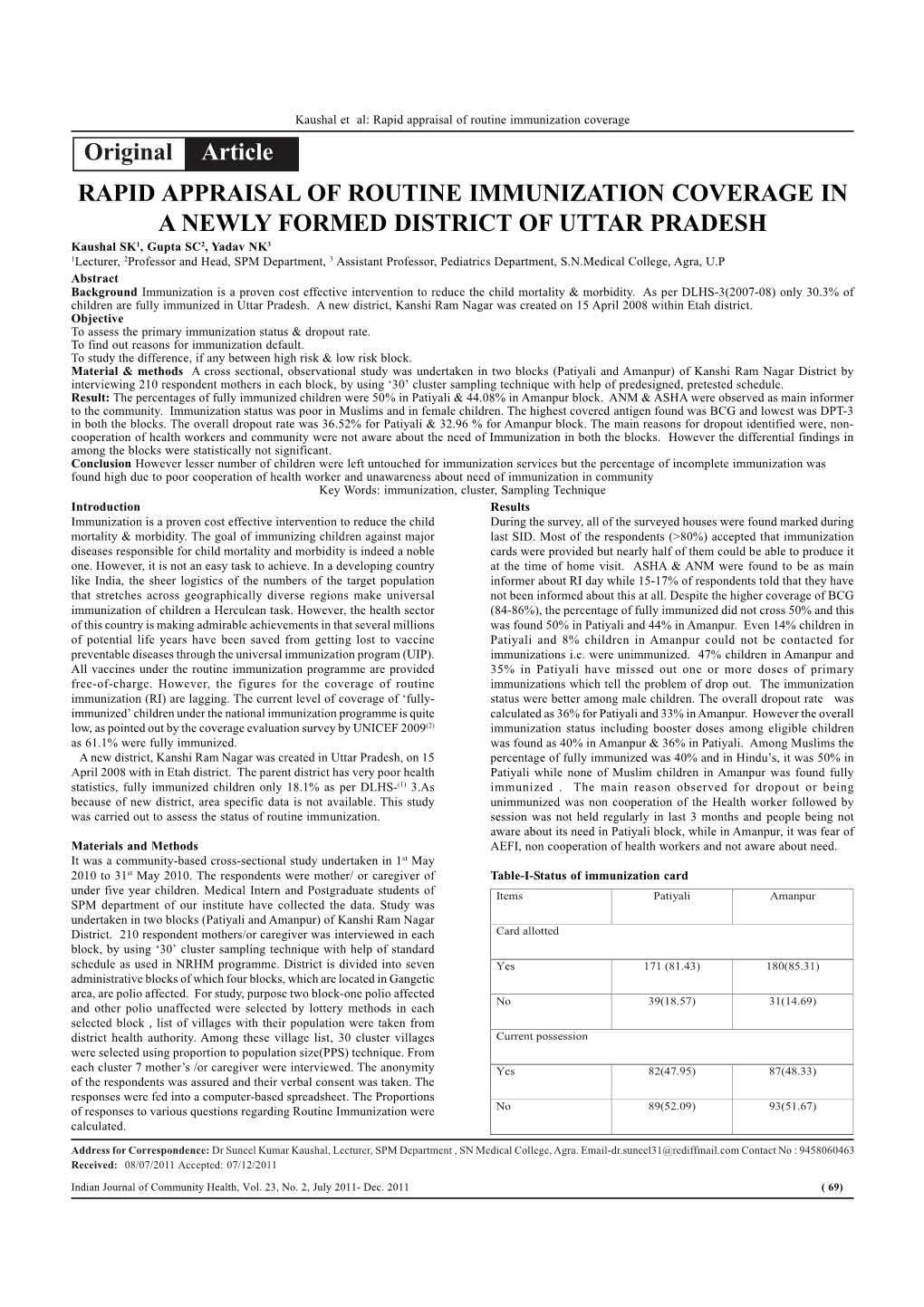
Original Article RAPID APPRAISAL of ROUTINE IMMUNIZATION
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Roll of Advocates Clerks at Kasganj.Pdf
(District Court Kasganj) (Roll of Advocates Clerks at Kasganj) Sl. ID No. Advocate Enrollment Regidencial Address Official Address Mob./Tell. Email Address NO. Name of Advocate Clerk Name No. Of No. Father/Husband's Name Advocate 1 Roll No. 0001/KSJ/2020 Deepak UP13269/19 Lalpur Nai basti mo. mohan sahawar ---- 9720488106 --- Ravi Kumar Verma S/o Chahar Singh Kumar Gate Kasganj Sharma 2 Roll No. 0002/KSJ/2020 Mo. Nishat UP01273/99 Mo. Nawab Gali Nyorian Kasganj Gali 3 Chamber 14 8958203020 ---- Shafiq Ahmad Khan S/o Khaleel Kamil Ahmad Khan 3 Roll No. 0003/KSJ/2020 Anurodh UP1353/99 Kushbihar colony Bilram gate Kasganj ---- 9568919249 ---- lalitesh Kumar S/o Leeladhar Kumar Saxena 4 Roll No. 0004/KSJ/2020 Mukesh UP8053/00 Vill Mosampur post nadrai Ps & Dist --- 9058581249 narendra9192babu@gmai Narendra Kumar S/o Ganga Singh Gupta Kasganj l.com 5 Roll No. 0005/KSJ/2020 Sarvesh UP1499/83 Vill Banupura post Amanpur Dist Gali 2 Chamber 20 7983157956 ----- Anjali D/o Satendra Kumar kumar Kasganj Gupta 6 Roll No. 0006/KSJ/2020 Pradeep UP3463/93 Durga colony Kasganj ---- 6399224696 ---- Smt. Bhudevi W/o Pradeep Kumar Kumar Kannojia 7 Roll No. 0007/KSJ/2020 Arun Kumar UP818/94 Mo. Jaijairam Gali Lodhiyan Kasganj --- 9568895404 --- Sonu S/o Ramesh Chandra Maheshwari 8 Roll No. 0008/KSJ/2020 Ayodhya UP05297/15 Vill Narouli post Kisrouli Kasganj Chamber 6 Gali 4 9830713026 ---- Rajpal Singh S/o Kanchan Singh Prasad 9 Roll No. 0009/KSJ/2020 Rajeev UP2344/01 Mo. Mohan Gali Kaysthan Post & Dist --- 8791865949 ----- Kamal Kumar S/o Ram Chandra Kumar Kasganj 10 Roll No. -

Annexure-V State/Circle Wise List of Post Offices Modernised/Upgraded
State/Circle wise list of Post Offices modernised/upgraded for Automatic Teller Machine (ATM) Annexure-V Sl No. State/UT Circle Office Regional Office Divisional Office Name of Operational Post Office ATMs Pin 1 Andhra Pradesh ANDHRA PRADESH VIJAYAWADA PRAKASAM Addanki SO 523201 2 Andhra Pradesh ANDHRA PRADESH KURNOOL KURNOOL Adoni H.O 518301 3 Andhra Pradesh ANDHRA PRADESH VISAKHAPATNAM AMALAPURAM Amalapuram H.O 533201 4 Andhra Pradesh ANDHRA PRADESH KURNOOL ANANTAPUR Anantapur H.O 515001 5 Andhra Pradesh ANDHRA PRADESH Vijayawada Machilipatnam Avanigadda H.O 521121 6 Andhra Pradesh ANDHRA PRADESH VIJAYAWADA TENALI Bapatla H.O 522101 7 Andhra Pradesh ANDHRA PRADESH Vijayawada Bhimavaram Bhimavaram H.O 534201 8 Andhra Pradesh ANDHRA PRADESH VIJAYAWADA VIJAYAWADA Buckinghampet H.O 520002 9 Andhra Pradesh ANDHRA PRADESH KURNOOL TIRUPATI Chandragiri H.O 517101 10 Andhra Pradesh ANDHRA PRADESH Vijayawada Prakasam Chirala H.O 523155 11 Andhra Pradesh ANDHRA PRADESH KURNOOL CHITTOOR Chittoor H.O 517001 12 Andhra Pradesh ANDHRA PRADESH KURNOOL CUDDAPAH Cuddapah H.O 516001 13 Andhra Pradesh ANDHRA PRADESH VISAKHAPATNAM VISAKHAPATNAM Dabagardens S.O 530020 14 Andhra Pradesh ANDHRA PRADESH KURNOOL HINDUPUR Dharmavaram H.O 515671 15 Andhra Pradesh ANDHRA PRADESH VIJAYAWADA ELURU Eluru H.O 534001 16 Andhra Pradesh ANDHRA PRADESH Vijayawada Gudivada Gudivada H.O 521301 17 Andhra Pradesh ANDHRA PRADESH Vijayawada Gudur Gudur H.O 524101 18 Andhra Pradesh ANDHRA PRADESH KURNOOL ANANTAPUR Guntakal H.O 515801 19 Andhra Pradesh ANDHRA PRADESH VIJAYAWADA -

T" (!R?J.!Fo Central State Ttebefictatry Narne of Nameof Cify/ULB No of Project S'no
St*te Urban BeveloPment AgeneY €sverslaest ef, Uttar Fra$esh Letter No. :- | 67l01 129 I]HF A-612017 -18 Dated:Z| April.20l7 Minutes of Meeting of 3d Stafe Level Appraisal Cammittee {SLAC} for Ilousing for AII held on 27.84"2fi17" Detail Project Report under "Flousing for Alf' has been appraised by the State Level Appraisal Committee {SLAC,}. After discussion, SLAC has appraised the DPR put up by the State Level Nodal Ageecy a*d regqnrue*ets thc apprcrval with fcllqtwjng s*ggg$Cc{}*: Mandatory of Adhar Card hBC Nonns to be eusured l. Summarv of 3I ,IILBs comprisine 9.363 validated BengEciaries under. Bqndficia{y Led Cegltructbn - New" wh{are egn+qnt tretter *nd la*d doeFmests was recsivqd *re g"iven beloqi Axr*unt inI,ekb S"No. Narneof Naar* af Cify/ tlLB 1S**f Prr{ect Ce*tr*l $t*te Beusficiary Distrlet E]trS Cost Share Share 5h*'re hfirse BLC-New Constr,nction I Prxapgarh turt$NP L6 I r r39.39 43CI.sS 287.S0 +L T .6Y KetraM€&igq!{NP 166 659.&2 249.** 166.*0 244.*2 j Jaiaun KadalnaNP 347 13"77,59 520-5fi 34?-*$ 510.S9 Lt K-c{ra NP 268 1S63-96 4€2SS 25S_SS 393.96 5 Muzar&inagar Jansa&iIP 1*t] 397.fiO 15S.0* t00.*0 t47.00 a ShahpurNP 226 897.22 339"0* 226.88 332.22 I Saharanprr NakurNPP 198 786.*6 297-A{J r93,*s 29t.tJb d Ti*sr ].IF ?4& 984.56 372.ffi ?48.*0 364.56 Nmai*a-l{P 2Q7 82r.79 3i*_5* 2*?,*g 344.29 '21t is BehatNF 148 5S7.56 zz2.*8 t48.C* -itl 11 Chilkana Saltangr NP 537 213I.89 8S5,50 53?.00 789.39 12 AnbehfaFeffihlP 248 9W.s6 372-08 243.0S 364.56 1? Cl*trak&oet R*jap*r.NP v*3 7162.57 439.5S 293.$0 43$.S7 It Hami+lr KuraraNF 187 741.98 280.50 rg7.0s 274.48 I5 SarilaNf ?55 1$t i.79 3*2.5* 255"0S 374.29 16 Msradabad Bhajpur [*taran]Fi:r ]{P 176 6q833 264.0S 176.*0 ?58.33 gilarilWP 268 1*63.37 4$:.$* 268rt9 393.37 1S Meerut KhtrkhodeNP 248 9S4,S1 3?2_fi* 248.S0 39.01 19 BhasumaNP tz3 488.S4 184-59 123.0S 180-54 q€lEris.st" (!r?j.!Fo Central State tteBefictatrY Narne of Nameof CifY/ULB No of Project S'No. -

Kashiram Nagar District, U.P
DISTRICT GROUND WATER BROCHURE KASHIRAM NAGAR DISTRICT, U.P. (A.A.P.: 2012-2013) By Sanjiv Kudesia Scientist 'B' CONTENTS Chapter Title Page No. DISTRICT AT A GLANCE, ETAH DISTRICT ..................3 1.0 INTRODUCTION ..................7 2.0 RAINFALL & CLIMATE ..................8 3.0 GEOMORPHOLOGY & SOIL TYPES ..................8 3.1 Geomorphology 3.2 Major Drainage 3.3 Soil Types 4.0 GROUND WATER SCENARIO ..................9 4.1 Hydrogeology 4.2 Ground Water Resources 4.3 Ground Water Quality 5.0 GROUND WATER MANAGEMENT STRATEGY ..................16 5.1 Ground Water Development 5.2 Water Conservation & Artificial Recharge 6.0 GROUND WATER RELATED ISSUES AND PROBLEMS ..................17 7.0 AWARENESS & TRAINING ACTIVITY ..................17 8.0 AREAS NOTIFIED BY CGWA/SGWA ..................17 9.0 RECOMMENDATIONS ..................18 PLATES: 1. INDEX MAP OF ETAH DISTRICT, U.P. 2. DEPTH TO WATER LEVEL, KASHIRAMNAGAR DISTRICT, U.P. (PRE- MONSOON, MAY, 2012) 3. DEPTH TO WATER LEVEL, KASHIRAMNAGAR DISTRICT, U.P. (POST-MONSOON, NOV., 2012) 4. CATEGORIZATION OF BLOCKS IN KASHIRAMNAGAR DISTRICT, U.P. 2 DISTRICT AT GLANCE, KASHIRAMNAGAR DISTRICT, U.P. 1. GENERAL INFORMATION i. Geographical Area (Sq. Km.) : 1993.08 ii. Administrative Divisions Number of Tehsil : 3 (Kasganj, Patiyali & Sahawar) Number of Block : 7 1. Sahawar, 2. Kasganj, 3. Amanpur, 4. Soron, 5. Sidhpura, 6. Ganj Dundwara, 7. Patiyal Nagar Palikas : 3 Nagar Panchayat : 7 Nyay Panchayat : 79 Gram Panchayat : 389 Number of Villages : 718 Assembly Areas : 03 iii. Population (as on 2011 census) : 1438156 Female : 672627 Male : 765529 Density : 736 person/sq.km. iv. Climatological Data Average Annual Rainfall (mm) : 722.40 Rainfall for 2011 (mm) : 482.60 Mean Maximum Temperature (0C) : 32 Mean Minimum Temperature (0C) : 26 Relative Humidity (Morning) (%) : 60 Relative Humidity (Evening) (%) : 41 Average Number of Rainy Days : 40 Wind Velocity (Km/Hr) : 4.5 Potential Evapotranspiration (mm) : 1467.20 2. -
Bareilly Zone CSC List
S Grampanchayat N District Block Name Village/CSC name Pincode Location VLE Name Contact No Village Name o Badaun Budaun2 Kisrua 243601 Village KISRUA Shailendra Singh 5835005612 Badaun Gunnor Babrala 243751 Babrala Ajit Singh Yadav Babrala 5836237097 Badaun Budaun1 shahavajpur 243638 shahavajpur Jay Kishan shahavajpur 7037970292 Badaun Ujhani Nausera 243601 Rural Mukul Maurya 7351054741 Badaun Budaun Dataganj 243631 VILLEGE MARORI Ajeet Kumar Marauri 7351070370 Badaun Budaun2 qadarchowk(R) 243637 qadarchowk sifate ali qadarchowk 7351147786 Badaun Budaun1 Bisauli 243632 dhanupura Amir Khan Dhanupura 7409212060 Badaun Budaun shri narayanganj 243639 mohalla shri narayanganj Ashok Kumar Gupta shri narayanganj 7417290516 Badaun BUDAUN1 Ujhani(U) 243639 NARAYANGANJ SHOBHIT AGRAWAL NARAYANGANJ 7417721016 Badaun BUDAUN1 Ujhani(U) 243639 NARAYANGANJ SHOBHIT AGRAWAL NARAYANGANJ 7417721016 Badaun BUDAUN1 Ujhani(U) 243639 BILSI ROAD PRADEEP MISHRA AHIRTOLA 7417782205 Badaun Vazeerganj Wazirganj (NP) 202526 Wazirganj YASH PAL 7499478130 Badaun Dahgawan Nadha 202523 Nadha Mayank Kumar 7500006864 Badaun Budaun2 Bichpuri 243631 VILL AND POST MIAUN Atul Kumar 7500379752 Badaun Budaun Ushait 243641 NEAR IDEA TOWER DHRUV Ushait 7500401211 Badaun BUDAUN1 Ujhani(R) 243601 Chandau AMBRISH KUMAR Chandau 7500766387 Badaun Dahgawan DANDARA 243638 DANDARA KULDEEP SINGH DANDARA 7534890000 Badaun Budaun Ujhani(R) 243601 KURAU YOGESH KUMAR SINGH Kurau 7535079775 Badaun Budaun2 Udhaiti Patti Sharki 202524 Bilsi Sandeep Kumar ShankhdharUGHAITI PATTI SHARKI 7535868001 -

Kasganj Dealers Of
Dealers of Kasganj Sl.No TIN NO. UPTTNO FIRM - NAME FIRM-ADDRESS 1 09125900007 KS0009108 JAJU AUTO MOBILES AMAPUR KASGANJ 2 09125900026 KS0001026 AGARWAL TREDARS SORONGET KASGANJ 3 09125900045 KS0001051 ASHOK KUMAR VINAY KUMAR NAVEEN MANDI ESTHAL KASGANJ (CLOSE) 4 09125900078 KS0002065 CHOLA BEEJ BHANDAR BILLRAM GATE KASGANJ 5 09125900083 KS0002344 DEENA NATH LAKHEM CHAND NADRAI GATE KASHGANJ 6 09125900106 KS0002850 GAYATRI DEVI B.K.O SORON KASGANJ 7 09125900111 KS0002608 GOLDAN REDIYOS NADAIGET KASGANJ 8 09125900125 KS0010264 HARI OM DHARMENDRA KUMAR SAHAWAR ETAH 9 09125900130 KS0003067 HORI LAL KISHORI LAL NAVEEN MANDI STAL KASGANJ 10 09125900144 KS0000530 KAMAL BOOT KASGANJ NADRAI GATE KASGANJ 11 09125900158 KS0015057 KISHAN KRISHI SAVA KANDRA SORON GATE KASGANJ 12 09125900163 KS0000477 KRISHANA TEA CO. NADARAI GATE KASGANJ 13 09125900182 KS0004324 MADRAS SHOE CO. NADRAI GATE KASGANJ 14 09125900205 KS0000397 MASTER JI CONFECTIONERY BILLRAM GATE KASGANJ 15 09125900210 KS0004437 MIHI LAL NEK RAM NAVEEN MANDI STAL KASGANJ 16 09125900219 KS0004538 MUNNAL LAL GUPTA NADRAI GATE KASGANJ 17 09125900257 KS0006151 RAJ STONE CO. SERCULAR ROAD KASGANJ 18 09125900262 KS0005630 RAKESH BABU AGRWAL GUR DEALER KASHGANJ 19 09125900281 KS0006163 RAMNIVAS CHHOTE LAL NAVEEN MANDI STAL KASGANJ 20 09125900295 KS0006491 SARASWATI AURVADIC BHAWAN RAILWAY RD. KASGANJ 21 09125900337 KS0007254 SURESH CHAND AGRAWAL SORON KASGANJ 22 09125900342 KS0007355 TAYAL AGRICULTURAL WORKS SORO GATE KASGANJ 23 09125900356 KS0007508 VINDHYA FARMA CITICALS SAHAV VALAYABDRA KASGANJ 24 09125900361 KS0007711 YADRAM & SONS NADRAI GATE KASHGANJ 25 09125900375 KS0009889 NAUSHEMIYAN THEKEDAR RAILWAYS ROAD KASGANJ 26 09125900394 KS0010555 AMBE ELECTRONICS NADARAIGET KASGANJ 27 09125900403 KS0009311 BASANT LAL OMPRKASH BKO. B.K.O. KASGANJ ETAH 28 09125900417 KS0011138 GUPTA GASS AGENCY NADARIGET KASGANJ ETAH 29 09125900422 KS0011708 BHUMBHI RAJ SINGH K.A. -

Interventions by Swachhagrahis & FLW Post CAB Orientation
Interventions by Swachhagrahis & FLW post CAB orientation Shashi Bala Saroj, a Swachhagrahi and Anganwadi worker of Narayanpur Buzurd GP in Puranpur Block of Pilibhit District in UP has been working towards addressing the gender gap in COVID-19 vaccination. Owing to her efforts in sensitizing people, as many as 138 individuals were vaccinated, of which 80 were women. The frontline worker (FLW) aims to get the whole community vaccinated soon and, in this regard, has been visiting homes to generate awareness and motivate people to get vaccinated. Realising that there was a huge gender gap in vaccination, she has increased focus on women, motivating them to get the jab and overcome their fears. She has helped with the entire process including accompanying many of them to the vaccination centre. Ms. Shashi Bala Saroj was one of the 15,406 Swachhagrahis and frontline workers (FLW) who attended an online orientation on COVID appropriate behaviours (CAB), its containment and management in rural areas. The grassroot workers were trained on the entire process - beginning from house-to-house surveillance to adherence to the cremation protocols. The online training was organised by UNICEF in collaboration with the Department of Panchayat Raj, UP from 18 May to 4 June 2021. Participants included Swachhagrahis, ASHA, ANM, schoolteachers, and district SBM(G) team who attended sessions chaired by Nodal Officer PRD-UP and respective Divisional Deputy Director (Panchayat) and facilitated by UNICEF and PRD state team. State officials have attributed the increase in people coming forward to take the vaccine to the Swachhagrahis who helped bring positivity and acceptance of the vaccine in the rural areas. -

Evaluation of Socio-Economic Development in Small Areas Was Undertaken by Indian Society of Agricultural Statistics, New Delhi
PROJECT REPORT Evaluation of Socio- Economic Development in Small Areas 9 . %+$7,$ 6 & 5$, SPONSORED BY PLANNING COMMISSION GOVERNMENT OF INDIA, NEW DELHI INDIAN SOCIETY OF AGRICULTURAL STATISTICS IASRI Campus, Library Avenue, Pusa New Delhi - 110 012 2003 - 2004 PREFACE A research project on Evaluation of Socio-economic Development in Small Areas was undertaken by Indian Society of Agricultural Statistics, New Delhi. Development is a process, which improves the quality of life. It requires a balanced human resource development in the country. Development of social sector along with technology absorption in agriculture could be considered as the primary objective of any economic developmental effort. The developmental programmes have been taken up in the country in a planned way with the main objective of enhancing the quality of life of people by providing the basic necessities as well as effecting improvement of economic well being. Economic regeneration attempted in successive Five Year Plans has made agriculture a pride of the country’s economy. This sector today provides livelihood to about 70 per cent of the labour force. Major objective of rural development has been the alleviation of poverty in the rural areas. The programmes for rural development have to be specific in its objectives to bring about a directional change and uniform agricultural development. The present study deals with the evaluation of the levels of development in agriculture, infrastructural facilities and overall socio-economic fields by constructing the composite index of development at community development block level in the state of Uttar Pradesh. For this study, the blocks have been taken as the unit of analysis. -

Designation Mobile No Office Phone Res. Phone Posting Place
3/9/2015 CUG NO Details BACK Home Print Close Please choose your Sorting For Full List option /Search Option : Designation Mobile No Office Phone Res. Phone Posting Place To Search a Name of the Post (Officer Particular BDO Full List Designation) Designation To Search a Particular Name Enter min 3 char. of Designation/Mobile No/Office Phone/Res. Phone/Posting Place Search CUG Office Residence S.No. Division District Officer Designation Fax No Posting Place Mobile No Phone Phone 1 AGRA MATHURA BDO Nandgaon 9454464521 NanadGaon 2 AGRA MATHURA BDO chhata 9454464522 Chhata 3 AGRA MATHURA BDO Chaumuha 9454464523 Chaumuha 4 AGRA MATHURA BDO Naujhil 9454464524 Naujhil 5 AGRA MATHURA BDO Mant 9454464525 Mant 6 AGRA MATHURA BDO Raya 9454464526 Raya 7 AGRA MATHURA BDO Goverdhan 9454464527 Goverdhan 8 AGRA MATHURA BDO Mathura 9454464528 Mathura 9 AGRA MATHURA BDO Mathura 9454464528 Mathura 10 AGRA MATHURA BDO Farah 9454464529 Farah 11 AGRA MATHURA BDO Farah 9454464529 Farah 12 AGRA MATHURA BDO Baldeo 9454464530 Baldeo Mathura 13 AGRA FEROZABAD BDO 9454464496 0 0 0 Firozabad 14 AGRA FEROZABAD BDO 9454464498 0 0 0 Eka 15 AGRA FEROZABAD BDO 9454464502 0 0 0 Jasarana 16 AGRA FEROZABAD BDO 9454464504 0 0 0 Araw 17 AGRA FEROZABAD BDO 9454464505 0 0 0 Madanpur 18 AGRA FEROZABAD BDO 8004418144 0 0 0 Araw 19 AGRA FEROZABAD BDO 9411411519 0 0 0 Jasarana 20 AGRA FEROZABAD BDO 9556266188 0 0 0 Eka 21 AGRA FEROZABAD BDO 9557340940 0 0 0 Shikohabad 05672 22 AGRA MAINPURI BDO Mainpuri 9410675800 Block MAINPURI 235844 05672 23 AGRA MAINPURI BDOKURAWALI 9415609022 -

Etah Dealers Of
Dealers of Etah Sl.No TIN NO. UPTTNO FIRM - NAME FIRM-ADDRESS 1 09125800003 EH0080175 RAJ TRACTORS G.T.ROAD ETAH 2 09125800017 EH0094994 NAU BHARAT MACHINARY STORE SIDPURA ETAH 3 09125800022 EH0078434 SINGH SERVICE STATION G.T.ROAD ETAH 4 09125800036 EH0037589 ANIL COAL DEPOT (CLOSED) JALESAR ETAH 5 09125800041 EH0048228 ASHOK ARMS STORE POST OFFICE ROAD ETAH 6 09125800055 EH0025842 BANGALI BABU GUPTA MAIN GANJ ETAH 7 09125800060 EH0045473 BHAGWAN SINGH SATY PRAKASH NAVEEN MANDI ETAH (CLOSE) 8 09125800069 EH0046463 BRAHMA NAND GUPTA K.A. NEW GALLA MANDI ETAH 9 09125800074 EH0075807 CHACHA AJENCY MARHERA ETAH 10 09125800093 EH0047376 DHARAM PAL LAKHAN SINGH NEW MANDI STAL ETAH 11 09125800102 EH0071859 DURGA TRADE CORPORATION JALESAR ETAH 12 09125800116 EH0045384 GULAB CHANDRA JAIN KIRANA KIRANA MARKET ETAH 13 09125800121 EH0048616 GUPTA BOOK STORE MIRHASHI ETAH 14 09125800135 EH0045804 HAZI MOHAISMIL BHARGAN ETAH 15 09125800140 EH0048354 JAGDISH PRASAD JAIN KIRANA MAINGANJ ETAH 16 09125800149 EH0075718 JAI SHIV BRICK FIELD NAGLA GOPAL ETAH 17 09125800154 EH0075403 JAIN TRADERS SABJEE MANDI ETAH 18 09125800168 EH0017478 KHAMANI RAM HARI SHANKAR MAINGANJ GAHNTAGHAR ETAH 19 09125800173 EH0070529 KOHALI PRINTING PRESS GANDHI MARKET ETAH 20 09125800187 EH0074664 MADAN TRADING COMPANY JALESAR ETAH 21 09125800192 EH0074296 MAHESH CHANDRA GUPTA ARTI NAVEEN MANDI STAL ETAH 22 09125800201 EH0041893 MOHD. ISHAQ MOHD. BASHIR MAINGANJ ETAH 23 09125800215 EH0076001 NATIONAL ARMS DELEAR MARHERA ETAH 24 09125800220 EH0046653 NAVEEN GLASS WORKS JALASER -
Advocate Roll, District Kasganj Dated 06.03.2020
(District Court Kasganj) (Provisional Roll of Advocates at Kasganj) Sl. Roll No. Enrollment Date of Residential Address Official Address Mob./Tell. No. Email Address NO. Name of Advocate No./Year Enrollmen Father/Husband's Name Council t 1 Roll No. KSJ/0001/2020 UP2508/82 08-05-82 Mo. Vioparian sahawar dist Kasganj First wing seat (Chamber) 9927325308 -- Mo. Nabi Qureshi S/o Mo. Ibrahim 2 Roll No.KSJ/0002/2020 UP07447/08 14-12-08 Mo. Jaijairam (Ahirpara) Kasganj Chanmber No. 19 Gali No. 2 9917883531 rahulsharma15@hotmai Rahul Sharma S/o Sri Vinod kumar Pin 207123 Dist. Court Kasganj n.com Sharma 3 Roll No. KSJ/0003/2020 UP1601/98 29-04-98 Vill. Lalupura post kachhera Dist. ---- 9758078487 --- Hari Om S/o Sri Kishan lal Kasganj 4 Roll No. KSJ/0004/2020 UP13269/19 14-12-19 Mo. Mohanlalpur Nai basti sahawar Gali No. 7 Chamber NO. 17 7906330080 deepsharma7906@gmail Deepak kumar S/o Late Sri Ram gate kasganj 207123 dist. Court kasganj .com Khiladi 5 Roll No. KSJ/0005/2020 UP5316/82 10-10-82 3B Shartri Nagar Etah Gali No. 3 Chamber No. 7 8279776773 --- Veerpal Singh Solanki S/o Late Sri Dist. Court Kasganj Chattarpal Singh 6 Roll No. KSJ/0006/2020 UP14061/00 26-11-00 Vill Dariyabganj post thana ---- 9319952091 santoshkradvocate2091 Santosh Kumar S/o Kanhi Lal Dariyabganj kasganj 207243 8630936301 @gmail.com 7 Roll No. KSJ/0007/2020 UP3421/10 28-03-10 Mo. Qvazi sahawar Kasganj ---- 8865859971 asiyachisti78660@mail. Asiya chishti D/o Abdul Rauf Chishti com 8 Roll No. -

District Kasganj (Kanshiram Nagar)
DSR - KASGANJ District Kasganj (Kanshiram Nagar) 1. Introduction: Kasganj is the 71st district in the Indian state of Uttar Pradesh. The district and particularly the city Kasgaj is popularly ko as eause it as estalished i a thik forest of kas. Kasgaj as also ko as Taay or Khasgaj durig Mughal ad British period. Kasgaj oes i the Aligarh division jurisdiction. KasganjDistrict was created on April 17, 2008 by dividing Etah district and is renamed as Kanshiram Nagar. Popular area of the district includes Nadri, Soron, Patiali. Kasganj the newly created district is among the four districts of Aligarh Division. Kasganj includes three Tehsils Kasganj, SahavarandPatiali. Kasganj is located at 27.82°N latitude 78.65°E longitude. It has an average elevation of 177 metres. Situated on the banks of river Kali, the town is in proximity of the Himalayan foothills. It is located in the Doab, the area between the holy rivers Ganges and Yamuna and the alluvium soil makes the land one of the most fertile regions. A large number of surrounding villages depend on agriculture and related economic activities. Area of Kasganj District is 1993.08 sq km and is at 68th place in Uttar Pradesh in terms of area of the district. The rural area covers 1918.2 Sq Km and urban recorded 75.6 Sq. Km. There are 389 Gram Panchayats and 715 revenue villages with 650 inhabited and 65 un-inhabited villages. The percentage share of urban population in the district is 20.1% as against 22.3% of the population in urban areas of the state.