ND Physician June 2015
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

2016 Lilly Report of Political Financial Support
16 2016 Lilly Report of Political Financial Support 1 16 2016 Lilly Report of Political Financial Support Lilly employees are dedicated to innovation and the discovery of medicines to help people live longer, healthier and more active lives, and more importantly, doing their work with integrity. LillyPAC was established to work to ensure that this vision is also shared by lawmakers, who make policy decisions that impact our company and the patients we serve. In a new political environment where policies can change with a “tweet,” we must be even more vigilant about supporting those who believe in our story, and our PAC is an effective way to support those who share our views. We also want to ensure that you know the story of LillyPAC. Transparency is an important element of our integrity promise, and so we are pleased to share this 2016 LillyPAC annual report with you. LillyPAC raised $949,267 through the generous, voluntary contributions of 3,682 Lilly employees in 2016. Those contributions allowed LillyPAC to invest in 187 federal candidates and more than 500 state candidates who understand the importance of what we do. You will find a full financial accounting in the following pages, as well as complete lists of candidates and political committees that received LillyPAC support and the permissible corporate contributions made by the company. In addition, this report is a helpful guide to understanding how our PAC operates and makes its contribution decisions. On behalf of the LillyPAC Governing Board, I want to thank everyone who has made the decision to support this vital program. -

MCF CONTRIBUTIONS JULY 1 - DECEMBER 31, 2016 Name State Candidate Amount U.S
MCF CONTRIBUTIONS JULY 1 - DECEMBER 31, 2016 Name State Candidate Amount U.S. House Robert Aderholt for Congress AL Rep. Robert Aderholt $2,000 ALABAMA TOTAL U.S. House Crawford for Congress AR Rep. Rick Crawford $1,500 Womack for Cogress Committee AR Rep. Stephen Womack $500 ARKANSAS TOTAL U.S. House Kyrsten Sinema for Congress AZ Rep. Kyrtsen Sinema $500 ARIZONA TOTAL U.S. House Denham for Congress CA Rep. Jeff Denham $1,500 Garamendi for Congress CA Rep. John Garamendi $500 Kevin McCarthy for Congress CA Rep. Kevin McCarthy $1,000 Valadao for Congress CA Rep. David Valadao $1,500 U.S. House Leadership Majority Committee PAC--Mc PAC CA Rep. Kevin McCarthy $5,000 State Assembly Adam Gray for Assembly 2016 CA Assm. Adam Gray $1,500 Catharine Baker for Assembly 2016 CA Assm. Catharine Baker $2,500 Cecilia Aguiar-Curry for Assembly 2016 CA Assm. Cecilia Aguiar-Curry $2,000 Chad Mayes for Assembly 2016 CA Assm. Chad Mayes $2,000 James Gallagher for Assembly 2016 CA Assm. James Gallagher $1,500 Patterson for Assembly 2016 CA Assm. James Patterson $2,000 Jay Obernolte for Assembly 2016 CA Assm. Jay Obernolte $1,500 Jim Cooper for Assembly 2016 CA Assm. Jim Cooper $1,500 Jimmy Gomez for Assembly 2016 CA Assm. Jimmy Gomez $1,500 Dr. Joaquin Arambola for Assembly 2016 CA Assm. Joaquin Arambula $1,500 Ken Cooley for Assembly 2016 CA Assm. Ken Cooley $1,500 Miguel Santiago for Assembly 2016 CA Assm. Miguel Santiago $1,500 Rudy Salas for Assembly 2016 CA Assm. -

Revised Meeting Notice
15.5171.01000 September 2, 2014 REVISED MEETING NOTICE Representative Chet Pollert, Chairman, has called a meeting of the BUDGET SECTION. Date: Wednesday, September 24, 2014 Time: 9:30 a.m. Place: Senate Chamber, State Capitol, Bismarck Agenda: Presentations by representatives of the Office of Management and Budget regarding the status of the general fund, revised 2013-15 biennium and preliminary 2015-17 biennium revenue forecasts, key economic indicators, irregularities in the fiscal practices of the state, employees receiving bonuses above the 25 percent limitation, tobacco settlement proceeds, and federal grant applications; by state agency representatives regarding Emergency Commission requests; by representatives of the Game and Fish Department on approval of land purchases; by representatives of the Department of Corrections and Rehabilitation on prison population, inmate admissions, and the number of inmates not admitted; by representatives of the Department of Human Services regarding transfers between line items or subdivisions; by representatives of the State Fire Marshal on income and expenditures of fire departments and reserve fund balances; by representatives of the Information Technology Department regarding the department's annual report; by the Legislative Council staff of the 2014 North Dakota Finance Facts, on the status of the state's federal funds receipts on block grant hearings required during the 2015 legislative session, and a resolution draft authorizing the Budget Section to hold any required legislative block -

3Rd DAY WEDNESDAY, DECEMBER 8, 2010 15 Third Day of Legislative
3rd DAY WEDNESDAY, DECEMBER 8, 2010 15 Third Day of Legislative Organizational Session JOURNAL OF THE HOUSE Sixty-second Legislative Assembly * * * * * Bismarck, December 8, 2010 The House convened at 8:30 a.m., with Speaker Drovdal presiding. The prayer was offered by Pastor Keith Ritchie, Cornerstone Community Church, Bismarck. The roll was called and all members were present except Representatives Dahl, R. Kelsch, and Zaiser. A quorum was declared by the Speaker. MOTION REP. VIGESAA MOVED that the House stand in recess until 9:10 a.m., which motion prevailed. THE HOUSE RECONVENED pursuant to recess taken, with Speaker Drovdal presiding. ANNOUNCEMENT SPEAKER DROVDAL ANNOUNCED that the House would be on the Seventh Order of business. The Chief Clerk read the Committee on Committees assignments. 2011 HOUSE STANDING COMMITTEES Appropriations Committee Committee Chairman - Jeff Delzer Vice Chairman - Keith Kempenich Education and Environment Division Committee Chairman - Bob Skarphol Clark Williams Vice Chairman - Kathy Hawken Dave Monson Mark Dosch Bob Martinson Government Operations Division Committee Chairman - Blair Thoreson Eliot Glassheim Vice Chairman - Matt Klein Joe Kroeber Keith Kempenich Mike Brandenburg Stacey Dahl 16 JOURNAL OF THE HOUSE 3rd DAY Human Resources Division Committee Chairman - Chet Pollert Lee Kaldor Vice Chairman - Larry Bellew Ralph Metcalf Gary Kreidt Jon Nelson Alon Wieland Education Committee Committee Chairman - RaeAnn Kelsch Lyle Hanson Vice Chairman - Lisa Meier Bob Hunskor Brenda Heller Corey Mock Dennis Johnson Phillip Mueller Karen Karls David Rust Mike Schatz John Wall Joe Heilman Karen Rohr Mark Sanford Finance and Taxation Committee Committee Chairman - Wesley Belter Scot Kelsh Vice Chairman - Craig Headland Shirley Meyer Glen Froseth Lonny Winrich Bette B. -

2021 FPA-ND Legislative Scorecard
2021 NORTH DAKOTA LEGISLATIVE REPORT CARD 67th LEGISLATIVE SESSION ABOUT THE SCORECARD We are pleased to share this scorecard for the 2021 North Dakota state legislative session. This is a snapshot of how lawmakers voted on key social and moral legislation related to life, education, family, religious freedom, and similar issues. Guided by our mission of building a state where God is honored, religious freedom flourishes, families thrive, and life is cherished, the scorecard focuses on seven bills. This scorecard is not an endorsement of any candidate or political party. It does not measure any lawmakers’ integrity, commitment to their faith, work ethic, or rapport with Family Policy Alliance of North Dakota. It is only a report on how each lawmaker voted. Please continue to hold our legislators accountable for their voting records and please pray that they may always vote in ways that uphold your biblical values as they make important decisions for our state. Sincerely, Mark Jorritsma Executive Director, Family Policy Alliance of North Dakota HOW WE FIGURED THE GRADES A bill is typically passed by a simple majority in the Senate (24 votes out of 47 senators) and the House (48 votes out of 94 Representatives.) Lawmakers earned percentage grades ranging from 0% to 100%, based upon dividing the candidate’s number of good votes cast by the number of total bills he/she voted on. The higher the score, the better their ranking. Not all lawmakers voted on every bill; the number of absences on these key bills is also noted and we encourage you to review whether your legislator actually voted on these important bills. -

Labor Townhall Posters 1-8-18.Xlsx
Official District Party 2013 2015 2017 Representative 60% 83% 48% Andrew 3 R Maragos Representative 0% 8% 17% Rosco Streyle 3 R Senator Oley 25% 9% 17% Larsen 3 R Official District Party 2013 2015 2017 Representative 26% Terry B. Jones 4 R Representative 27% Bill Oliver 4 R Senator Jordan Kannianen 4 R Official District Party 2013 2015 2017 Representative 0% 8% 4% Roger Brabandt 5 R Representative 0% 8% 17% Scott Louser 5 R Senator Randall 25% 36% 25% Burckhard 5 R Official District Party 2013 2015 2017 Representative 30% 27% 18% Dick Anderson 6 R Representative 26% Craig A. 6 R Johnson Senator Shawn Vedda 6 R Official District Party 2013 2015 2017 Representative 0% 16% 18% Rick Becker 7 R Representative 0% 25% 22% Jason Dockter 7 R Senator Nicole 25% 36% 83% Poolman 7 R Official District Party 2013 2015 2017 Representative 0% 25% 22% Jeff Delzer 8 R Representative 30% 25% 30% Vernon Laning 8 R Senator Howard 25% 27% 50% Anderson 8 R Official District Party 2013 2015 2017 Representative 100% 100% 91% Tracy Boe 9 D Representative 100% 100% 86% Marvin Nelson 9 D Senator Richard 100% 100% 83% Marcellais 9 D Official District Party 2013 2015 2017 Representative 100% 100% 100% Ron Guggisberg 11 D Representative 95% Gretchen 11 D Dobervich Senator Tim 100% 91% 100% Mathern 11 D Official District Party 2013 2015 2017 Representative 0% 10% 22% Kim Koppelman 13 R Representative 8% 14% Christopher 13 R Olson Senator Judy 63% 54% 83% Lee 13 R Official District Party 2013 2015 2017 Representative 50% 42% 48% Jon Nelson 14 R Representative 10% 16% 22% Robin Weisz 14 R Senator Jerry 13% 0% 67% Klein 14 R Official District Party 2013 2015 2017 Representative 5% Andrew 16 R Marschall Representative 0% 9% 18% Ben Koppelman 16 R Senator David a. -
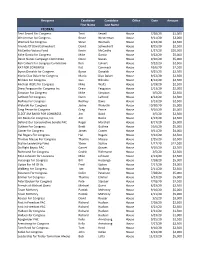
2020 PAC Contributions.Xlsx
Recipient Candidate Candidate Office Date Amount First Name Last Name FEDERAL Terri Sewell For Congress Terri Sewell House 7/28/20 $1,000 Westerman for Congress Bruce Westerman House 9/11/20 $3,000 Womack for Congress Steve Womack House 9/22/20 $2,500 Friends Of David Schweikert David Schweikert House 8/25/20 $2,500 McCarthy Victory Fund Kevin McCarthy House 1/27/20 $20,000 Mike Garcia for Congress Mike Garcia House 9/22/20 $5,000 Devin Nunes Campaign Committee Devin Nunes House 9/10/20 $5,000 Ken Calvert For Congress Committee Ken Calvert House 9/22/20 $2,500 KAT FOR CONGRESS Kat Cammack House 10/6/20 $2,500 Byron Donalds for Congress Byron Donalds House 9/25/20 $2,500 Mario Diaz‐Balart for Congress Mario Diaz‐Balart House 9/22/20 $2,500 Bilirakis For Congress Gus Bilirakis House 8/14/20 $2,500 Michael Waltz for Congress Mike Waltz House 3/19/20 $2,500 Drew Ferguson for Congress Inc. Drew Ferguson House 2/13/20 $2,000 Simpson For Congress Mike Simpson House 3/5/20 $2,500 LaHood For Congress Darin LaHood House 8/14/20 $2,500 Rodney For Congress Rodney Davis House 3/13/20 $2,500 Walorski For Congress Jackie Walorski House 10/30/20 $5,000 Greg Pence for Congress Greg Pence House 9/10/20 $5,000 ELECT JIM BAIRD FOR CONGRESS Jim Baird House 3/5/20 $2,500 Jim Banks for Congress, Inc. Jim Banks House 2/13/20 $2,500 Defend Our Conservative Senate PAC Roger Marshall House 8/17/20 $5,000 Guthrie For Congress Brett Guthrie House 10/6/20 $5,000 Comer for Congress James Comer House 9/11/20 $4,000 Hal Rogers For Congress Hal Rogers House 9/22/20 $2,500 -

Final Environmental Assessment
ENVIRONMENTAL ASSESSMENT PROPOSAL OF CRITICAL HABITAT FOR THE NORTHERN GREAT PLAINS BREEDING POPULATION OF PIPING PLOVERS (Charadrius melodus) Prepared by U.S. Fish and Wildlife Service South Dakota Ecological Services Field Office Pierre, South Dakota June 2002 Table of Contents 1.0 Purpose for the Proposed Action ...............................................1 2.0 Need for the Action......................................................1 2.1 Background ................................................2 2.2 Critical Habitat..............................................5 3.0 Description of Alternatives ................................................6 3.1 Alternative Considered But Not Fully Evaluated ...................7 3.2 Alternative A. No Action Alternative............................7 3.3 Action Alternatives ..........................................7 3.3.1 Alternative B. Designation as Identified in the Proposed Rule Proposed Action ................................10 3.3.2 Alternative C. Essential Habitat Identified in the 1988 Great Lakes and Northern Great Plains Piping Plover Recovery Plan....16 3.3.3 Alternative D. Essential Habitat Identified in the 1994 Technical/Agency Draft Revised Recovery Plan on the Great Lakes and Northern Great Plains ...........................17 3.4 Table 1. Summary of Actions by Alternative.....................21 4.0 Description of the Affected Environment.....................................24 4.1 Physical Environment .......................................24 4.2 Fish and Wildlife...........................................25 -

Contest County Name Party Mailing Address Email / Web Phone
Contest County Name Party Mailing Address Email / Web Phone Representative in Congress Kelly Armstrong Republican 1515 Burnt Boat Dr Ste C #112 [email protected] (701) 471-6036 Bismarck ND 58503 armstrongnd.com Representative in Congress Steven James Peterson Libertarian 2808 HICKORY ST N [email protected] (701) 936-4362 FARGO ND 58102-1715 stevenjamespeterson.com Representative in Congress Zach Raknerud Democratic-NPL 304 5th St NW [email protected] Minot ND 58703 https://www.ZachForND.com Representative in Congress Roland Clifford Riemers Democratic-NPL 1024 UNIVERSITY AVE [email protected] (701) 317-1803 PO Box 14702 GRAND FORKS ND 58208 State Senator David S Rust Republican PO BOX 1198 [email protected] (701) 216-0270 District 02 TIOGA ND 58852-1198 State Senator Lisa Finley-DeVille Democratic-NPL 13 1ST AVE NE (701) 421-8020 District 04 PO Box 501 MANDAREE ND 58757 State Senator Jordan Kannianen Republican 8011 51ST ST NW [email protected] (701) 421-8813 District 04 STANLEY ND 58784-9562 State Senator Morris Holen Jr Democratic-NPL PRAIRIE VIEW ACRES #8 [email protected] (701) 228-3345 District 06 BOTTINEAU ND 58318 State Senator Shawn Vedaa Republican PO BOX 550 (701) 721-5346 District 06 VELVA ND 58790-0550 State Senator Howard C Anderson Jr Republican 2107 7TH ST NW [email protected] (701) 448-2235 District 08 TURTLE LAKE ND 58575-9667 State Senator Charlie Hart Democratic-NPL 15983 100TH ST NE (701) 520-2750 District 10 PEMBINA ND 58271-9712 State Senator Janne Myrdal Republican PO Box 153 (701) 331-0946 -

2019 NORTH DAKOTA LEGISLATIVE REPORT CARD 66Th LEGISLATIVE SESSION DEAR FRIENDS
2019 NORTH DAKOTA LEGISLATIVE REPORT CARD 66th LEGISLATIVE SESSION DEAR FRIENDS, I am pleased to share this report card for the most recent North Dakota state legislative session. Here is a snapshot of how lawmakers voted on key social and moral legislation related to the right to life, education, family, marriage and other issues. Guided by our mission of building a state where God is honored, religious liberty flourishes, families thrive, and life is cherished, this report card focuses on seven bills/resolutions (hereafter collectively called bills) in the North Dakota Senate and House of Representatives during the 2019 Legislative Session. All these are included in this report card. A bill is passed by a simple majority in the Senate (24 votes out of 47 senators) and the House (48 votes out of 94 Representatives.) Lawmakers earned percentage grades ranging from 0% to 100%, based on how they voted on the relevant bills coming before their chamber. This report card is not an endorsement of any candidate or political party. It does not measure any lawmakers’ integrity, commitment to their faith, work ethic, or rapport with Family Policy Alliance of North Dakota. It is only a report on how each lawmaker voted. One of the most common questions people ask is, “How did my legislator vote?” This report card should help you answer that question. Sincerely, Mark Jorritsma Executive Director, Family Policy Alliance of North Dakota CONTENTS Introduction Letter 2 About the Report Card 3 Bill and Resolution Descriptions 4 Legislator Votes 5-7 – 2 – ABOUT THE REPORT CARD Family Policy Alliance of North Dakota selected votes on key legislation from the North Dakota Senate and North Dakota House of Representatives based on our core belief in promoting, protecting, and strengthening traditional family values. -

2016 Political Contributions
January 1 - June 30 2016* Name Candidate Amount PAC Name ALABAMA Alabama House Democratic Caucus $ 1,000.00 Johnson & Johnson State Party Committee ARIZONA Arizona Republican Party Federal Account $ 2,500.00 J&J PAC State Party Committee Arizona State Democratic Central Executive Committee $ 2,500.00 J&J PAC State Party Committee CALIFORNIA Anna Eshoo for Congress Rep. Anna G. Eshoo (D) $ 2,000.00 J&J PAC Federal House California Issues Forum $ 15,000.00 Johnson & Johnson Devin Nunes Campaign Committee Rep. Devin G. Nunes (R) $ 1,000.00 J&J PAC Federal House Dr. Raul Ruiz for Congress Rep. Raul Ruiz (D) $ 2,500.00 J&J PAC Federal House Eggman for Assembly Assm. Susan Talamantes Eggman (D) $ 1,500.00 Johnson & Johnson State House/Assembly Jeff Stone for Senate 2018 Sen. Jeff Stone (R) $ 2,000.00 Johnson & Johnson State Senate Joaquin Arambula for Assembly 2016 Joaquin Arambula (D) $ 1,000.00 Johnson & Johnson State House/Assembly Majority Committee PAC‐‐Mc PAC Rep. Kevin Owen McCarthy (R) $ 5,000.00 J&J PAC Federal Leadership PAC Royce Campaign Committee Rep. Edward Randall Royce (R) $ 3,500.00 J&J PAC Federal House Scott Peters for Congress Rep. Scott H. Peters (D) $ 2,000.00 J&J PAC Federal House Victory in November Election PAC (VINEPAC) Rep. Michael C. Thompson (D) $ 5,000.00 J&J PAC Federal Leadership PAC Walters for Congress Rep. Mimi K. Walters (R) $ 1,000.00 J&J PAC Federal House FLORIDA Friends of Dena Dena Marie Minning (D) $ 1,000.00 J&J PAC Federal House GEORGIA Collins for Congress Rep. -

1St DAY MONDAY, DECEMBER 3, 2012 1 Organizational And
Page 1 1st DAY MONDAY, DECEMBER 3, 2012 1 Organizational and Orientation Session JOURNAL OF THE HOUSE Sixty-third Legislative Assembly * * * * * Bismarck, December 3, 2012 The House convened at 1:00 p.m., with Speaker Drovdal presiding. The prayer was offered by Pastor Paul Gibson, First Baptist Church, Bismarck. COMMUNICATION FROM SECRETARY OF STATE ALVIN A. JAEGER In accordance with Section 54-03-03 of the North Dakota Century Code, I certify the enclosed list is a true and correct record of members of the House elected in the General Election held on November 6, 2012. Each member was issued a Certificate of Election (copies enclosed) after the State Canvassing Board certified the results of the election on November 16, 2012. The Certificates of Election were prepared by the Secretary of State and signed by the Governor, Secretary of State, and the Clerk of the Supreme Court (as member of the State Canvassing Board), as prescribed in North Dakota Century Code Sections 16.1-15-45 and 16.1-15-46. In addition, in accordance with Section 4, Article XI, of the North Dakota Constitution, an Oath of Office (or affirmation) form was provided to each Representative, with instructions to execute the Oath before a Notary Public and file it with the Secretary of State before he or she assumes the duties of their office. IN TESTIMONY WHEREOF, I have set my hand and affixed the Great Seal of the State of North Dakota at the Capitol in the City of Bismarck on this date. 63rd Legislative Assembly Representatives Elected - General Election, November 6, 2012 MEMBER DISTRICT NUMBER Davis S.