Feminizing Hormone Therapy for Adolescents
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Progestin-Only Systemic Hormone Therapy for Menopausal Hot Flashes
EDITORIAL Progestin-only systemic hormone therapy for menopausal hot flashes Clinicians treating postmenopausal hot flashes often recommend “systemic estrogen treatment.” However, progestin-only therapy also can effectively treat hot flashes and is an option for women with a contraindication to estrogen therapy. Robert L. Barbieri, MD Editor in Chief, OBG MANAGEMENT Chair, Obstetrics and Gynecology Brigham and Women’s Hospital Boston, Massachusetts Kate Macy Ladd Professor of Obstetrics, Gynecology and Reproductive Biology Harvard Medical School he field of menopause medi- women. In one study, 133 postmeno- in postmenopausal women with cine is dominated by studies pausal women with an average age an American Heart Association risk T documenting the effective- of 55 years and approximately 3 years score greater than 10% over 10 years.3 ness of systemic estrogen or estro- from their last menstrual period were Additional contraindications to sys- gen-progestin hormone therapy for randomly assigned to 12 weeks of temic estrogen include women with the treatment of hot flashes caused treatment with placebo or micronized cardiac disease who have a throm- by hypoestrogenism. The effective- progesterone 300 mg daily taken at bophilia, such as the Factor V Leiden ness of progestin-only systemic bedtime.1 Mean serum progesterone mutation.4 hormone therapy for the treatment levels were 0.28 ng/mL (0.89 nM) and For women who are at high risk of hot flashes is much less studied 27 ng/mL (86 nM) in the women taking for estrogen-induced cardiovascu- and seldom is utilized in clinical placebo and micronized progesterone, lar events, micronized progesterone practice. -

Informed Consent for Feminizing Hormone Therapy
Informed Consent for Feminizing Hormone Therapy For _________________________ Date of Birth: _____________ Name Used: ____________________ Patient Name as listed in chart Name if different from chart This form will assist you (and your guardian) to think through the expected effects of hormone therapy including possible unwanted side effects. You are encouraged to talk about this treatment with your medical provider and decide if hormone therapy is right for you (your child). By signing this form, you are stating that you have discussed the effects and risks of this medication with your medical provider or a member of the medical team and that you understand and accept these effects and possible risks. You (and your guardian) may ask questions and talk about any concerns you have related to this treatment at any time in this process. Estrogen (usually estradiol) is used to feminize the body (make it look more traditionally female). This medical treatment will reduce some male features and increase some female features of the body. Androgen (testosterone) blockers further decrease the amount of and/or block the effect of testosterone and masculinization of the body. Your medical provider will help decide which form and the amount of estrogen (shots, pills, gels, patches) and androgen blockers (pills, gels, shots, implanted) that are best for you based on your personal needs and any medical or mental health conditions you might have. Each person’s body responds to estrogen differently and it is hard to promise or predict with certainty how each person may respond to treatment. Your medical provider will talk with you throughout the treatment and will help you achieve the best results safely. -

A Guide to Feminizing Hormones – Estrogen
1 | Feminizing Hormones A Guide to Feminizing Hormones Hormone therapy is an option that can help transgender and gender-diverse people feel more comfortable in their bodies. Like other medical treatments, there are benefits and risks. Knowing what to expect will help us work together to maximize the benefits and minimize the risks. What are hormones? Hormones are chemical messengers that tell the body’s cells how to function, when to grow, when to divide, and when to die. They regulate many functions, including growth, sex drive, hunger, thirst, digestion, metabolism, fat burning & storage, blood sugar, cholesterol levels, and reproduction. What are sex hormones? Sex hormones regulate the development of sex characteristics, including the sex organs such as genitals and ovaries/testicles. Sex hormones also affect the secondary sex characteristics that typically develop at puberty, like facial and body hair, bone growth, breast growth, and voice changes. There are three categories of sex hormones in the body: • Androgens: testosterone, dehydroepiandrosterone (DHEA), dihydrotestosterone (DHT) • Estrogens: estradiol, estriol, estrone • Progestin: progesterone Generally, “males” tend to have higher androgen levels, and “females” tend to have higher levels of estrogens and progestogens. What is hormone therapy? Hormone therapy is taking medicine to change the levels of sex hormones in your body. Changing these levels will affect your hair growth, voice pitch, fat distribution, muscle mass, and other features associated with sex and gender. Feminizing hormone therapy can help make the body look and feel less “masculine” and more “feminine" — making your body more closely match your identity. What medicines are involved? There are different kinds of medicines used to change the levels of sex hormones in your body. -

Puberty Suppression Treatment for Patients with Gender Dysphoria
GENder Education and Care Interdisciplinary Support (GENECIS) Puberty Suppression Treatment for Patients with Gender Dysphoria Patient Information and Informed Parental Consent and Assent for Minors Before considering to give treatment to your child to suppress puberty (put puberty "on hold” with “puberty blockers”), you need to be aware of the possible benefits and risks. After your questions or concerns are addressed and you have decided to proceed with puberty suppression for your child, you will need to initial the statements of this form as well as sign the consent form. If there is more than one parent/legal guardian, both will have to sign. Your child will also need to assent this form. What are the benefits of suppressing puberty in adolescents with gender dysphoria? The Endocrine Society recommends suppression of puberty (put puberty "on hold” with “puberty blockers”), for children that have the diagnosis of gender dysphoria as well as other specific criteria listed in the section below. This recommendation was done by experts in treating youth with gender dysphoria, based on the premise that this may: allow for a smooth social transition to the gender role that is congruent with their gender identity; test persistence of the affirmed gender after living a “real-life experience” and before receiving irreversible hormonal or surgical treatment; and diminish the psychological trauma and risk of suicide induced by the physical changes of puberty. This may also avoid the need for surgery and other expensive treatments that are required to reverse the physical effects of puberty (i.e. mastectomies, tracheal and facial shaving, and electrolysis). -

Exposure to Female Hormone Drugs During Pregnancy
British Journal of Cancer (1999) 80(7), 1092–1097 © 1999 Cancer Research Campaign Article no. bjoc.1998.0469 Exposure to female hormone drugs during pregnancy: effect on malformations and cancer E Hemminki, M Gissler and H Toukomaa National Research and Development Centre for Welfare and Health, Health Services Research Unit, PO Box 220, 00531 Helsinki, Finland Summary This study aimed to investigate whether the use of female sex hormone drugs during pregnancy is a risk factor for subsequent breast and other oestrogen-dependent cancers among mothers and their children and for genital malformations in the children. A retrospective cohort of 2052 hormone-drug exposed mothers, 2038 control mothers and their 4130 infants was collected from maternity centres in Helsinki from 1954 to 1963. Cancer cases were searched for in national registers through record linkage. Exposures were examined by the type of the drug (oestrogen, progestin only) and by timing (early in pregnancy, only late in pregnancy). There were no statistically significant differences between the groups with regard to mothers’ cancer, either in total or in specified hormone-dependent cancers. The total number of malformations recorded, as well as malformations of the genitals in male infants, were higher among exposed children. The number of cancers among the offspring was small and none of the differences between groups were statistically significant. The study supports the hypothesis that oestrogen or progestin drug therapy during pregnancy causes malformations among children who were exposed in utero but does not support the hypothesis that it causes cancer later in life in the mother; the power to study cancers in offspring, however, was very low. -

Menopausal Hormone Therapy
GYNAECOLOGY ENDOCRINOLOGY Menopausal hormone therapy: where are we now? Menopausal hormone therapy (MHT) is an effective treatment for symptoms associated with menopause, such as hot flushes, night sweats, mood changes, sleep disturbances and changes in sexual function. While the evidence around MHT has changed over the years, there is now international consensus that the benefits of MHT are likely to outweigh the risks for most women aged < 60 years or within ten years of menopause, for whom menopausal symptoms are affecting their quality of life. KEY PRACTICE POINTS: Every woman’s experience of menopause is different, and Among the oestrogen and progestogen formulations perceptions of menopause vary across cultures. Most available, transdermal oestrogen (funded) and micronised women will experience some menopause symptoms, progesterone (not funded) are associated with the lowest however, only some will seek treatment. risk of adverse effects Menopausal hormone therapy (MHT) is likely to offer overall There is no specific recommended duration for MHT. The benefit to women with menopausal symptoms affecting decision to continue treatment should be reviewed on their quality of life if they are aged < 60 years or within ten an annual basis, taking into account any changes in the years of menopause patient’s risk factors, adverse effects and extent of benefit. Adverse outcomes associated with MHT include breast If women primarily seek assistance for urogenital symptoms cancer, stroke and venous thromboembolism (VTE). of menopause, vaginal products are recommended instead However, the risk of these outcomes depends on factors of MHT. This includes moisturisers, lubricants or a vaginal such as the age or time since menopause when MHT oestrogen cream or pessary. -

Combined Estrogen–Progestogen Menopausal Therapy
COMBINED ESTROGEN–PROGESTOGEN MENOPAUSAL THERAPY Combined estrogen–progestogen menopausal therapy was considered by previous IARC Working Groups in 1998 and 2005 (IARC, 1999, 2007). Since that time, new data have become available, these have been incorporated into the Monograph, and taken into consideration in the present evaluation. 1. Exposure Data 1.1.2 Progestogens (a) Chlormadinone acetate Combined estrogen–progestogen meno- Chem. Abstr. Serv. Reg. No.: 302-22-7 pausal therapy involves the co-administration Chem. Abstr. Name: 17-(Acetyloxy)-6-chlo- of an estrogen and a progestogen to peri- or ropregna-4,6-diene-3,20-dione menopausal women. The use of estrogens with IUPAC Systematic Name: 6-Chloro-17-hy- progestogens has been recommended to prevent droxypregna-4,6-diene-3,20-dione, acetate the estrogen-associated risk of endometrial Synonyms: 17α-Acetoxy-6-chloro-4,6- cancer. Evidence from the Women’s Health pregnadiene-3,20-dione; 6-chloro-Δ6-17- Initiative (WHI) of adverse effects from the use acetoxyprogesterone; 6-chloro-Δ6-[17α] of a continuous combined estrogen–progestogen acetoxyprogesterone has affected prescribing. Patterns of exposure Structural and molecular formulae, and relative are also changing rapidly as the use of hormonal molecular mass therapy declines, the indications are restricted, O CH and the duration of the therapy is reduced (IARC, 3 C 2007). CH3 CH3 O C 1.1 Identification of the agents CH3 H O 1.1.1 Estrogens HH For Estrogens, see the Monograph on O Estrogen-only Menopausal Therapy in this Cl volume. C23H29ClO4 Relative molecular mass: 404.9 249 IARC MONOGRAPHS – 100A (b) Cyproterone acetate Structural and molecular formulae, and relative Chem. -

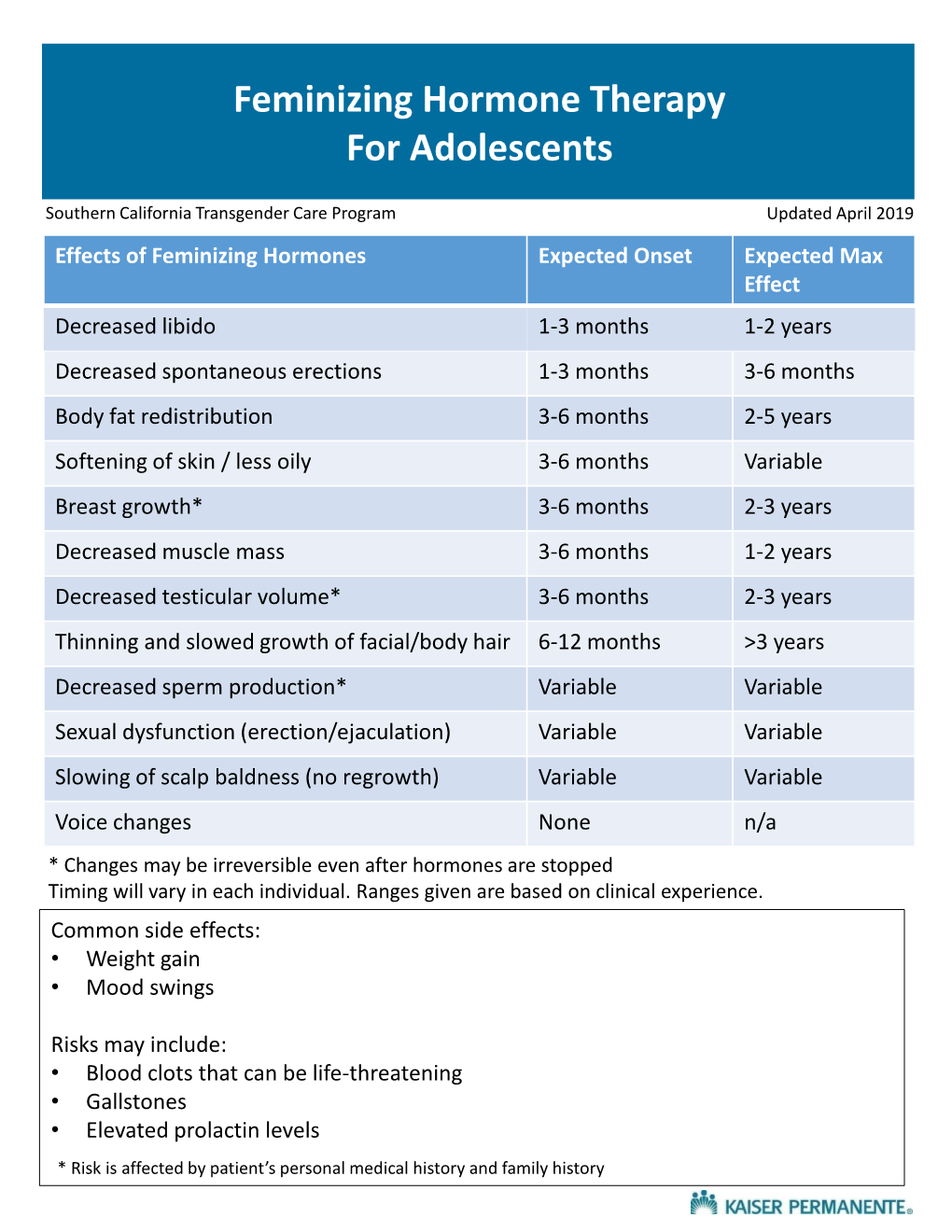
EFFECTS of FEMINIZING HORMONE THERAPY (ESTROGEN) Effects in RED Are Permanent Changes
EFFECTS OF FEMINIZING HORMONE THERAPY (ESTROGEN) Effects in RED are permanent changes. Effect First noticeable: Maximum effect: Breast enlargement 3-6 months 2-3 years Softening of skin, less 3-6 months Unknown oily skin Slower, thinner growth 6-12 months 3 years or more of facial and body hair Decrease in male Hair loss stops in 1-3 1-2 years pattern baldness months but hair does not grow back Decreased muscle mass 3-6 months 1-2 years / strength Body fat redistribution 3-6 months 2-5 years (more fat on buttocks, hips, thighs, face) Decreased libido (sex 1-3 months 1-2 years drive) Decreased spontaneous 1-3 months 3-6 months erections Decreased volume 3-6 months 2-3 years (shrinking) of the testes Decreased sperm Variable Variable production/Infertility What are the emotional and intellectual effects of estrogen? People are very different so their emotional and intellectual changes vary widely. People taking estrogen have reported: ● feeling more emotional and more in touch with their feelings ● crying more easily ● mood swings ● depression or sadness ● thinking differently, having different ways of looking at things ● feeling “more like myself” when taking a hormone that aligns with gender identity; feeling more comfortable in one’s body What estrogen does not do: ● change a person’s bone structure ● change a person’s height ● stop the growth of facial hair or eliminate a beard ● cause male pattern balding on the scalp to grow back ● raise the pitch of the voice to a higher level ● provide reliable birth control ● protect against sexually transmitted infections What are the risks of taking estrogen? The major risks are: ● blood clots ― can result in stroke or even death ● gallbladder disease ● liver disease ● weight gain ● high cholesterol which causes heart disease ● high blood pressure EFFECTS OF MASCULINIZING HORMONE THERAPY (TESTOSTERONE) Effects in RED are permanent changes. -

Farr Handouts
4/14/2021 Recent Pharmacological & Faculty Therapeutic Developments in Women’s Health Glen E. Farr, PharmD Professor Emeritus of Clinical Satellite Conference and Live Webcast Pharmacy and Translational Science April 16, 2021 University of Tennessee 9:00 – 12:00 p.m. Central Time College of Pharmacy [email protected] Produced by the Alabama Department of Public Health Video Communications and Distance Learning Division Educational Objectives Still Have • Outline the recent developments, Sugar & guidelines and/or recommendations Spice for pharmacological management of women’s health conditions, with a focus on contraception. • Identify essential information to counsel patients on the therapeutic application of these medications. Edi the Grand Dog’s first visit to our house 1 4/14/2021 2020 Drug Approvals FDA Annual Novel • 53 Novel agents approved Drug Approvals: – Historical previous 10 year average = 40 2011-2020 • 31 Orphan Drugs • 21 “First in Class” 59 53 48 45 46 • 17 Fast-track 39 41 30 • 22 Break-through 27 22 • 30 Priority review 2011 2012 2013 2014 2015 2016 2017 2018 2019 2020 • 12 Accelerated approval FDA.gov Faster FDA Drug Approvals: 3 Question Knowledge Good or Bad? Assessment on • Over the last 4 decades, the FDA has loosened its Contraception requirements for approving new drugs, increasingly accepting less data and more surrogate endpoints in clinical trials, and shortening its reviews. Is this good or bad? • From 1995 to 1997, 80.6% of new drugs were approved on the basis of two pivotal trials — but that number dropped to 52.8% from 2015 to 2017. A number of programs were enacted during the study period that led to faster approvals, such as fast track and the breakthrough therapy designation. -

Gender Dysphoria in Children and Adolescents: Medical Considerations
4/12/2016 Gender Dysphoria in Children and Adolescents: Medical Considerations Elyse Pine, MD Staff Physician Chase Brexton Health Care April 30, 2016 I have no relevant financial relationships with commercial interests I WILL be discussing off‐label uses of medications Medical Interventions 1 4/12/2016 Doing Nothing Can be Harmful! Physical Interventions for Adolescents • 1. Fully reversible interventions. – GnRH agonists “puberty blockers” – Spironolactone to decrease testosterone – Oral contraceptives or Progestin to suppress menses • 2. Partially reversible interventions. – Hormone therapy • 3. Irreversible interventions. – Surgical procedures. Typical Puberty • Female puberty ‐ onset (breast bud) age 8 to age 13 – menarche < 5 years from breast bud • Male puberty ‐ onset (testicular enlargement) > age 9, to onset by age 14 • Pace of puberty – Typically 2 years from breast bud to first period – Typically 2 years from testicular enlargement to growth spurt, voice changes, facial hair 2 4/12/2016 Female Pubertal Development Male Pubertal Development “Side Effects” of Puberty • Masculinizing changes of puberty – Deepening of voice – Adam’s apple – Facial and body hair – Skeletal changes of face • Feminizing changes of puberty – Breast growth – Change in body shape‐ hips/thighs – Menstrual cycles (reversible) 3 4/12/2016 The Dutch Protocol • GnRH agonists at age 12, cross sex hormone treatment at 16. • The first 70 Dutch candidates treated with GnRH analogs between 2000 and 2008 showed improved psychological functioning. • None opted to discontinue pubertal suppression and all eventually began cross‐sex hormone treatment. • More recently, the Amsterdam group found that adolescents with GID who underwent pubertal suppression had improved behavioral, emotional, and depressive symptoms with psychometric testing. -

PE2572 Puberty Blockers
Puberty Blockers What are puberty Puberty blockers are medicines that block puberty-related hormones that blockers? make your body go through puberty. Starting puberty blockers is a decision that is different for everyone. To make the most informed decision, this handout is meant to help you understand: • What is puberty? • What do puberty blockers do? • What are the changes that will happen to my body? • What are the benefits, risks and costs involved? We will work with you to support the decision that is best for you. You can view a video about puberty blockers at seattlechildrens.org/gender. How does puberty Puberty is the process the body goes through to become capable of begin? making a baby (reproduction), as well as reach adult size and brain development. Puberty starts when your brain tells your pituitary gland to start releasing puberty-related hormones. This happens at different ages for different people. During this time, your body starts to increase the amount of certain puberty-related hormones (Luteinizing Hormone (LH) and Follicle- Stimulating Hormone (FSH). This causes your testicles to start producing testosterone or your ovaries start producing estrogen. These hormones do not cause acne, pubic or armpit hair – those are caused by other hormones. Body changes in • Testicle growth (this improves the body’s ability to make testosterone) people with testicles • Penis growth (without puberty • Pubic hair blockers) • Increased acne, increased armpit and facial hair • Rapid growth (growth spurt) • Voice changes (deepens) Body changes in • Breast changes people with ovaries • Changes in body shape, including fuller hips (without puberty • Menstrual periods start (usually more than 2 years after breast changes blockers) begin) 1 of 6 To Learn More Free Interpreter Services • Adolescent Medicine • In the hospital, ask your nurse. -

Transgender Health: Helping Your Trans Patient to Live Their Life More
TRANSGENDER HEALTH Helping your trans patient to live their life more easily. Gender affirming services Putting you in charge of your gender journey A patient's perspective Trans life is sacrificing everything for peace of mind @VanessaS2hart Menu 2 INTRODUCTION 5 About this reference guide 5 GenderGP 6 Forward 7 Acknowledgement 8 Understanding gender identity 9 The trans umbrella 9 Gender at a glance 11 Sexuality 11 Transitioning 12 Prevalence 16 Primary healthcare team 17 Barriers to care 20 Training 20 Fear 21 Research 22 The importance of affirmation 23 Real life experience (RLE) 23 Patient groups 25 Adults 25 Older people 26 Towards the end of life 27 Children 28 Adolescents 29 Learning disabilities 32 Autistic spectrum 32 Transgender care: specialist or generalist? 34 The Royal College of General Practitioners (RCGP) 36 Creating a trans-friendly practice 37 First presentation 39 Considerations in primary care 42 General care 42 Gender dysphoria 43 Initiating treatment 44 Continuing care 45 Common scenarios 46 NHS Gender Markers 46 The process for changing gender marker 49 Gender Recognition Certificates (GRC) 49 Screening and diagnosis 50 Referral to a Gender Identity Clinic 51 Waiting times 53 3 Private Care 53 Going abroad for treatment 55 Legal requirements when treating trans patients 55 Conversion therapy 56 Coercion 57 Assessment and diagnosis 58 Criteria for treatment 60 Counselling and support 61 Medical management 62 Hormone therapy 62 Self-medication 64 Unlicensed medicines 64 Side effects 65 Informed consent 65 An important