Scar Reactivation and Dry Cough
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Skin Test Christina P
SKINTEST Skin Test Christina P. Linton 1. A middle-aged, diabetic woman presents with 6. What is the estimated 5-year survival rate for well-demarcated, yellow-brown, atrophic, telangiectatic melanoma that has spread beyond the original area plaques with a raised, violaceous border on her shins. of involvement to the nearby lymph nodes (but What is the most likely diagnosis? not to distant nodes or organs)? a. Lipodermatosclerosis a. 25% b. Pyoderma gangrenosum b. 41% c. Necrobiosis lipoidica c. 63% d. Erythema nodosum d. 87% 2. Which of the following types of fruit is most likely 7. What is another name for leprosy? to cause phytophotodermatitis? a. von Recklinghausen’s disease a. Pineapple b. MuchaYHabermann disease b. Grapefruit c. Schamberg’s disease c. Kiwi d. Hansen’s disease d. Peach 8. Which of the following is not an expected 3. Hypothyroidism can cause several changes to the skin extracutaneous finding in patients with and skin appendages including all of the following, HenochYScho¨ nlein purpura? except: a. Abdominal pain a. Hyperpigmentation b. Hematuria b. Easy bruising c. Shortness of breath c. Thin, brittle nails d. Arthralgias d. Dry, coarse skin 9. When the term ‘‘papillomatous’’ is used to describe 4. In a patient with neurofibromatosis, which sign refers a skin lesion, it means that the lesion is to the presence of bilateral axillary freckling? a. characterized by multiple fine surface projections. a. Auspitz sign b. erupting like a mushroom or fungus. b. Crowe sign c. characterized by fine fissures and cracks in the skin. c. Russell sign d. sieve like and contains many perforations. -

Skin Lesions in Diabetic Patients
Rev Saúde Pública 2005;39(4) 1 www.fsp.usp.br/rsp Skin lesions in diabetic patients N T Foss, D P Polon, M H Takada, M C Foss-Freitas and M C Foss Departamento de Clínica Médica. Faculdade de Medicina de Ribeirão Preto. Universidade de São Paulo. Ribeirão Preto, SP, Brasil Keywords Abstract Skin diseases. Dermatomycoses. Diabetes mellitus. Metabolic control. Objective It is yet unknown the relationship between diabetes and determinants or triggering factors of skin lesions in diabetic patients. The purpose of the present study was to investigate the presence of unreported skin lesions in diabetic patients and their relationship with metabolic control of diabetes. Methods A total of 403 diabetic patients, 31% type 1 and 69% type 2, underwent dermatological examination in an outpatient clinic of a university hospital. The endocrine-metabolic evaluation was carried out by an endocrinologist followed by the dermatological evaluation by a dermatologist. The metabolic control of 136 patients was evaluated using glycated hemoglobin. Results High number of dermophytosis (82.6%) followed by different types of skin lesions such as acne and actinic degeneration (66.7%), pyoderma (5%), cutaneous tumors (3%) and necrobiosis lipoidic (1%) were found. Among the most common skin lesions in diabetic patients, confirmed by histopathology, there were seen necrobiosis lipoidic (2 cases, 0.4%), diabetic dermopathy (5 cases, 1.2%) and foot ulcerations (3 cases, 0.7%). Glycated hemoglobin was 7.2% in both type 1 and 2 patients with adequate metabolic control and 11.9% and 12.7% in type 1 and 2 diabetic patients, respectively, with inadequate metabolic controls. -

The Prevalence of Cutaneous Manifestations in Young Patients with Type 1 Diabetes
Clinical Care/Education/Nutrition/Psychosocial Research ORIGINAL ARTICLE The Prevalence of Cutaneous Manifestations in Young Patients With Type 1 Diabetes 1 2 MILOSˇ D. PAVLOVIC´, MD, PHD SLAANA TODOROVIC´, MD tions, such as neuropathic foot ulcers; 2 4 TATJANA MILENKOVIC´, MD ZORANA ÐAKOVIC´, MD and 4) skin reactions to diabetes treat- 1 1 MIROSLAV DINIC´, MD RADOSˇ D. ZECEVIˇ , MD, PHD ment (1). 1 5 MILAN MISOVIˇ C´, MD RADOJE DODER, MD, PHD 3 To understand the development of DRAGANA DAKOVIC´, DS skin lesions and their relationship to dia- betes complications, a useful approach would be a long-term follow-up of type 1 OBJECTIVE — The aim of the study was to assess the prevalence of cutaneous disorders and diabetic patients and/or surveys of cuta- their relation to disease duration, metabolic control, and microvascular complications in chil- neous disorders in younger type 1 dia- dren and adolescents with type 1 diabetes. betic subjects. Available data suggest that skin dryness and scleroderma-like RESEARCH DESIGN AND METHODS — The presence and frequency of skin mani- festations were examined and compared in 212 unselected type 1 diabetic patients (aged 2–22 changes of the hand represent the most years, diabetes duration 1–15 years) and 196 healthy sex- and age-matched control subjects. common cutaneous manifestations of Logistic regression was used to analyze the relation of cutaneous disorders with diabetes dura- type 1 diabetes seen in up to 49% of the tion, glycemic control, and microvascular complications. patients (3). They are interrelated and also related to diabetes duration. Timing RESULTS — One hundred forty-two (68%) type 1 diabetic patients had at least one cutaneous of appearance of various cutaneous le- disorder vs. -

Mycosis Fungoides: a Dermatological Masquerader D
REVIEW ARTICLE DOI 10.1111/j.1365-2133.2006.07526.x Mycosis fungoides: a dermatological masquerader D. Nashan, D. Faulhaber,* S. Sta¨nder,* T.A. Luger* and R. Stadler Department of Dermatology, University of Freiburg, Hautstr. 7, 79104 Freiburg, Germany *Department of Dermatology, University of Mu¨nster, Mu¨nster, Germany Department of Dermatology, Klinikum Minden, Minden, Germany Summary Correspondence Mycosis fungoides (MF), a low-grade lymphoproliferative disorder, is the most D. Nashan. common type of cutaneous T-cell lymphoma. Typically, neoplastic T cells localize E-mail: [email protected] to the skin and produce patches, plaques, tumours or erythroderma. Diagnosis of MF can be difficult due to highly variable presentations and the sometimes non- Accepted for publication 8 June 2006 specific nature of histological findings. Molecular biology has improved the diag- nostic accuracy. Nevertheless, clinical experience is of substantial importance as Key words MF can resemble a wide variety of skin diseases. We performed a literature clinical subtypes, differential diagnoses, mycosis review and found that MF can mimic >50 different clinical entities. We present fungoides, overview a structured framework of clinical variations of classical, unusual and distinct Conflicts of interest forms of MF. Distinct subforms such as ichthyotic MF, adnexotropic (including None declared. syringotropic and folliculotropic) MF, MF with follicular mucinosis, granuloma- tous MF with granulomatous slack skin and papuloerythroderma of Ofuji are delineated in more detail. Mycosis fungoides (MF), a low-grade lymphoproliferative dis- fungoides’ with ‘differential diagnosis’ and ‘clinical picture’, order, is the most common type of cutaneous T-cell lymph- and ‘mycosis fungoides’ and ‘cutaneous T-cell lymphoma’ in oma. -

Response of Ulcerated Necrobiosis Lipoidica to Clofazimine
Letters to the Editor 651 Response of Ulcerated Necrobiosis Lipoidica to Clofazimine Frauke Benedix, Annette Geyer, Verena Lichte, Gisela Metzler, Martin Röcken and Anke Strölin* Department of Dermatology, University Hospital of Tuebingen, Liebermeisterstrasse 25, DE-72076 Tuebingen, Germany. *E-mail: anke.stroelin@med. uni-tuebingen.de Accepted May 25, 2009. Sir, The patient was referred to our department with multiple, Necrobiosis lipoidica (NL) is a chronic granulomatous pre-tibial brownish-livid, bizarrely configured, partly sclerotic maculae and plaques, pronounced central atrophy and several inflammatory disease of the skin of unknown aetiology, fibrinous ulcerations. which can be associated with diabetes mellitus. NL is Chronic venous insufficiency and peripheral arterial occlusion characterized by slowly growing initially erythematous were excluded by digital photoplethysmography, arterial and plaques that turn into yellow-brown, partly telangiectatic venous dopplersonography. Laboratory tests showed normal and atrophic scars. Ulcerations occur in approximately liver enzymes, creatinine and blood count. Borrelia serology, anti-nuclear antibody screening and HbA1c were in normal 35% of cases. ranges. Microbiological swabs detected Staphylococcus aureus Many therapies have been recommended for this without clinical signs of local inflammation. chronic disease; nevertheless, therapeutic success The biopsy showed granulomatous inflammation involving the is rare. We report here the successful treatment of entire corium and the upper subcutaneous fat tissue, with homo- ulcerated NL with clofazimine, without noteworthy genous necrobiosis lined by epithelioid histiocytes, foreign body giant cells and lymphoid cell aggregates with germinal centres, side-effects. as well as lymphoplasmacellular infiltrations around the vessels. Histology thus confirmed the diagnosis of NL (Fig. 1a). As the previous therapies were without effect, we started anti- CASE REPORT inflammatory treatment with clofazimine, 100 mg/day. -

Successful Treatment of Ulcerative and Diabeticorum
Letters 1. Picardi A, Pasquini P, Cattaruzza MS, et al. Psychosomatic factors in first- Another prevalent transverse linear crease of the face, the onset alopecia areata. Psychosomatics. 2003;44(5):374-381. nasal crease, appears across the lower third of the nasal dor- 2. Vannatta K, Gartstein MA, Zeller MH, Noll RB. Peer acceptance and social sum. In some cases, changes of pigmentation, milia, or pseudo- behavior during childhood and adolescence: how important are appearance, comedones are present along the nasal crease.5 Transverse na- athleticism, and academic competence? Int J Behav Dev. 2009;33(4): 303-311. sal milia in the absence of a transverse nasal crease are less frequently reported. Recently, our research team6 reported a OBSERVATION case of seborrheic keratosis–like hyperplasia and horn cysts aligned along this crease. These findings were attributed to the Deep Labiomental Fold With Pseudocomedones fact that the triangular cartilage and the alar cartilage attach The labiomental fold is a transverse indentation of the face, in a linear fashion at the junction of the middle and lower third which marks the intersection of the lower lip and chin.1 It plays of the nose, producing a potential embryonic fault line in which a significant role in movement of the lower lip and in facial ex- retention cysts presenting as milia and comedones can occur.5 pression. We describe herein a child with a linear pattern of Early acne lesions favor the forehead, nose, and chin in microcomedones located along a deep labiomental fold. many children. Although many times overlooked, the exter- nal ear is another common location for open and closed com- Report of a Case | A 7-year-old healthy girl presented with a line edones in young patients with acne.7 We think that the com- of black papules on her chin. -

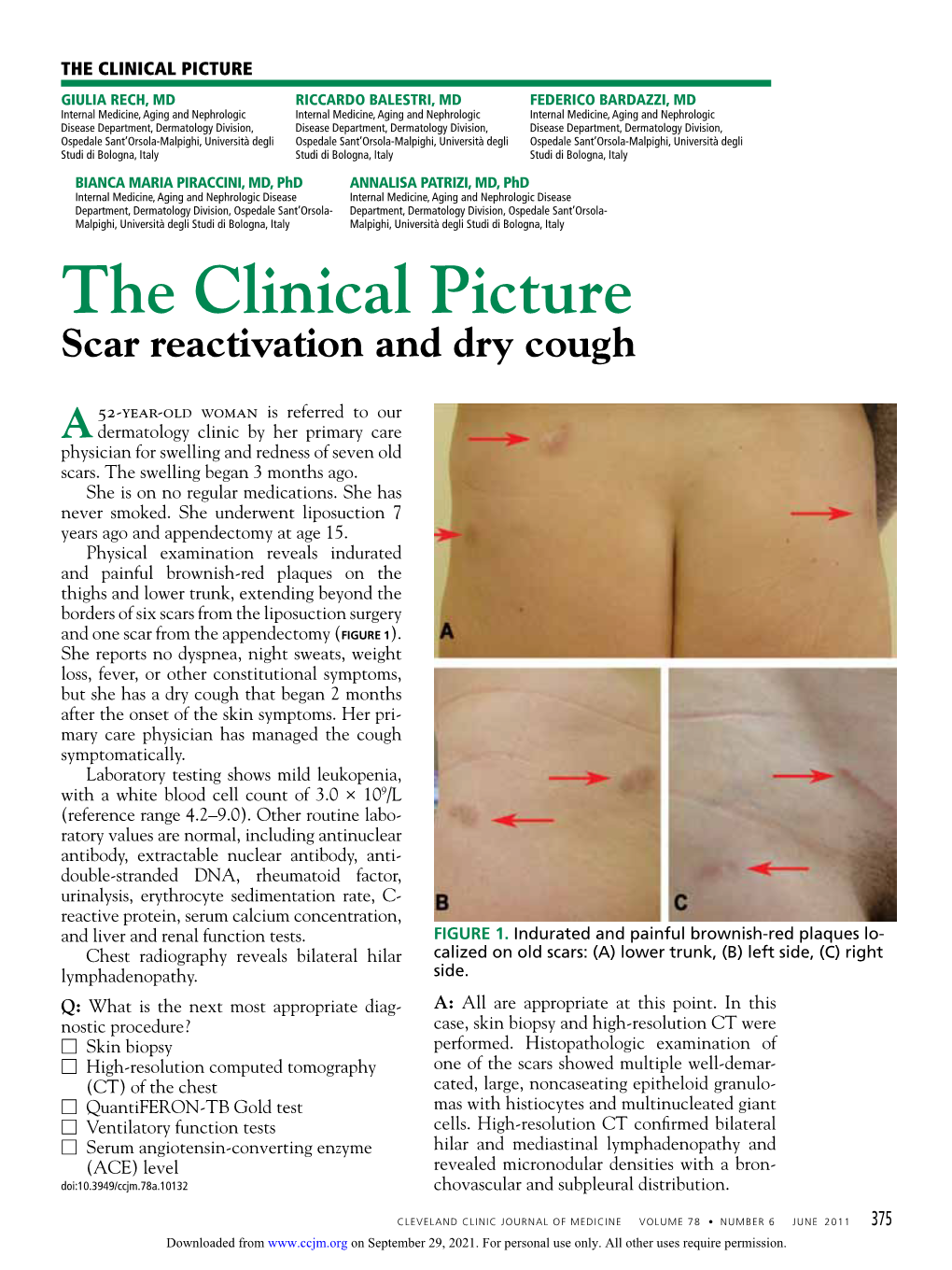
Chest Scars P.27 4
DERM CASE DERM CASE Test your knowledge wTeitsht ymouulrtikpnleo-wchleodicgee cwaisthes multiple-choice cases This month – 6 cases: 1. Chest Scars p.27 4. Torso Clusters p.30 2. Redish-Brown Plaques p.28 5. Face Protrusions p.31 3. Demarcated Facial Birthmark p.29 6. Hypopigmented Papules p.32 Case 1 Chest Scars This gentleman has developed these skin lesions on his chest. He used to excessively pick his cystic acne, which was in the same area. What is your diagnosis? a. Dermatofibroma protuberans b. Keloid scar c. Perifollicular fibroma d. Angio fibroma Answer Keloid scar (answer b) , which is excessive connec - tive tissue proliferation following an injury. Therapy: No good therapy is available for Pathogenesis: Predisposing factors for keloid for - keloids. Never make any bold promises. Simple re- mation are: excision almost never works and oftentsigonifnicantly • Ethnic factors: Keloids are far more common in worsens th©e problem. ibu blacks. Treatmtent: Possibilities tinrcludead–,corticosteroid h is nlo • Location: Sternum, shoulders, neck (after iingjection, tangenltiaDl debudlkoiwng excision, and exci - yr ia an se thyroid operation), ear lobes (piercing), apnkles, sion and ccoveragerswcith skinalgruaft can be considered o er use son shins, over clavicle, edge of chin, and other sites monly if itedis certaipnetrhat the new wound can heal C ris for m tho py where skin tension is generally increaseCd. o . Auunder lcesos skin tension with exogenous pressure r ited gle • Type of injury: Burns and infections morheiboften saipnplied and that the graft donor site can be placed e pro t a form keloids, leading to aconltractusrees and prin under prophylactic pressure. -

Necrobiosis Lipoidica with Superimposed Pyoderma Vegetans
CASE REPORT Necrobiosis Lipoidica With Superimposed Pyoderma Vegetans Carl J. Barrick, DO; Omobola Onikoyi, DO; Nektarios I. Lountzis, MD; Tanya Ermolovich, DO; Stephen M. Purcell, DO foul odor was noted in the area underlying the lesion. PRACTICE POINTS Initial punch biopsy demonstrated epidermal hyperplasia • Necrobiosis lipoidica (NL), a chronic granulomatous with neutrophil-rich sinus tracts consistent with pyoderma disease characterized by collagen degeneration, vegetans (PV)(Figure 2A). Tissue culture was positive for granulomatous formation, and endothelial-wall thick- Staphylococcus aureus and Streptococcus anginosus. Cultures ening, is most often seen in association with insulin- for both fungi and acid-fast bacilli were negative for growth. dependent diabetes mellitus (DM). The patient was treated with mupirocin ointment 2% • Asymptomatic, well-circumscribed, violaceous pap- and 3 months of cephalexin 250 mg twice daily, which ules and nodules coalesce into plaques on the lower cleared the purulent crust; however, serous drainage, extremities, face, or trunk in NL. ulceration, and erythemacopy persisted. The patient needed an • Treatment mainstay is topical and intralesional extended course of antibiotics, which had not been previ- corticosteroids at active borders of lesions. Other ously administered to clear the purulence. During this treat- treatments used with some success include tumor ment regimen, the patient’s DM remained uncontrolled. necrosis factor α inhibitors, topical tretinoin, topical tacrolimus, and skin grafting. Control and manage- notA second deeper punch biopsy revealed a layered gran- ment of DM can be helpful. ulomatous infiltrate with sclerosis throughout the dermis most consistent with necrobiosis lipoidica (NL)(Figure 2B). Direct immunofluorescence biopsy was negative. Once the Necrobiosis lipoidica (NL) is a granulomatous inflammatory skin PV was clear, betamethasone dipropionate ointment 0.05% disease strongly associated with diabetes mellitus (DM). -

Treatment of Necrobiosis Lipoidica
22 The Open Dermatology Journal, 2008, 2, 22-25 Treatment of Necrobiosis Lipoidica with 595 nm Pulsed Dye Laser – A Case Report Jean-Loïc Michel*,a and Odile Richardb aPrivate Office of Dermatology, Residence V° Avenue, 14 Place des Grenadiers-Quartier Grouchy, 42000 Saint- Etienne, France bService de Pédiatrie, Centre hospitalier universitaire, 42055 Saint-Etienne, France Abstract: Introduction: Necrobiosis Lipoidica (NL) had no adequate treatment. Some case has been treated by different vascular lasers. Third generation pulsed dye lasers with a wavelength of 595 nm has been attempted. Their selectively de- stroys shallower ectatic blood vessels. Material and Methods: We used a 595 nm, Dermobeam 2000® laser (manufactured by Deka© MELA Calenzano, Italy), with a dynamic skin cooling system (Spray). The parameters were 7 mm spot, 6 J/cm2, 0.5 Hz, and 0.5 msec. Case Report: A young Caucasian girl was diagnosed at 9 years of age (January 2002) with Necrobiosis Lipoidica over the entire pretibial region of both legs. She had been suffering from type 1 diabetes mellitus for 4 years. She received 3 insu- lin injections per day. Results: A long-standing skin breakdown of the left leg was observed which required two months’ dressing with hydrocol- loids. A cosmetic improvement was obtained after this single treatment, with a decrease in erythema and telangiectasias, and stabilization in terms of progression. However, 13 months after treatment, an extension of the peripheral telangiectasis and erythema border of the lesions was observed. Discussion: Laser therapy is proven useful to treat Necrobiosis Lipoidica only in rare cases. It is possible to treat te- langiectasias, however there is a risk of ulceration. -

Necrobiosis Lipoidica
Necrobiosis Lipoidica: A case report with dermoscopic review Sameer Shrestha1, Natalia Spierings2, and Suchana Marahatta1 1BP Koirala Institute of Health Sciences 2Affiliation not available October 16, 2020 Abstract We are presenting a case of Necrobiosis Lipodica disease in a 55 year lady whose diabetes status was not known at the time of presentation in dermatology OPD. Traditionally, the diagnosis is confirmed by histopathological examination (HPE). Dermoscopy can also be used as a noninvasive tool to confirm the diagnosis. Keywords: Dermoscopy, Necrobiosis Lipoidica, Diabetes mellitus, Granulomatous Skin Con- dition Key Clinical Message The diagnosis of NL is made traditionally by Histopathology. This case report with review helps to diagnosis NL via dermoscopy and differentiating it from other granulomatous skin condition. Introduction Necrobiosis Lipoidica (NL) is a rare idiopathic, chronic granulomatous skin condition that usually presents as asymptomatic erythematous papule on legs progressing to waxy plaques that may develop atrophy and ulceration (1). It can complicate Diabetes mellitus (DM) in about 0.3% (2). Dermoscopy may be a useful non-invasive tool to differentiate NL from other granulomatous skin conditions like lupus Vulgaris (LV), cutaneous Leishmaniasis(CL), granuloma annular(GA) and cutaneous Sarcoidosis(CS). However little is known about the characteristic findings of NL on dermoscopy. We present a case of NL that was confirmed by HPE along with its dermoscopic features and a review of the literature. Case Report A 55-year old lady presented with a 3 year history of two asymptomatic erythematous lesions , one on each shin, which had started as pinhead size papules. There was no history of any trauma, DM or thyroid disorders. -

Sabra Dermatitis: Combined Features of Delayed Hypersensitivity and Foreign Body Reaction to Implanted Glochidia
Volume 26 Number 4| April 2020| Dermatology Online Journal || Case Presentation 26(4):9 Sabra dermatitis: combined features of delayed hypersensitivity and foreign body reaction to implanted glochidia Cynthia Magro MD, Shari Lipner MD PhD Affiliations: Weill Cornell Medicine, New York, New York, USA Corresponding Author: Cynthia Magro, M. D. 1300 York Avenue, F-309, New York, NY 10065, Tel: 212-746-6434, Email: [email protected] immune response may occur whereby the histologic Abstract reaction patterns are varied and include eczematous A striking dermatitis referred to by its colloquial alterations, interface dermatitis, and features of designation of sabra dermatitis is associated with delayed dermal hypersensitivity including an glochidia inoculation from the Opuntia cactus immunogenic pattern of granulomatous commonly known as the prickly pear. We report a 45- year-old woman who had an unexpected encounter inflammation. Classic cutaneous inflammatory with a cactus plant during a trip to Texas. She reactions that encompass the spectrum of innate brushed up against the plant and was aware that she immunity and an immunologically triggered had been inoculated with several spines of the plant. response are best exemplified by reactions to Five days later she developed erythematous papules injectable filler substances such as hyaluronic acid, on the digits accompanied by swelling. The biopsy implanted silica from antecedent trauma, and red showed a very striking granulomatous reaction pattern within the dermis. There was a linear cinnabar tattoo pigment. A striking dermatitis pattern of necrobiosis, likely representing a tract of referred to by its colloquial designation of sabra inoculation injury palisaded by histiocytes including dermatitis is associated with the glochidia multinucleated forms. -

Necrobiosis Lipoidica: Ultrastructural and Biochemical Demonstration of a Collagen Defect
Necrobiosis Lipoidica: Ultrastructural and Biochemical Demonstration of a Collagen Defect Aarne Oikarinen, M .D ., Ph. D., Minna Mo rtenhul11 cr, M .D ., M atti Kallioincn, M .D., Ph.D., and Eeva-Riitta Savolainen, M. D., Ph.D. Coll agen Resea rch Unit, Unive rsity of O Ulll , Departmcnts of Dc n1l3tology (AO, MM ), Anatomy (AO), Pathology (MK), and Medi ca l Biochcmistry (AO, E-RS), Uni ve rsity of O ulu , O Ulll , Finl and T en pati ents with necrobiosis lipoidica lesions were stud lagen was unchanged in the affected skin . Fibrobl asts ied. Five pati ents had diabetes mellitus. The age of the es tablished fr o m affected skin synthesized less coll agen than patients vari ed from 15 to 73 yea rs and the durati on o f the ce ll s deri ved fr om hea lth y-looking skin. T he decreased col skin lesions w as fro m 2 to 20 yea rs. Histologica ll y, the lagen synthesis was due to a decreased amount of m essen lesions w ere characterized by degeneration of coll agen and ger RN A fo r type I procoll agen, m easured by hybridization elas tin. In som e lesions el as tin fibers could be seen in areas w ith a specific human cDN A cl one. T he producti on of devoid of normal-looking coll agen. Electron microscopy colla genase by these fib robl as ts was not in creased. O ur revea led loss of cross-striation of coHa gen fibrils and a marked res ults thus indica te that in necro bi osis lipoidica lesions, vari atio n in the diameter o f individual coll agen fibrils.