Medial Collateral Ligament, Pages 63
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Discussion Concerning Deltoid Ligament and Antero-Medial Capsule Repair in the Surgical Management of Supination External Rotati
ISSN: 2643-4016 Wei et al. Int Arch Orthop Surg 2017, 1:001 Volume 1 | Issue 1 Open Access International Archives of Orthopaedic Surgery ORIGINAL ARTICLE Discussion Concerning Deltoid Ligament and Antero-Medial Cap- sule Repair in the Surgical Management of Supination External Rotation Ankle Fractures Wei REN1,3, Masumi MARUO HOLLEDGE1, Yong Cheng HU2,3 and Jike LU1* 1Department of Orthopedic Surgery, United Family Hospital, Beijing, China Check for 2Department of Foot and Ankle Surgery, Tianjin Hospital, Tianjin, China updates 3Tianjin Medical University, Tianjin, China *Corresponding author: Jike LU, Department of Orthopedic Surgery, United Family Hospital, 2 Jiangtai Lu, Chaoyang District, Beijing, China, Tel: +4008-9191-91, E-mail: [email protected] the Lauge-Hansen classification is frequently utilized. Abstract In the classification, Supination-External Rotation (SER) Objective: To evaluate the importance of ankle deltoid liga- injuries are the most common occurrences. In a clinical ment and anteromedial capsule repair in Lauge-Hansen Su- pination-External Rotation Stage IV (SER IV) ankle fractures. setting, SER stage IV (SER IV) can be seen as a fracture of the lateral malleolus (Weber B fibular fractures) on Methods: A total of 15 patients with SER IV ankle fractures radiographs, when there is no medial malleolus frac- without medial malleolus fractures, were studied. All patients were treated with lateral malleolus Open Reduction Internal ture. However, the classification indicates that SER IV Fixation (ORIF) and transsydesmotic screws with the deltoid injuries include the syndesmotic ligament rupture and ligament, as well as anteromedial capsule repair. The Lower the deltoid ligament injuries (bimalleolar equivalent). Extremity Function Scale (LEFS), Foot and Ankle Disabili- Obviously, SER IV injuries are unstable ankle fractures. -

Ankle Ligament Injuries
ARTIGO DE REVISÃO Ankle ligament injuries Per A.F.H. Renström, M.D., Ph.D.1 and Scott A. Lynch, M.D.2 ABSTRACT ing and/or taping can alleviate instability problems in most patients. For cases of chronic instability that are refractory Acute ankle ligament sprains are common injuries. The to bracing and external support, surgical treatment can be majority of these occur during athletic participation in the explored. If the chronic instability is associated with subta- 15 to 35 year age range. Despite the frequency of the injury, lar instability that is refractory to conservative measures and diagnostic and treatment protocols have varied greatly. bracing as outlined above, surgical treatment must address Lateral ligament complex injuries are by far the most com- the subtalar joint as well. mon of the ankle sprains. Lateral ligament injuries typically Subtalar ligament injury and instability are probably more occur during plantar flexion and inversion, which is the po- common than appreciated. Definition and diagnosis of this sition of maximum stress on the anterotalofibular liagment entity are difficult, however. Fortunately, it appears that in (ATFL). For this reason, the ATFL is the most commonly the majority of the acute injuries healing occurs with the torn ligament during an inversion injury. In more severe in- same functional rehabilitation program as that for lateral ankle version injuries the calcaneofibular (CFL), posterotalofibu- ligament sprains. lar (PTFL) and subtalar ligament can also be injured. For chronic subtalar instability an intial attempt at func- Most acute lateral ankle ligament injuries recover quickly tional rehabilitation with ankle proprioceptive training and with nonoperative management. -

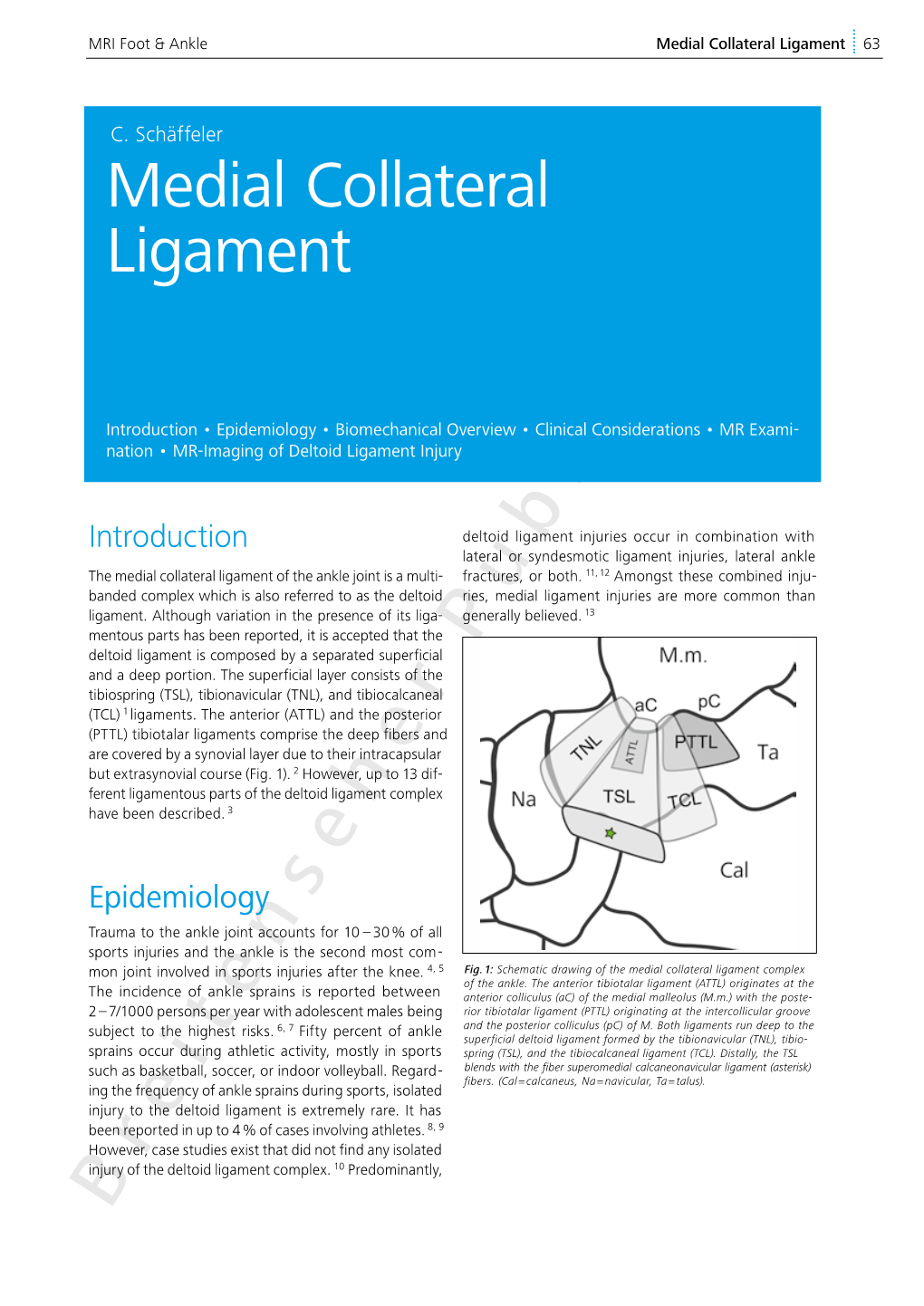
The Ligament Anatomy of the Deltoid Complex of the Ankle: a Qualitative and Quantitative Anatomical Study
e62(1) COPYRIGHT Ó 2014 BY THE JOURNAL OF BONE AND JOINT SURGERY,INCORPORATED The Ligament Anatomy of the Deltoid Complex of the Ankle: A Qualitative and Quantitative Anatomical Study Kevin J. Campbell, BS, Max P. Michalski, MSc, Katharine J. Wilson, MSc, Mary T. Goldsmith, MS, Coen A. Wijdicks, PhD, Robert F. LaPrade, PhD, MD, and Thomas O. Clanton, MD Investigation performed at the Department of Biomedical Engineering, Steadman Philippon Research Institute, and the Steadman Clinic, Vail, Colorado Background: The deltoid ligament has both superficial and deep layers and consists of up to six ligamentous bands. The prevalence of the individual bands is variable, and no consensus as to which bands are constant or variable exists. Although other studies have looked at the variance in the deltoid anatomy, none have quantified the distance to relevant osseous landmarks. Methods: The deltoid ligaments from fourteen non-paired, fresh-frozen cadaveric specimens were isolated and the ligamentous bands were identified. The lengths, footprint areas, orientations, and distances from relevant osseous landmarks were measured with a three-dimensional coordinate measurement device. Results: In all specimens, the tibionavicular, tibiospring, and deep posterior tibiotalar ligaments were identified. Three additional bands were variable in our specimen cohort: the tibiocalcaneal, superficial posterior tibiotalar, and deep anterior tibiotalar ligaments. The deep posterior tibiotalar ligament was the largest band of the deltoid ligament. The origins from the distal center of the intercollicular groove were 16.1 mm (95% confidence interval, 14.7 to 17.5 mm) for the tibionavicular ligament, 13.1 mm (95% confidence interval, 11.1 to 15.1 mm) for the tibiospring ligament, and 7.6 mm (95% confidence interval, 6.7 to 8.5 mm) for the deep posterior tibiotalar ligament. -

Medial Ankle Instability Instabilidade Medial Do Tornozelo
AR T IGO ES P ECI A L Medial ankle instability Instabilidade medial do tornozelo Beat Hintermann1, Alexej Barg2, Markus Knupp3 Abstract While much is known about the anatomy and biomechanics of lateral ankle ligaments, the medial ankle ligaments are still poorly understood. Analogously, very little objective data is available regarding the clinical presentation of medial ankle instability. The focus of this article is to elucidate the anatomy and function of the medial ligaments, and to present our experience for diagnosis and treatment of incompetent deltoid ligament. Keywords: Ankle joint/physiology; Ankle joint/surgery; Arthroscopy; Collateral ligaments/ physiology; Collateral ligaments/surgery; Joint instability/etiology; Joint instability/ physioology; Joint instability/surgery; Ligaments, articular/anatomy & histology Resumo Até quanto é conhecida a anatomia e a biomecânica do complexo ligamentar lateral, o li- gamento medial continua mal compreendido. Analogamente, poucos relatos objetivos são direcionados ao quadro clínico da instabilidade medial. O objetivo deste artigo é elucidar a anatomia e a biomecânica do ligamento medial e mostrar a experiência no diagnóstico e na conduta da incompetência do ligamento deltóide. Descritores: Articulação do tornozelo/fisiologia; Articulação do tornozelo/cirurgia; Artroscopia; Ligamentos colaterias/fisiologia; Ligamentos colaterais/cirurgia; Instabilidade articular/etiologia; Instabilidade articular/fisiologia; Instabilidade articular/cirurgia; Ligamentos articulares/anatomia & histologia Correspondência -

The Attachment Sites and Attachment Areas of Deltoid Ligament Related to Clinical Implications: a Cadaveric Study
Int. J. Morphol., 38(4):1106-1111, 2020. The Attachment Sites and Attachment Areas of Deltoid Ligament Related to Clinical Implications: A Cadaveric Study Los Sitios y las Áreas de Inserción del Ligamento Deltoideo Relacionadas con las Implicaciones Clínicas: Un Estudio Cadavérico Chanatporn Inthasan1; Yasuhito Tanaka2; Tanawat Vaseenon3 & Pasuk Mahakkanukrauh4,5 INTHASAN, C.; TANAKA, Y.; VASEENON, T. & MAHAKKANUKRAUH, P. The attachment sites and attachment areas of deltoid ligament related to clinical implications: a cadaveric study. Int. J. Morphol 38(4):1106-1111, 2020. SUMMARY: Currently, the treatment for patients with deltoid ligament injuries who require surgical treatment are anatomical repair and reconstruction. The clinicians should understand the exact knowledge of attachment areas of individual bands of deltoid ligament for a successful treatment. We studied 46 ankles of fresh frozen cadavers. The individual bands of deltoid ligament were divided to small fibers. Afterwards, each small fiber of each band was cut and marked with acrylic color on the origin and insertion followed by photo taking. Lastly, the photos of individual origin and insertion were used to calculate the attachment areas. We found six bands of deltoid ligament in all ankles except tibionavicular ligament. Moreover, we discovered deep to tibiocalcaneal and posterior to sustentaculum tali ligaments in 3 cases. Regarding the attachment area, the deep posterior tibiotalar ligament had the largest proximal and distal attachment areas which were 87.36±23.15 mm2 and 88.88±24.24 mm2, respectively. The anterior tibiotalar ligament had the least proximal and distal attachment areas which were 23.12±8.25 mm2 and 33.16±14.63 mm2, respectively. -

The Ligament Anatomy of the Deltoid Complex of the Ankle: a Qualitative and Quantitative Anatomical Study
e62(1) COPYRIGHT Ó 2014 BY THE JOURNAL OF BONE AND JOINT SURGERY,INCORPORATED The Ligament Anatomy of the Deltoid Complex of the Ankle: A Qualitative and Quantitative Anatomical Study Kevin J. Campbell, BS, Max P. Michalski, MSc, Katharine J. Wilson, MSc, Mary T. Goldsmith, MS, Coen A. Wijdicks, PhD, Robert F. LaPrade, PhD, MD, and Thomas O. Clanton, MD Investigation performed at the Department of Biomedical Engineering, Steadman Philippon Research Institute, and the Steadman Clinic, Vail, Colorado Background: The deltoid ligament has both superficial and deep layers and consists of up to six ligamentous bands. The prevalence of the individual bands is variable, and no consensus as to which bands are constant or variable exists. Although other studies have looked at the variance in the deltoid anatomy, none have quantified the distance to relevant osseous landmarks. Methods: The deltoid ligaments from fourteen non-paired, fresh-frozen cadaveric specimens were isolated and the ligamentous bands were identified. The lengths, footprint areas, orientations, and distances from relevant osseous landmarks were measured with a three-dimensional coordinate measurement device. Results: In all specimens, the tibionavicular, tibiospring, and deep posterior tibiotalar ligaments were identified. Three additional bands were variable in our specimen cohort: the tibiocalcaneal, superficial posterior tibiotalar, and deep anterior tibiotalar ligaments. The deep posterior tibiotalar ligament was the largest band of the deltoid ligament. The origins from the distal center of the intercollicular groove were 16.1 mm (95% confidence interval, 14.7 to 17.5 mm) for the tibionavicular ligament, 13.1 mm (95% confidence interval, 11.1 to 15.1 mm) for the tibiospring ligament, and 7.6 mm (95% confidence interval, 6.7 to 8.5 mm) for the deep posterior tibiotalar ligament. -

The Lower Extremity Exam for the Family Practitioner
Melinda A. Scott, D.O. THE LOWER EXTREMITY Orthopedic Associates of EXAM FOR THE FAMILY Dayton Board Certified in Primary Care PRACTITIONER Sports Medicine GOALS Identify landmarks necessary for exam of the lower extremity Review techniques for a quick but thorough exam Be familiar with normal findings and range of motion Review some special maneuvers and abnormal findings Review common diagnoses PRE-TEST QUESTIONS 20% 20% 20% 20% 20% If a patient has hip arthritis, where will he or she typically complain of pain? A. Buttock B. Low back C. Lateral hip D. Groin E. Posterior thigh 10 A. B. C. D. E. Countdown PRE-TEST QUESTIONS A positive straight leg raise test indicates 20% 20% 20% 20% 20% that the patient’s hip pain is from a A. Radicular/sciatic etiology B. Hip joint pathology C. Bursitis D. Tight Hamstrings E. Weak hip flexors 10 Countdown A. B. C. D. E. PRE-TEST QUESTIONS A positive McMurray’s tests is indicative of 20% 20% 20% 20% 20% a possible A. ACL tear B. MCL tear C. Patellar dislocation D. Joint effusion E. Meniscus tear 10 Countdown A. B. C. D. E. PRE-TEST QUESTIONS Anterior drawer test on the knee is performed with the knee in 20% 20% 20% 20% 20% A. 30 degrees flexion B. 90 degrees flexion C. Full extension D. 45 degrees flexion E. 130 degrees flexion 10 Countdown A. B. C. D. E. PRE-TEST QUESTIONS A positive squeeze test during an ankle 20% 20% 20% 20% 20% exam is indicative of A. Syndesmotic injury B. -

High Ankle Sprains: Diagnosis & Treatment
High Ankle Sprains: Diagnosis & Treatment Mark J. Mendeszoon, DPM, FACFAS, FACFAOM Precision Orthopaedic Specialties University Regional Hospitals Advanced Foot & Ankle Fellowship- Director It Is Only an Ankle Sprain Evaluate Degree of Ecchymosis & Edema If Not Properly Treated Chronic Pain & Ankle Instability Epidemiology Waterman et al. JBJS 2010 states: 2 million ankle sprains per year = 2 billion in health care cost Injury results in time lost and disability in 60% of patients 30% of all sport injury Epidemiology Syndesmotic Injuries: •1% to 18% of all ankle sprains • 32% develop calcification and chronic pain •High incidence of post traumatic arthritis Greater source of impairment than the typical lateral ankle sprain Anatomy Inferior Tibiofibular Joint: defined as a syndesmotic articulation which consists of five separate portions Motion in all three planes Anatomy “Syndesmotic Ligaments: • Anterior Inferior Tibio Fibular Ligament • Posterior Inferior Tibio Fibular Ligament • Transverse Tibio Fibular Ligament • Interosseous Ligament • Interosseous Membrane Deltoid Ligament The deep portion of the deltoid ligament also contributes to syndesmotic stability Acting as a restraint against lateral shift of the talus Biomechanics of Syndesmosis RELEVANT ASPECTS OFANKLE: A considerable clearance takes place between the talus and the distal fibula, which is limited by the tibiofibular syndesmosis With normal stance, almost no twisting and shearing forces act on the ankle joint= static tibfib tension Axial loading tensions AITF and PITF with increase of 10 -17% of body weight intact syndesmosis, the intermalleolar distance increases with dorsiflexion of the talus by 1.0 to 1.25 mm Haraguchi et al. 2009 Intact syndesmosis Fibula ROTATES 2 * externally Equals ~ 2.4 mm distally 0.2-0.4 mm Anterior -posteriorly THUS Fibula moves in 3 D Ogilvie & Harris 1994 Study on Individual Ligaments for Syndesmotic Stability 35% ATIFL 33% TRANSVERSE LIG. -

Adding Deltoid Ligament Repair in Ankle Fracture Treatment: Is It Necessary? a Systematic Review
Foot and Ankle Surgery 25 (2019) 714–720 Contents lists available at ScienceDirect Foot and Ankle Surgery journal homepage: www.elsevier.com/locate/fas Review Adding deltoid ligament repair in ankle fracture treatment: Is it necessary? A systematic review a, b c b c Sherif Dabash *, Ahmed Elabd , Eric Potter , Isaac Fernandez , Chris Gerzina , b a b Ahmed M. Thabet , William McGarvey , Amr Abdelgawad a Department of Orthopaedic Surgery, The University of Texas Health Science Center at Houston, 6431 Fannin Street, Houston, TX, 77030, United States b Department of Orthopaedic Surgery & Rehabilitation, Texas Tech University Health Sciences Center — El Paso, 4801 Alberta Avenue, El Paso, TX, 79905 United States c Department of Medical Education, Paul L. Foster School of Medicine, Texas Tech University Health Sciences Center — El Paso, Medical Education Building 2200, 5001 El Paso Drive, El Paso, TX, 79905, United States A R T I C L E I N F O A B S T R A C T Article history: Background: Deltoid ligament injuries are typically caused by supination-external rotation or pronation Received 30 May 2018 injury. Numerous ligament reconstruction techniques have been proposed; however, clear indications for Received in revised form 18 August 2018 operative repair have not yet been well established in the literature. Accepted 2 November 2018 Methods: We reviewed primary research articles comparing ORIF treatment for ankle fracture with versus without deltoid ligament repair. Keywords: Results: Five studies were identified with a total of 281 patients.137 patients underwent ORIF with deltoid repair, Ankle fracture while 144 patients underwent ORIF without deltoid ligament repair. -

Why Don't We Care About the Deltoid Ligament
Why Don’t We Care About the Deltoid Ligament Sean T. Grambart DPM FACFAS Assistant Dean of Academic Affairs, Des Moines University, College of Podiatric Medicine and Surgery Past-President, American College of Foot and Ankle Surgeons Disclosure • Bespa Global, Partner • Orthosolutions, Design Team • ACFAS Speaker Why are we discussing deltoid repairs?? Anatomy of the Deltoid Complex Superficial ligament Primary restraint to hindfoot • Originates primarily from eversion the anterior malleolus • Tibiocalcaneal (3) Primary restraint to talar external • Tibiospring (2) rotation • Tibionavicular (1) Deep ligament • Confluent with the tibiotalar joint capsule • Deep Anterior Tibiotalar (1) Knee Surg Sports Traumatol Arthrosc (2013) 21:1316–1327 • Deep Posterior Tibiotalar (2) What Camp are You In?? • No Reason to Repair the Deltoid • Deltoid repair should be performed in all patients with bimalleolar equivalent ankle fractures • Repair the deltoid only if medial-sided exposure is already required to clear soft tissue from the medial gutter • Deltoid ligament repair among high-level athletes and only after arthroscopic confirmation of complete deltoid ligament rupture. • Repair only among those who are intraoperatively unstable after ORIF What do we know biomechanically?? 21 ankles were analyzed with a motion capture system • Uninjured ankles • Ankles with SER-IV injuries • Ankles with ORIF • Ankles with ORIF and deltoid repair Journal of Orthopaedics 17 (2020) 87–90 Journal of Orthopaedics 17 (2020) 87–90 Compared to the Intact State • ORIF -

Slide 1 Manual Therapy for the Hip and Lower Quarter
Slide 1 ___________________________________ Manual Therapy for the Hip and Lower Quarter ___________________________________ Techniques and Supporting Evidence ___________________________________ Mitchell Barber Scarlett Morris ___________________________________ PT, MPT, CMT, OCS, FAAOMPT PT, DPT, CMT, OCS ___________________________________ ___________________________________ ___________________________________ Slide 2 ___________________________________ Disclosures: ___________________________________ ___________________________________ ___________________________________ ___________________________________ ___________________________________ ___________________________________ Slide 3 ___________________________________ Session 1: The Hip ___________________________________ ___________________________________ ___________________________________ ___________________________________ ___________________________________ ___________________________________ Slide 4 ___________________________________ The Hip Hip Anatomy ___________________________________ o Synovial ball-and socket joint o The head of the femur points in an ___________________________________ anterior/medial/superior direction o The acetabulum faces lateral/inferior/anterior ___________________________________ o Anteversion angle of the neck is 10-15 degrees ___________________________________ ___________________________________ ___________________________________ Slide 5 ___________________________________ The Hip Hip Anatomy ___________________________________ o Femoral -

Original Article Efficacy of Deltoid Ligament Reconstruction on the Curative Effect, Complication and Long-Term Prognosis in A
Int J Clin Exp Med 2017;10(9):13778-13783 www.ijcem.com /ISSN:1940-5901/IJCEM0060421 Original Article Efficacy of deltoid ligament reconstruction on the curative effect, complication and long-term prognosis in ankle fracture-dislocation with deltoid ligament injury Guangxue Gu, Jiwen Yu, Yongfeng Huo, Gang Xu, Zhaoyang Yin, Jian Yu, Luxin Sheng, Leiming Li Department of Traumatic Orthopedics, The First People’s Hospital of Lianyungang, Lianyungang, Jiangsu Province, China Received June 28, 2017; Accepted August 2, 2017; Epub September 15, 2017; Published September 30, 2017 Abstract: Objective: To investigate the clinical efficacy, complications and long-term prognosis of deltoid ligament reconstruction in the treatment of ankle fracture-dislocation with deltoid ligament injury. Methods: Forty enrolled patients with ankle fracture and deltoid ligament injury were diagnosed and treated in our hospital from May 2010 to June 2014. They were divided into control group and treatment group with 20 cases in each according to the random number table method. The patients in the control group were only treated with fracture open reduction and internal fixation, while the patients in the treatment group were treated with deltoid ligament reconstruction as well as fracture open reduction and internal fixation. After the surgery, all the patients were regularly followed up for 12 to 18 months. Meanwhile, the degree of pain (VAS score) and the incidences of complications were evaluated and recorded 3 months after the operation. At the final follow-up, the Ankle Hindfoot Scale of American Orthopaedic Foot and Ankle Society (AOFAS) was applied to evaluate the ankle recovery of patients.