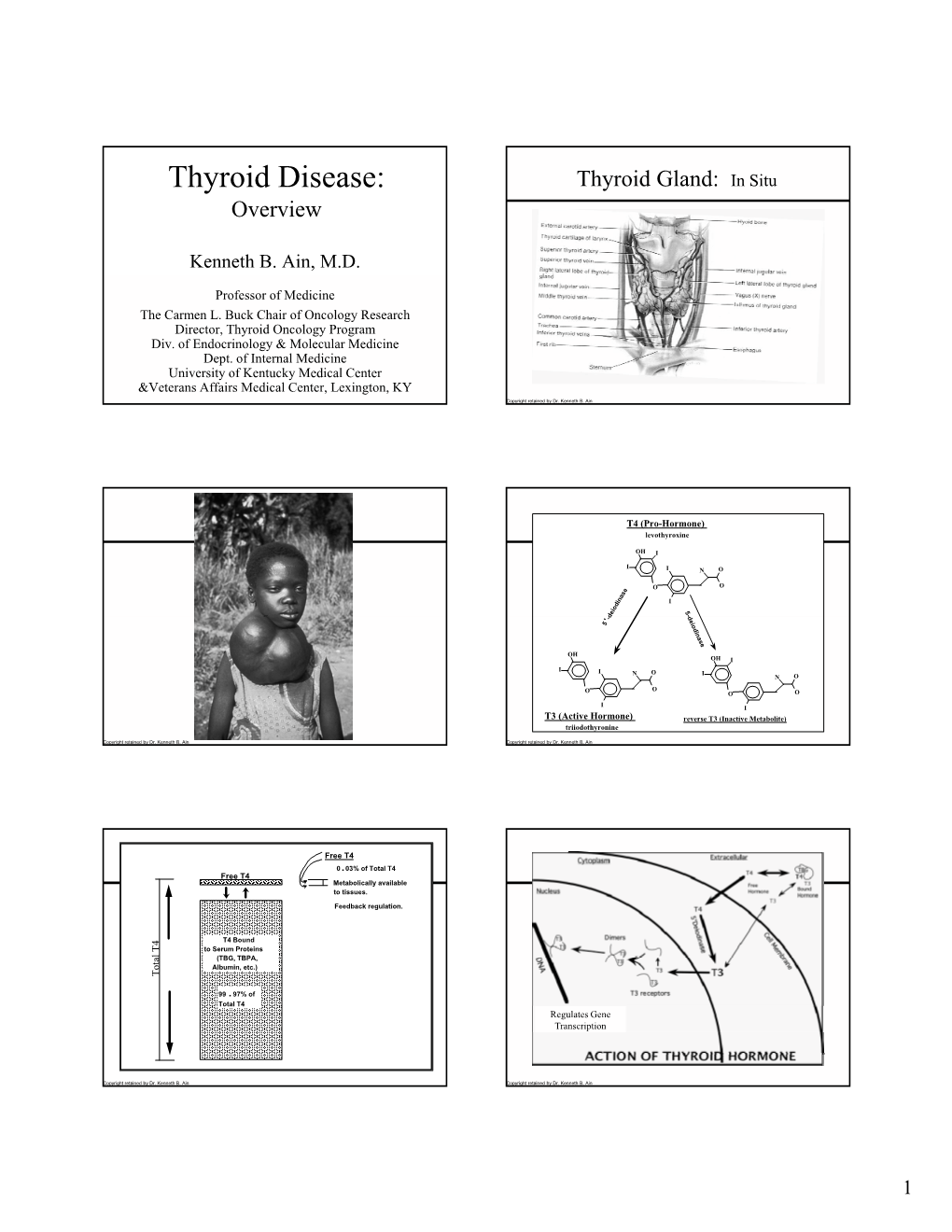
Thyroid Disease: Thyroid Gland: in Situ Overview
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Endo4 PRINT.Indb
Contents 1 Tumours of the pituitary gland 11 Spindle epithelial tumour with thymus-like differentiation 123 WHO classifi cation of tumours of the pituitary 12 Intrathyroid thymic carcinoma 125 Introduction 13 Paraganglioma and mesenchymal / stromal tumours 127 Pituitary adenoma 14 Paraganglioma 127 Somatotroph adenoma 19 Peripheral nerve sheath tumours 128 Lactotroph adenoma 24 Benign vascular tumours 129 Thyrotroph adenoma 28 Angiosarcoma 129 Corticotroph adenoma 30 Smooth muscle tumours 132 Gonadotroph adenoma 34 Solitary fi brous tumour 133 Null cell adenoma 37 Haematolymphoid tumours 135 Plurihormonal and double adenomas 39 Langerhans cell histiocytosis 135 Pituitary carcinoma 41 Rosai–Dorfman disease 136 Pituitary blastoma 45 Follicular dendritic cell sarcoma 136 Craniopharyngioma 46 Primary thyroid lymphoma 137 Neuronal and paraneuronal tumours 48 Germ cell tumours 139 Gangliocytoma and mixed gangliocytoma–adenoma 48 Secondary tumours 142 Neurocytoma 49 Paraganglioma 50 3 Tumours of the parathyroid glands 145 Neuroblastoma 51 WHO classifi cation of tumours of the parathyroid glands 146 Tumours of the posterior pituitary 52 TNM staging of tumours of the parathyroid glands 146 Mesenchymal and stromal tumours 55 Parathyroid carcinoma 147 Meningioma 55 Parathyroid adenoma 153 Schwannoma 56 Secondary, mesenchymal and other tumours 159 Chordoma 57 Haemangiopericytoma / Solitary fi brous tumour 58 4 Tumours of the adrenal cortex 161 Haematolymphoid tumours 60 WHO classifi cation of tumours of the adrenal cortex 162 Germ cell tumours 61 TNM classifi -

Thyroid Research Biomed Central
Thyroid Research BioMed Central Case report Open Access Solitary intrathyroidal metastasis of renal clear cell carcinoma in a toxic substernal multinodular goiter Gianlorenzo Dionigi*1, Silvia Uccella2, Myriam Gandolfo3, Adriana Lai3, Valentina Bertocchi1, Francesca Rovera1 and Maria Laura Tanda3 Address: 1Department of Surgical Sciences, University of Insubria, Varese, Italy, 2Human Morphology, University of Insubria, Varese, Italy and 3Clinical Medicine, University of Insubria, Varese, Italy Email: Gianlorenzo Dionigi* - [email protected]; Silvia Uccella - [email protected]; Myriam Gandolfo - [email protected]; Adriana Lai - [email protected]; Valentina Bertocchi - [email protected]; Francesca Rovera - [email protected]; Maria Laura Tanda - [email protected] * Corresponding author Published: 24 October 2008 Received: 29 May 2008 Accepted: 24 October 2008 Thyroid Research 2008, 1:6 doi:10.1186/1756-6614-1-6 This article is available from: http://www.thyroidresearchjournal.com/content/1/1/6 © 2008 Dionigi et al; licensee BioMed Central Ltd. This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. Abstract Introduction: Thyroid gland is a rare site of clinically detectable tumor metastasis. Case report: A 71-year-old woman was referred to our department for an evaluation of toxic multinodular substernal goiter. She had a history of renal clear cell carcinoma of the left kidney, which had been resected 2 years previously. US confirmed the multinodular goiter. Total thyroidectomy with neuromonitoring was performed on March 2008. -

California Tumor Tissue Registry
CALIFORNIA TUMOR TISSUE REGISTRY California Tumor Tissue Registry c/o: Department ofPathol ogy and Human Anatomy Lorna Linda University School ofMedicine 11021 Campus Avenue, AH 335 Loma Linda, Cnllfomin 92350 (909) 824-4788 FAX: (909) 478-4188 Target audience: Practicing pathologists and pathology residen.ts. Goal: To acquaint the participant with the histologic features of a variety of benign and malignant neoplasms and tumor-like conditions. Oblectlve: The participant will be able to recognize morphologic features of a variety of benign and malignant neoplasms and tumor-like conditions and relate those processes to pertinent references in the medical literature. Educational methods and media: Review of representative glass slides with associated histories. Feedback on consensus diagnoses from participating pathologists. Listing of selected references from the medical literature. Principal faculty: Weldon K. Bullock, MD Donald R. Chase, MD CME Credit: The CTTR designates this activity for up to 2 hours of continuing medical education. Participants must return their diagnoses to the CTTR as documentation of participation in this activity. Accreditation: The California Tumor Tissue Registry is accredited by the California Medical Association as a provider of continuing medical education. CONTRIBUTOR: Shelley L. Tepper, M.D. CASE NO. 1 • JANUARY 1997 San Francisco, CA TISSUE FROM: Thyroid ACCESSION #25451 CLINICAL ABSTRACf: This 34"year-old gay Caucasian male with generalized lymphadenopathy presented with a left neck mass. A few weeks later, a right neck mass developed. A total thyroidectomy was performed. GROSS PATHOLOGY: The right lobe of this 48 gram total thyroidectomy specimen vias markedly larger than the left and measured 7.0 x 3.0 x 4.0 em in greatest dimension. -

Evaluation of Head and Neck Masses in Adults
Evaluation of Head and Neck Masses in Adults Kristi Chang, MD Associate Professor Department of Otolaryngology-Head and Neck Surgery University of Iowa Hospitals and Clinics Annual Refresher Course for the Family Physician April 2018 1 Objectives Recognize when practitioners should worry about head and neck adenopathy Identify what are common serious causes of cervical lymphadenopathy and neck masses Understand how location of a neck mass guides differential diagnosis Identify indications warranting a biopsy of a neck mass and referral to an otolaryngologist 2 Neck mass –Background Definition: abnormal lesion that is visible, palpable, or seen on imaging study – can be acquired or congenital Location: – below mandible, above clavicle, deep to skin Etiologies can be varied – Adult neck masses are more likely to be malignant neoplasms – Persistent neck masses should be considered malignant until proven otherwise 3 Neck Mass - History What is the Age of patient? • Adults > 40 yrs old ~ 80% of neck masses are neoplastic (except thyroid) • Peds neck masses ~ 80% infectious/inflammatory • 16-40 yrs ~ 30% neoplastic, 50% infectious/inflammatory What is the DURATION of the mass? What is the LOCATION of mass? Duration and location are key factors in developing differential diagnosis Any new, persistent lateral neck mass in an adult > 40 yrs old is likely to be malignant Many upper aerodigestive tract cancers present with the chief concern of a painless neck mass 4 Neck Mass - Duration impacts Etiology • Traumatic: hematoma, vascular injury • Infectious/Inflammatory: • adenopathy from viral or bacterial infection . ACUTE : onset over days • odontogenic . more likely to be symptomatic • salivary gland • Neoplastic process more likely: • metastatic from upper aerodigestive • tract mucosa . -

Genetics of Familial Non-Medullary Thyroid Carcinoma (FNMTC)
cancers Review Genetics of Familial Non-Medullary Thyroid Carcinoma (FNMTC) Chiara Diquigiovanni * and Elena Bonora Unit of Medical Genetics, Department of Medical and Surgical Sciences, University of Bologna, 40138 Bologna, Italy; [email protected] * Correspondence: [email protected]; Tel.: +39-051-208-8418 Simple Summary: Non-medullary thyroid carcinoma (NMTC) originates from thyroid follicular epithelial cells and is considered familial when occurs in two or more first-degree relatives of the patient, in the absence of predisposing environmental factors. Familial NMTC (FNMTC) cases show a high genetic heterogeneity, thus impairing the identification of pivotal molecular changes. In the past years, linkage-based approaches identified several susceptibility loci and variants associated with NMTC risk, however only few genes have been identified. The advent of next-generation sequencing technologies has improved the discovery of new predisposing genes. In this review we report the most significant genes where variants predispose to FNMTC, with the perspective that the integration of these new molecular findings in the clinical data of patients might allow an early detection and tailored therapy of the disease, optimizing patient management. Abstract: Non-medullary thyroid carcinoma (NMTC) is the most frequent endocrine tumor and originates from the follicular epithelial cells of the thyroid. Familial NMTC (FNMTC) has been defined in pedigrees where two or more first-degree relatives of the patient present the disease in absence of other predisposing environmental factors. Compared to sporadic cases, FNMTCs are often multifocal, recurring more frequently and showing an early age at onset with a worse outcome. FNMTC cases Citation: Diquigiovanni, C.; Bonora, E. -

Thyroid and Parathyroid Glands
HISTOLOGY Endocrine Block – 432 Histology Team Lectures 2 and 3: Thyroid and Parathyroid Glands Done by: Lama Al Tawil Bayan Al Mugheerah Reviewed by: Ammar Alyamani Color Guide: Black: Slides. Red: Important. Green: Doctor’s notes (Female). Blue: Doctor’s notes (Male). Orange: Explanation. Objectives 1. Describe the histological structure of thyroid gland. 2. Identify and correlate between the different endocrine cells in thyroid gland and their functions. 3. Describe the microscopic structure of the parathyroid gland. 4. Describe the functional structure of the parathyroid cells. Mind Map THYROID GLAND STROMA PARENCHYMA Reticlular Follicular Parafollicular Capsule Septa cells cells (C cells) fibers Parathyroid Gland Stroma Parenchyma Reticlular Capsule Septa Chief Cells Oxyphil Cells C.T Thyroid Gland THYROID GLAND STROMA PARENCHYMA OF THYROID GLAND 1- Capsule: THYROID FOLLICLES: Dense irregular collagenous C.T. Are the structural and functional units of the 2- Septa (Interlobular septa): thyroid gland. (Variable in size and spherical in shape). Dense irregular collagenous C.T because L/M: it’s part of the capsule divides the thyroid 1- Simple cuboidal epithelium: into lobules. a- Follicular cells. 3- Reticular fibers: b- Parafollicular cells. (Adjacent to a). Thin C.T., composed mostly of reticular 2- Colloid: central colloid-filled lumen. (Acidophilic without any cells and rich in iodine and fibers with rich capillary plexus thyroglobulin, and so it has the stored hormone & (fenestrated blood capillary) surrounds it’s also the place of iodination). each thyroid follicle. N.B. Each follicle is surrounded by thin basal lamina. Each follicle is single layered. a) FOLLICULAR (PRINCIPAL) CELLS L/M: E/M: - Simple cuboidal cells. -
A Comprehensive Review on MEN2B
25 2 Endocrine-Related F Castinetti et al. Multiple endocrine neoplasia 25:2 T29–T39 Cancer type 2B THEMATIC REVIEW A comprehensive review on MEN2B Frederic Castinetti1, Jeffrey Moley2, Lois Mulligan3 and Steven G Waguespack4 1Department of Endocrinology, Aix Marseille University, CNRS UM 7286, Assistance Publique Hopitaux de Marseille, Marseille, France 2Department of Surgery, Washington University School of Medicine, St Louis, Missouri, USA 3Division of Cancer Biology and Genetics, Cancer Research Institute, Queen’s University, Kingston, Ontario, Canada 4Department of Endocrine Neoplasia and Hormonal Disorders, The University of Texas MD Anderson Cancer Center, Houston, Texas, USA Correspondence should be addressed to F Castinetti: [email protected] This paper is part of a thematic review section on 25 Years of RET and MEN2. The guest editors for this section were Lois Mulligan and Frank Weber. Abstract MEN2B is a very rare autosomal dominant hereditary tumor syndrome associated with Key Words medullary thyroid carcinoma (MTC) in 100% cases, pheochromocytoma in 50% cases and f medullary thyroid cancer multiple extra-endocrine features, many of which can be quite disabling. Only few data f pheochromocytoma are available in the literature. The aim of this review is to try to give further insights into f ganglioneuromas the natural history of the disease and to point out the missing evidence that would help f RET clinicians optimize the management of such patients. MEN2B is mainly characterized by f marfanoid the early occurrence of MTC, which led the American Thyroid Association to recommend preventive thyroidectomy before the age of 1 year. However, as the majority of mutations are de novo, improved knowledge of the nonendocrine signs would help to lower the age of diagnosis and improve long-term outcomes. -

ENDOCRINE SYSTEM the Nervous and Endocrine Systems Act Together to Coordinate Functions of All Body Systems
ENDOCRINE SYSTEM The nervous and endocrine systems act together to coordinate functions of all body systems. Recall that the nervous system acts through nerve impulses (action potentials) conducted along axons of neurons. At synapses, nerve impulses trigger the release\ of mediator (messenger) molecules called neurotransmitters The endocrine system also controls body activities by releasing mediators, called hormones, but the means of control of the two systems are very different A hormone (hormon _ to excite or get moving) is a mediator molecule that is released in one part of the body but regulates the activity of cells in other parts of the body. Most hormones enter interstitial fluid and then the bloodstream. The circulating blood delivers hormones to cells throughout the body. Both neurotransmitters and hormones exert their effects by binding to receptors on or in their ―target‖ cells. Several mediators act as both neurotransmitters and hormones. One familiar example is norepinephrine, which is released as a neurotransmitter by sympathetic postganglionic neurons and as a hormone by chromaffin cells of the adrenal medullae. The body contains two kinds of glands: exocrine glands and endocrine glands. Exocrine glands (exo- _ outside) secrete their products into ducts that carry the secretions into body cavities, into the lumen of an organ, or to the outer surface of the body. Exocrine glands include sudoriferous (sweat), sebaceous (oil), mucous, and digestive glands. Endocrine glands (endo- _ within) secrete their products (hormones) into the interstitial fluid surrounding the secretory cells rather than into ducts. From the interstitial fluid, hormones diffuse into blood capillaries and blood carries them to target cells throughout the body. -

(MEN2) the Risk
What you should know about Multiple Endocrine Neoplasia Type 2 (MEN2) MEN2 is a condition caused by mutations in the RET gene. Approximately 25% (1 in 4) individuals with medullary thyroid cancer have a mutation in the RET gene. Individuals with RET mutations may also develop tumors in their parathyroid and adrenal glands (pheochromocytoma). There are three types of MEN2, based on the family history and specific mutation found in the RET gene: • MEN2A is the most common type of MEN2, with medullary thyroid cancer developing in young adulthood. MEN2A is also associated with adrenal and parathyroid tumors. • MEN2B is the most aggressive form of MEN2, with medullary thyroid cancer developing in early childhood. MEN2B is associated with adrenal tumors, but parathyroid tumors are rare. Individuals with MEN2B can also develop benign nodules on their lips and tongue, abnormalities of the gastrointestinal tract, and are usually tall in comparison to their family members. • Familial Medullary Thyroid Cancer (FMTC) is characterized by medullary thyroid cancer (usually in young adulthood) without adrenal or parathyroid tumors. The risk for cancer associated with MEN2 • MEN2A is associated with a ~100% risk for medullary thyroid cancer; 50% risk of adrenal tumors; and 25% risk of parathyroid tumors • MEN2B is associated with a 100% risk for medullary thyroid cancer; 50% risk of adrenal tumors; and rare risk of parathyroid tumors • FMTC is associated with ~ 100% risk for medullary thyroid cancer; and no risk for adrenal or parathyroid tumors Tumors that develop in the adrenal glands in individuals with MEN2 are typically not cancerous, but can produce excessive amounts of hormones called catecholamines, which can cause very high blood pressure. -

Dopamicue Somatostatin Corticosteroids
https://theses.gla.ac.uk/ Theses Digitisation: https://www.gla.ac.uk/myglasgow/research/enlighten/theses/digitisation/ This is a digitised version of the original print thesis. Copyright and moral rights for this work are retained by the author A copy can be downloaded for personal non-commercial research or study, without prior permission or charge This work cannot be reproduced or quoted extensively from without first obtaining permission in writing from the author The content must not be changed in any way or sold commercially in any format or medium without the formal permission of the author When referring to this work, full bibliographic details including the author, title, awarding institution and date of the thesis must be given Enlighten: Theses https://theses.gla.ac.uk/ [email protected] Role of Bioaetive Peptides In Autoimmune Thyroid Disease Thesis Submitted To The Faculty of Medicine University of Glasgow For The Degree of Doctor of Philosophy By Gholam Reza Moshtaghi Kashanian Department of Pathological Biochemistry Gartnavel General Hospital Glasgow June 1996 ProQuest Number: 10391489 All rights reserved INFORMATION TO ALL USERS The quality of this reproduction is dependent upon the quality of the copy submitted. In the unlikely event that the author did not send a com plete manuscript and there are missing pages, these will be noted. Also, if material had to be removed, a note will indicate the deletion. uest ProQuest 10391489 Published by ProQuest LLO (2017). Copyright of the Dissertation is held by the Author. All rights reserved. This work is protected against unauthorized copying under Title 17, United States C ode Microform Edition © ProQuest LLO. -

Thyroid Hormone Synthesis Continues Despite Biallelic Thyroglobulin Mutation with Cell Death
Thyroid hormone synthesis continues despite biallelic thyroglobulin mutation with cell death Xiaohan Zhang, … , Viviana A. Balbi, Peter Arvan JCI Insight. 2021. https://doi.org/10.1172/jci.insight.148496. Research In-Press Preview Endocrinology Graphical abstract Find the latest version: https://jci.me/148496/pdf Thyroid hormone synthesis continues despite biallelic thyroglobulin mutation with cell death Authors: Xiaohan Zhang1, Aaron P. Kellogg1, Cintia E. Citterio1,2,3, Hao Zhang1, Dennis Larkin1, Yoshiaki Morishita1,4, Héctor M. Targovnik2,3, Viviana Balbi5, and Peter Arvan1* Affiliations: 1Division of Metabolism, Endocrinology & Diabetes, University of Michigan, Ann Arbor, MI 48105 2Universidad de Buenos Aires. Facultad de Farmacia y Bioquímica. Departamento de Microbiología, Inmunología, Biotecnología y Genética/Cátedra de Genética. Buenos Aires, Argentina. 3CONICET, Universidad de Buenos Aires, Instituto de Inmunología, Genética y Metabolismo (INIGEM), Buenos Aires, Argentina 4Division of Diabetes, Department of Internal Medicine, Aichi Medical University, 1-1 Yazakokarimata, Nagakute, Aichi 480-1195, Japan 5Department of Endocrinology and Growth, Hospital de Niños Sor María Ludovica, La Plata, Argentina Conflict of interest: The authors declare that no conflict of interest exists. Short Title: Thyroxine synthesis from dead cells 1 Complete absence of thyroid hormone is incompatible with life in vertebrates. Thyroxine is synthesized within thyroid follicles upon iodination of thyroglobulin conveyed from the endoplasmic reticulum (ER), via the Golgi complex, to the extracellular follicular lumen. In congenital hypothyroidism from bi-allelic thyroglobulin mutation, thyroglobulin is misfolded and cannot advance from the ER, eliminating its secretion and triggering ER stress. Nevertheless, untreated patients somehow continue to synthesize sufficient thyroxine to yield measurable serum levels that sustain life. -
Case Report: Primary Thyroid Lymphoma Presenting As a Rapidly Enlarging Thyroid Mass
Endocrinology & Metabolism International Journal Case Report Open Access Case report: primary thyroid lymphoma presenting as a rapidly enlarging thyroid mass Abstract Volume 1 Issue 1 - 2014 Primary thyroid lymphoma is a rarely encountered clinical entity that occurs mainly in G Papadakis,1 A Tertipi,1 M Papazian,2 K elderly females. We present a case of B-cell origin thyroid lymphoma. The diagnosis was 1 1 made by combined histology and immunochemistry. A 79-year-old woman presented with Moustakas, A Pappas 1Department of Endocrinology and Diabetes Center, Metaxa an enlarging neck mass with compression signs, dysphagia and pressure sensation around Anticancer Hospital, Greece the neck. On admission, the sonogram of the thyroid gland showed an enlarged mass and 2Department of Pathology, Metaxa Anticancer Hospital, Greece CT scan demonstrated diffuse enlargement of the thyroid extending on the anterior chest wall. After total thyroidectomy, the histological investigation revealed the presence of a Correspondence: Georgios Papadakis, Department of diffuse large B-cell non-Hodgkin’s lymphoma without other loci from the systemic staging. Endocrinology and Diabetes Center, Metaxa Anticancer The patient underwent chemotherapy and radiation therapy. Clinicians should include Hospital, Mpotasi 51, Pireaus 18537, Athens, Greece, Tel primary thyroid lymphoma in the differential diagnosis of a rapidly enlarging thyroid mass. 00306932598392, Email Keywords: primary thyroid lymphoma, non-hodgkin lymphoma, thyroid cancer Received: October 21, 2014 | Published: November 15, 2014 Abbreviations: PTL, primary thyroid lymphomas; MALT, On admission three months later, the symptoms deteriorated. mucosa associated lymphoid tissue Clinical examination revealed a firm, immobile and painless mass descending in the anterior chest wall.