FEP 5 Tier Rx Drug Formulary (607) Standard Option
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

SPIRONOLACTONE Spironolactone – Oral (Common Brand Name
SPIRONOLACTONE Spironolactone – oral (common brand name: Aldactone) Uses: Spironolactone is used to treat high blood pressure. Lowering high blood pressure helps prevent strokes, heart attacks, and kidney problems. It is also used to treat swelling (edema) caused by certain conditions (e.g., congestive heart failure) by removing excess fluid and improving symptoms such as breathing problems. This medication is also used to treat low potassium levels and conditions in which the body is making too much of a natural chemical (aldosterone). Spironolactone is known as a “water pill” (potassium-sparing diuretic). Other uses: This medication has also been used to treat acne in women, female pattern hair loss, and excessive hair growth (hirsutism), especially in women with polycystic ovary disease. Side effects: Drowsiness, lightheadedness, stomach upset, diarrhea, nausea, vomiting, or headache may occur. To minimize lightheadedness, get up slowly when rising from a seated or lying position. If any of these effects persist or worsen, notify your doctor promptly. Tell your doctor immediately if any of these unlikely but serious side effects occur; dizziness, increased thirst, change in the amount of urine, mental/mood chances, unusual fatigue/weakness, muscle spasms, menstrual period changes, sexual function problems. This medication may lead to high levels of potassium, especially in patients with kidney problems. If not treated, very high potassium levels can be fatal. Tell your doctor immediately if you notice any of the following unlikely but serious side effects: slow/irregular heartbeat, muscle weakness. Precautions: Before taking spironolactone, tell your doctor or pharmacist if you are allergic to it; or if you have any other allergies. -

Endothelin System and Therapeutic Application of Endothelin Receptor
xperim ACCESS Freely available online & E en OPEN l ta a l ic P in h l a C r m f o a c l a o n l o r g u y o J Journal of ISSN: 2161-1459 Clinical & Experimental Pharmacology Research Article Endothelin System and Therapeutic Application of Endothelin Receptor Antagonists Abebe Basazn Mekuria, Zemene Demelash Kifle*, Mohammedbrhan Abdelwuhab Department of Pharmacology, School of Pharmacy, College of Medicine and Health Sciences, University of Gondar, Gondar, Ethiopia ABSTRACT Endothelin is a 21 amino acid molecule endogenous potent vasoconstrictor peptide. Endothelin is synthesized in vascular endothelial and smooth muscle cells, as well as in neural, renal, pulmonic, and inflammatory cells. It acts through a seven transmembrane endothelin receptor A (ETA) and endothelin receptor B (ETB) receptors belongs to G protein-coupled rhodopsin-type receptor superfamily. This peptide involved in pathogenesis of cardiovascular disorder like (heart failure, arterial hypertension, myocardial infraction and atherosclerosis), renal failure, pulmonary arterial hypertension and it also involved in pathogenesis of cancer. Potentially endothelin receptor antagonist helps the treatment of the above disorder. Currently, there are a lot of trails both per-clinical and clinical on endothelin antagonist for various cardiovascular, pulmonary and cancer disorder. Some are approved by FAD for the treatment. These agents are including both selective and non-selective endothelin receptor antagonist (ETA/B). Currently, Bosentan, Ambrisentan, and Macitentan approved -

PI3K Inhibitors in Cancer: Clinical Implications and Adverse Effects
International Journal of Molecular Sciences Review PI3K Inhibitors in Cancer: Clinical Implications and Adverse Effects Rosalin Mishra , Hima Patel, Samar Alanazi , Mary Kate Kilroy and Joan T. Garrett * Department of Pharmaceutical Sciences, College of Pharmacy, University of Cincinnati, Cincinnati, OH 45267-0514, USA; [email protected] (R.M.); [email protected] (H.P.); [email protected] (S.A.); [email protected] (M.K.K.) * Correspondence: [email protected]; Tel.: +1-513-558-0741; Fax: +1-513-558-4372 Abstract: The phospatidylinositol-3 kinase (PI3K) pathway is a crucial intracellular signaling pathway which is mutated or amplified in a wide variety of cancers including breast, gastric, ovarian, colorectal, prostate, glioblastoma and endometrial cancers. PI3K signaling plays an important role in cancer cell survival, angiogenesis and metastasis, making it a promising therapeutic target. There are several ongoing and completed clinical trials involving PI3K inhibitors (pan, isoform-specific and dual PI3K/mTOR) with the goal to find efficient PI3K inhibitors that could overcome resistance to current therapies. This review focuses on the current landscape of various PI3K inhibitors either as monotherapy or in combination therapies and the treatment outcomes involved in various phases of clinical trials in different cancer types. There is a discussion of the drug-related toxicities, challenges associated with these PI3K inhibitors and the adverse events leading to treatment failure. In addition, novel PI3K drugs that have potential to be translated in the clinic are highlighted. Keywords: cancer; PIK3CA; resistance; PI3K inhibitors Citation: Mishra, R.; Patel, H.; Alanazi, S.; Kilroy, M.K.; Garrett, J.T. -

Minutes of the CHMP Meeting 14-17 September 2020
13 January 2021 EMA/CHMP/625456/2020 Corr.1 Human Medicines Division Committee for medicinal products for human use (CHMP) Minutes for the meeting on 14-17 September 2020 Chair: Harald Enzmann – Vice-Chair: Bruno Sepodes Disclaimers Some of the information contained in these minutes is considered commercially confidential or sensitive and therefore not disclosed. With regard to intended therapeutic indications or procedure scopes listed against products, it must be noted that these may not reflect the full wording proposed by applicants and may also vary during the course of the review. Additional details on some of these procedures will be published in the CHMP meeting highlights once the procedures are finalised and start of referrals will also be available. Of note, these minutes are a working document primarily designed for CHMP members and the work the Committee undertakes. Note on access to documents Some documents mentioned in the minutes cannot be released at present following a request for access to documents within the framework of Regulation (EC) No 1049/2001 as they are subject to on- going procedures for which a final decision has not yet been adopted. They will become public when adopted or considered public according to the principles stated in the Agency policy on access to documents (EMA/127362/2006). 1 Addition of the list of participants Official address Domenico Scarlattilaan 6 ● 1083 HS Amsterdam ● The Netherlands Address for visits and deliveries Refer to www.ema.europa.eu/how-to-find-us Send us a question Go to www.ema.europa.eu/contact Telephone +31 (0)88 781 6000 An agency of the European Union © European Medicines Agency, 2020. -

Expert Review 2
2021 Expert Committee on Selection and Use of Essential Medicines Application review I.1 Albendazole, mebendazole and praziquantel for the indication of treatment of (item number) taeniid cestode cysts Does the application adequately ☒ Yes address the issue of the public health ☐ need for the medicine? No ☐ Not applicable Comments: The larval stages of three taeniid cestode parasites, Echinococcus granulosus, Echinococcus multilocularis and Taenia solium, produce cysts in humans that are of medical relevance. The diseases caused by these parasitic cysts are called cystic echinococcosis (CE), alveolar echinococcosis (AE), and cysticercosis (being neurocysticercosis (NCC) the most common form) respectively, and they are recognised by WHO as neglected tropical diseases. NCC is mainly a disease of poverty that predominantly affects rural populations in Africa, Asia and Latin America. Access to diagnostic and treatment, to better manage epilepsy and other NCC is a challenge for the people affected in these communities due to the availability and costs of specialised diagnostic and care. Stigma and social discrimination also mean that many people try to “hide” the disease. Briefly summarize the role of the The only real options for treatment of CE are albendazole (ALB) and Mebendazole proposed medicine(s) relative to other (MEB). ALB is the drug of choice as it has better bioavailability. ALB is also preferred to therapeutic agents currently included in MEB, because MEB requires a higher dose and a higher pill burden, for example, an the Model List, or available in the adult patient would require 8 tablets/day of MEB compared with 2 tablets/day ALB. market. ALB and praziquantel ( PZQ) are the only drugs used for the antiparasitic treatment of NCC. -

Acetadote (Acetylcysteine) Injection Is Available As a 20% Solution in 30 Ml (200Mg/Ml) Single Dose Glass Vials
NDA 21-539/S-004 Page 3 Acetadote® (acetylcysteine) Injection Package Insert NDA 21-539/S-004 Page 4 RX ONLY PRESCRIBING INFORMATION ACETADOTE® (acetylcysteine) Injection For Intravenous Use DESCRIPTION Acetylcysteine injection is an intravenous (I.V.) medication for the treatment of acetaminophen overdose. Acetylcysteine is the nonproprietary name for the N-acetyl derivative of the naturally occurring amino acid, L-cysteine (N-acetyl-L-cysteine, NAC). The compound is a white crystalline powder, which melts in the range of 104° to 110°C and has a very slight odor. The molecular formula of the compound is C5H9NO3S, and its molecular weight is 163.2. Acetylcysteine has the following structural formula: H CH3 N SH O COOH Acetadote is supplied as a sterile solution in vials containing 20% w/v (200 mg/mL) acetylcysteine. The pH of the solution ranges from 6.0 to 7.5. Acetadote contains the following inactive ingredients: 0.5 mg/mL disodium edetate, sodium hydroxide (used for pH adjustment), and Sterile Water for Injection, USP. CLINICAL PHARMACOLOGY Acetaminophen Overdose: Acetaminophen is absorbed from the upper gastrointestinal tract with peak plasma levels occurring between 30 and 60 minutes after therapeutic doses and usually within 4 hours following an overdose. It is extensively metabolized in the liver to form principally the sulfate and glucoronide conjugates which are excreted in the urine. A small fraction of an ingested dose is metabolized in the liver by isozyme CYP2E1 of the cytochrome P-450 mixed function oxidase enzyme system to form a reactive, potentially toxic, intermediate metabolite. The toxic metabolite preferentially conjugates with hepatic glutathione to form nontoxic cysteine and mercapturic acid derivatives, which are then excreted by the kidney. -
ALBENDAZOLE (Extrapolation to All Ruminants)
European Medicines Agency Veterinary Medicines and Inspections EMEA/MRL/865/03-FINAL June 2004 COMMITTEE FOR MEDICINAL PRODUCTS FOR VETERINARY USE ALBENDAZOLE (Extrapolation to all ruminants) SUMMARY REPORT (3) 1. Albendazole is a benzimidazole carbamate, used for the treatment of gastrointestinal infestations with roundworms, lungworms and tapeworms and adult flukes of Fasciola hepatica. Albendazole is currently entered into Annex I of Council Regulation (EEC) No. 2377/90 in accordance with the following table: Pharmacologically Marker residue Animal MRLs Target Other active substance(s) species tissues provisions Albendazole Sum of albendazole Bovine, 100 µg/kg Muscle sulphoxide, ovine 100 µg/kg Fat albendazole sulphone 1000 µg/kg Liver and albendazole 2- 500 µg/kg Kidney amino sulphone 100 µg/kg Milk expressed as albendazole 2. In reviewing the availability of endo- and ectoparasiticides for sheep and goats, albendazole was considered for extrapolation from bovine and ovine species to all ruminants. The considerations and criteria leading to the identification of albendazole are described in the Position Paper Regarding Availability of Veterinary Medicines – Extrapolation of MRLs (EMEA/CVMP/457/03-FINAL). 3. The scientific justification for this extrapolation was assessed in accordance with the Notes for Guidance on Risk Analysis Approach for Residues of Veterinary Medicinal Products in Food of Animal Origin (EMEA/CVMP/187/00-FINAL) and on the Establishment of Maximum Residue Limits for Minor Animal Species (EMEA/CVMP/153a/97-FINAL). 4. In setting the ADI in the original assessment of albendazole, the data summarised on the paragraphs below were considered. 5. The mode of action of albendazole is by binding strongly with the tubulin in the cells of nematodes. -

The Promise of N-Acetylcysteine in Neuropsychiatry
Review The promise of N-acetylcysteine in neuropsychiatry 1,2,3,4 5,6 1 1,2,4 Michael Berk , Gin S. Malhi , Laura J. Gray , and Olivia M. Dean 1 School of Medicine, Deakin University, Geelong, Victoria, Australia 2 Department of Psychiatry, University of Melbourne, Parkville, Victoria, Australia 3 Orygen Research Centre, Parkville, Victoria, Australia 4 The Florey Institute of Neuroscience and Mental Health, Victoria, Australia 5 Discipline of Psychiatry, Sydney Medical School, University of Sydney, Sydney, Australia 6 CADE Clinic, Department of Psychiatry, Level 5 Building 36, Royal North Shore Hospital, St Leonards, 2065, Australia N-Acetylcysteine (NAC) targets a diverse array of factors with the pathophysiology of a diverse range of neuropsy- germane to the pathophysiology of multiple neuropsy- chiatric disorders, including autism, addiction, depression, chiatric disorders including glutamatergic transmission, schizophrenia, bipolar disorder, and Alzheimer’s and Par- the antioxidant glutathione, neurotrophins, apoptosis, kinson’s diseases [3]. Determining precisely how NAC mitochondrial function, and inflammatory pathways. works is crucial both to understanding the core biology This review summarises the areas where the mecha- of these illnesses, and to opening the door to other adjunc- nisms of action of NAC overlap with known pathophysi- tive therapies operating on these pathways. The current ological elements, and offers a pre´ cis of current literature article will initially review the possible mechanisms of regarding the use of NAC in disorders including cocaine, action of NAC, and then critically appraise the evidence cannabis, and smoking addictions, Alzheimer’s and Par- that suggests it has efficacy in the treatment of neuropsy- kinson’s diseases, autism, compulsive and grooming chiatric disorders. -

AHFS Pharmacologic-Therapeutic Classification System
AHFS Pharmacologic-Therapeutic Classification System Abacavir 48:24 - Mucolytic Agents - 382638 8:18.08.20 - HIV Nucleoside and Nucleotide Reverse Acitretin 84:92 - Skin and Mucous Membrane Agents, Abaloparatide 68:24.08 - Parathyroid Agents - 317036 Aclidinium Abatacept 12:08.08 - Antimuscarinics/Antispasmodics - 313022 92:36 - Disease-modifying Antirheumatic Drugs - Acrivastine 92:20 - Immunomodulatory Agents - 306003 4:08 - Second Generation Antihistamines - 394040 Abciximab 48:04.08 - Second Generation Antihistamines - 394040 20:12.18 - Platelet-aggregation Inhibitors - 395014 Acyclovir Abemaciclib 8:18.32 - Nucleosides and Nucleotides - 381045 10:00 - Antineoplastic Agents - 317058 84:04.06 - Antivirals - 381036 Abiraterone Adalimumab; -adaz 10:00 - Antineoplastic Agents - 311027 92:36 - Disease-modifying Antirheumatic Drugs - AbobotulinumtoxinA 56:92 - GI Drugs, Miscellaneous - 302046 92:20 - Immunomodulatory Agents - 302046 92:92 - Other Miscellaneous Therapeutic Agents - 12:20.92 - Skeletal Muscle Relaxants, Miscellaneous - Adapalene 84:92 - Skin and Mucous Membrane Agents, Acalabrutinib 10:00 - Antineoplastic Agents - 317059 Adefovir Acamprosate 8:18.32 - Nucleosides and Nucleotides - 302036 28:92 - Central Nervous System Agents, Adenosine 24:04.04.24 - Class IV Antiarrhythmics - 304010 Acarbose Adenovirus Vaccine Live Oral 68:20.02 - alpha-Glucosidase Inhibitors - 396015 80:12 - Vaccines - 315016 Acebutolol Ado-Trastuzumab 24:24 - beta-Adrenergic Blocking Agents - 387003 10:00 - Antineoplastic Agents - 313041 12:16.08.08 - Selective -

Reference List of Drugs with Potential Anticholinergic Effects 1, 2, 3, 4, 5
ANTICHOLINERGICS: Reference List of Drugs with Potential Anticholinergic Effects 1, 2, 3, 4, 5 J Bareham BSP © www.RxFiles.ca Aug 2021 WHENEVER POSSIBLE, AVOID DRUGS WITH MODERATE TO HIGH ANTICHOLINERGIC ACTIVITY IN OLDER ADULTS (>65 YEARS OF AGE) Low Anticholinergic Activity; Moderate/High Anticholinergic Activity -B in combo Beers Antibiotics Antiparkinsonian Cardiovascular Agents Immunosuppressants ampicillin *ALL AVAILABLE AS amantadine SYMMETREL atenolol TENORMIN azaTHIOprine IMURAN cefOXitin GENERIC benztropine mesylate COGENTIN captopril CAPOTEN cyclosporine NEORAL clindamycin bromocriptine PARLODEL chlorthalidone GENERIC ONLY hydrocortisone CORTEF gentamicin (Oint & Sol’n NIHB covered) carbidopa/levodopa SINEMET digoxin LANOXIN, TOLOXIN methylprednisolone MEDROL piperacillin entacapone COMTAN dilTIAZem CARDIZEM, TIAZAC prednisone WINPRED dipyridamole PERSANTINE, ethopropazine PARSITAN vancomycin phenelzine NARDIL AGGRENOX disopyramide RYTHMODAN Muscle Relaxants pramipexole MIRAPEX Antidepressants baclofen LIORESAL ( on intrathecal only) procyclidine KEMADRIN furosemide LASIX amitriptyline ELAVIL cyclobenzaprine FLEXERIL selegiline ELDEPRYL hydrALAZINE APRESOLINE clomiPRAMINE ANAFRANIL isosorbide ISORDIL methocarbamol ROBAXIN OTC trihexyphenidyl ARTANE desipramine NORPRAMIN metoprolol LOPRESOR orphenadrine NORFLEX OTC doxepin >6mg SINEQUAN Antipsychotics NIFEdipine ADALAT tiZANidine ZANAFLEX A imipramine TOFRANIL quiNIDine GENERIC ONLY C ARIPiprazole ABILIFY & MAINTENA -

Phase I Trial of the PARP Inhibitor Olaparib and AKT Inhibitor Capivasertib in Patients with BRCA1/2- and Non–BRCA1/2-Mutant Cancers
Published OnlineFirst June 12, 2020; DOI: 10.1158/2159-8290.CD-20-0163 RESEARCH ARTICLE Phase I Trial of the PARP Inhibitor Olaparib and AKT Inhibitor Capivasertib in Patients with BRCA1/2- and Non–BRCA1/2-Mutant Cancers Timothy A. Yap1,2, Rebecca Kristeleit3, Vasiliki Michalarea1, Stephen J. Pettitt4,5, Joline S.J. Lim1, Suzanne Carreira2, Desamparados Roda1,2, Rowan Miller3, Ruth Riisnaes2, Susana Miranda2, Ines Figueiredo2, Daniel Nava Rodrigues2, Sarah Ward1,2, Ruth Matthews1,2, Mona Parmar1,2, Alison Turner1,2, Nina Tunariu1, Neha Chopra1,4, Heidrun Gevensleben2, Nicholas C. Turner1,4, Ruth Ruddle2, Florence I. Raynaud2, Shaun Decordova2, Karen E. Swales2, Laura Finneran2, Emma Hall2, Paul Rugman6, Justin P.O. Lindemann6, Andrew Foxley6, Christopher J. Lord4,5, Udai Banerji1,2, Ruth Plummer7, Bristi Basu8, Juanita S. Lopez1,2, Yvette Drew7, and Johann S. de Bono1,2 Downloaded from cancerdiscovery.aacrjournals.org on September 30, 2021. © 2020 American Association for Cancer Research. Published OnlineFirst June 12, 2020; DOI: 10.1158/2159-8290.CD-20-0163 ABSTRACT Preclinical studies have demonstrated synergy between PARP and PI3K/AKT path- way inhibitors in BRCA1 and BRCA2 (BRCA1/2)–deficient andBRCA1/2 -proficient tumors. We conducted an investigator-initiated phase I trial utilizing a prospective intrapatient dose- escalation design to assess two schedules of capivasertib (AKT inhibitor) with olaparib (PARP inhibi- tor) in 64 patients with advanced solid tumors. Dose expansions enrolled germline BRCA1/2-mutant tumors, or BRCA1/2 wild-type cancers harboring somatic DNA damage response (DDR) or PI3K–AKT pathway alterations. The combination was well tolerated. Recommended phase II doses for the two schedules were: olaparib 300 mg twice a day with either capivasertib 400 mg twice a day 4 days on, 3 days off, or capivasertib 640 mg twice a day 2 days on, 5 days off. -
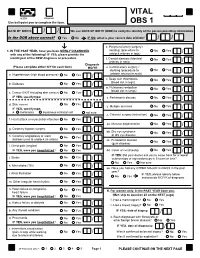
VITAL Jan 2019 Follow-Up
VITAL 6308 Request Use ball-point pen to complete the form. OBS 1 DATE OF BIRTH: / / We use DATE OF BIRTH (DOB) to verify the identity of the person providing information. Is the DOB above correct? Yes No IF NO, what is your correct date of birth? / / s. Peripheral artery surgery / 1. IN THE PAST YEAR, have you been NEWLY DIAGNOSED stenting (procedure to No Yes / with any of the following? IF YES, please provide the unblock arteries in legs) month/year of the NEW diagnosis or procedure. t. Carotid stenosis (blocked No Yes Answer NO/YES on each line. arteries in neck) / Diagnosis (Please complete either N/Y for each item) MO/YR u. Carotid artery surgery / stenting (procedure to No Yes / a. Hypertension (high blood pressure) No Yes / unblock arteries in neck) v. Deep vein thrombosis No Yes (blood clot in legs) / b. Diabetes No Yes / w. Pulmonary embolism No Yes (blood clot in lungs) / c. Cancer (NOT including skin cancer) No Yes / IF YES, specify type: _______________________ x. Parkinson's disease No Yes / d. Skin cancer No Yes / y. Multiple sclerosis No Yes IF YES, specify type: / e. melanoma squamous or basal cell not sure z. Cataract surgery (extraction) No Yes / f. Heart attack or myocardial infarction No Yes / aa. Macular degeneration No Yes / g. Coronary bypass surgery No Yes / bb. Dry eye syndrome No Yes or dry eye disease / h. Coronary angioplasty or stent No Yes (balloon used to unblock an artery) / cc. Periodontal disease No Yes (gum disease) / i. Chest pain (angina) No Yes / IF YES, were you hospitalized? No Yes dd.