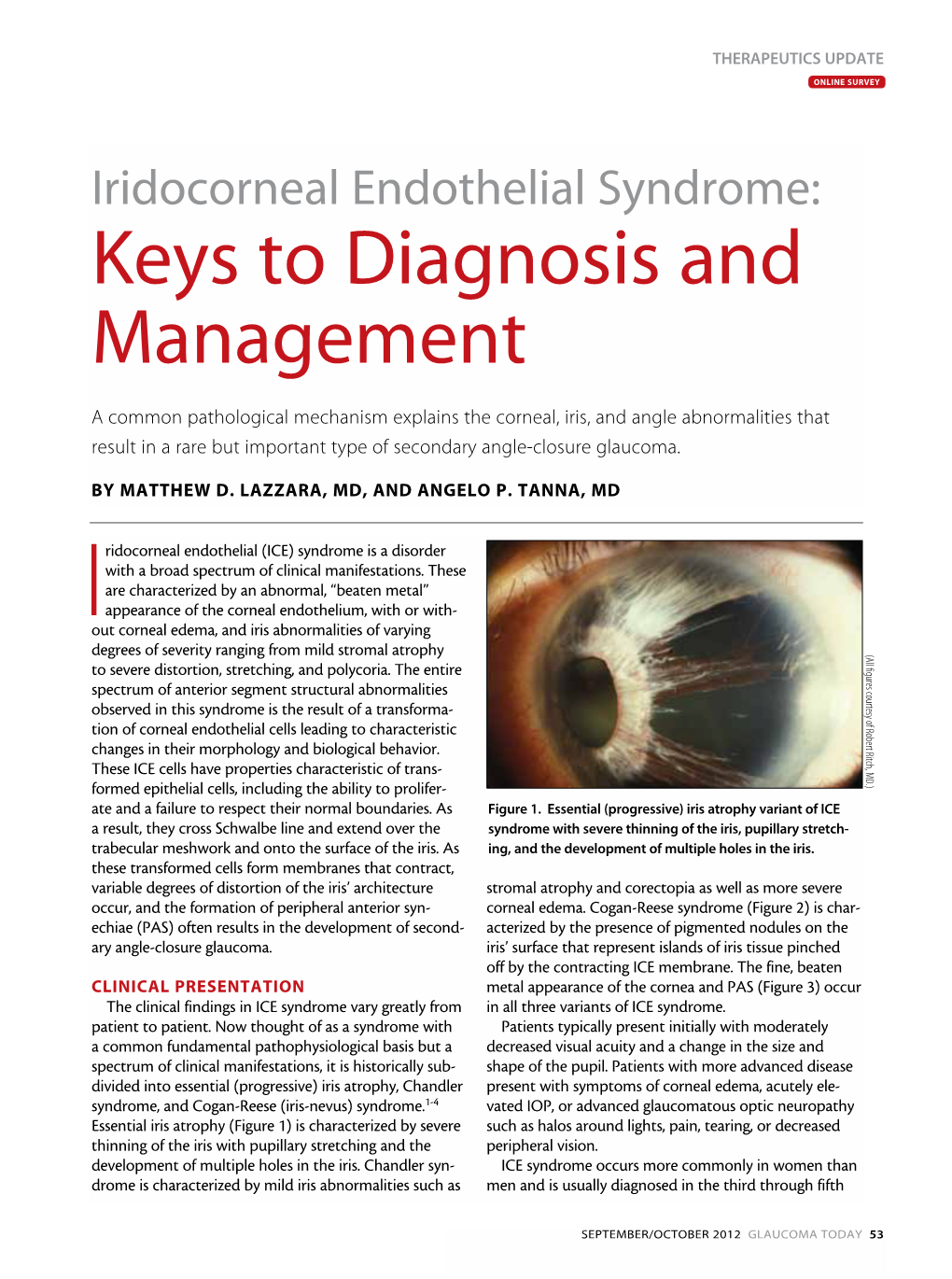
Iridocorneal Endothelial Syndrome: Keys to Diagnosis and Management
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

PITX2 and FOXC1 Spectrum of Mutations in Ocular Syndromes
European Journal of Human Genetics (2012) 20, 1224–1233 & 2012 Macmillan Publishers Limited All rights reserved 1018-4813/12 www.nature.com/ejhg ARTICLE PITX2 and FOXC1 spectrum of mutations in ocular syndromes Linda M Reis1, Rebecca C Tyler1, Bethany A Volkmann Kloss1,2,KalaFSchilter1,2, Alex V Levin3,RBrianLowry4, Petra JG Zwijnenburg5,ElizaStroh3,UlrichBroeckel1, Jeffrey C Murray6 and Elena V Semina*,1,2 Anterior segment dysgenesis (ASD) encompasses a broad spectrum of developmental conditions affecting anterior ocular structures and associated with an increased risk for glaucoma. Various systemic anomalies are often observed in ASD conditions such as Axenfeld-Rieger syndrome (ARS) and De Hauwere syndrome. We report DNA sequencing and copy number analysis of PITX2 and FOXC1 in 76 patients with syndromic or isolated ASD and related conditions. PITX2 mutations and deletions were found in 24 patients with dental and/or umbilical anomalies seen in all. Seven PITX2-mutant alleles were novel including c.708_730del, the most C-terminal mutation reported to date. A second case of deletion of the distant upstream but not coding region of PITX2 was identified, highlighting the importance of this recently discovered mechanism for ARS. FOXC1 deletions were observed in four cases, three of which demonstrated hearing and/or heart defects, including a patient with De Hauwere syndrome; no nucleotide mutations in FOXC1 were identified. Review of the literature identified several other patients with 6p25 deletions and features of De Hauwere syndrome. The 1.3-Mb deletion of 6p25 presented here defines the critical region for this phenotype and includes the FOXC1, FOXF2, and FOXQ1 genes. -

Microphthalmos Associated with Cataract, Persistent Fetal Vasculature, Coloboma and Retinal Detachment
Case Report Case report: Microphthalmos associated with cataract, persistent fetal vasculature, coloboma and retinal detachment VP Singh1, Shrinkhal2,* 1Professor, 2Junior Resident, Department of Ophthalmology, Institute of Medical Sciences, Banaras Hindu University, Varanasi, Uttar Pradesh *Corresponding Author: Email: [email protected] Abstract We present here a case of left eye microphthalmos associated with cataract, persistent fetal vasculature (previously known as persistent hyperplastic primary vitreous), iris and retinochoroidal coloboma and retinal detachment. No surgical intervention was done and the patient was kept on regular follow-up. Keywords: Microphthalmos, Cataract, Persistent fetal vasculature, Coloboma, Retinal detachment. Case Summary reacting in left eye. Mature cataract (Fig. 2) was present A 12 years old girl was referred to our department with fundus details not visible. with chief complaint of sudden diminution of vision in left eye for last 20 days. She was apparently well 20 days back, and then incidentally she closed her right eye and noticed diminution of vision in her left eye. Antenatal history was uneventful. There was no history of trauma during delivery or during perinatal period. Parents took her to a local practioner where she was diagnosed with unilateral left eye congenital cataract and referred to our centre. Her visual acuity at presentation was 6/6 in right eye on Snellen’s chart; left eye visual acuity was only 6/60 on Snellen’s visual acuity chart. Intraocular pressure was 18 mm of Hg in right eye and 14 mm of Hg in left eye by Applanation tonometry. There was no history of trauma, fever, headache, any drug intake before she Fig. -

Eye Abnormalities Present at Birth
Customer Name, Street Address, City, State, Zip code Phone number, Alt. phone number, Fax number, e-mail address, web site Eye Abnormalities Present at Birth Basics OVERVIEW • Single or multiple abnormalities that affect the eyeball (known as the “globe”) or the tissues surrounding the eye (known as “adnexa,” such as eyelids, third eyelid, and tear glands) observed in young dogs and cats at birth or within the first 6–8 weeks of life • Congenital refers to “present at birth”; congenital abnormalities may be genetic or may be caused by a problem during development of the puppy or kitten prior to birth or during birth • The “cornea” is the clear outer layer of the front of the eye; the pupil is the circular or elliptical opening in the center of the iris of the eye; light passes through the pupil to reach the back part of the eye (known as the “retina”); the iris is the colored or pigmented part of the eye—it can be brown, blue, green, or a mixture of colors; the “lens” is the normally clear structure directly behind the iris that focuses light as it moves toward the back part of the eye (retina); the “retina” contains the light-sensitive rods and cones and other cells that convert images into signals and send messages to the brain, to allow for vision GENETICS • Known, suspected, or unknown mode of inheritance for several congenital (present at birth) eye abnormalities • Remaining strands of iris tissue (the colored or pigmented part of the eye) that may extend from one part of the iris to another or from the iris to the lining of the -

Ocular Associations of Myelinated Retinal Nerve Ibers: a Study Based
ISSN 2374-216X Ocular associations of myelinated retinal nerve ibers: A study based on a case report Sonay Beyatli, BS; Yasemin Polat, BS; Ali Riza Cenk Celebi, MD, FEBO* *Ali Riza Cenk Celebi, MD, FEBO Acibadem University School of Medicine Department of Ophthalmology Turgut Ozal Boulevard, No: 16, Kucukcekmece, Istanbul 34303, Turkey Abstract Purpose: The purpose of this case report is to present a patient with unilateral isolated myelinated retinal nerve ibers (MRNFs) with its differential diagnosis. Case presentation: A 34 year-old man admitted for a routine annual checkup examination. His slit lamp biomicroscopic examination of both eyes and dilated fundus examination of the right eye were all within normal limits. Dilated fundus examination of the left eye revealed the presence of white-grey patch like lesion on the upper temporal quadrant of the retina unrelated to the optic nerve head. The appearance of the lesion was consistent with the MRNF. Visual ield exam revealed absolute scotomas corresponding to the MRNF site. Systemic examination of the patient was unremarkable. Conclusion: In cases of MRNFs it is essential to perform clinical investigations to determine the precise location of and potential etiological factors and ocular associations for MRNFs. Keywords MRNFs; biomicroscopy; absolute scotomas Introduction Myelin accelerates the transmission of the electrical signals along the myelin nerve ibers [1]. The myelination of the retinal ganglion cell axons starts from the geniculate body in the intrauterine life and it ends at the level of lamina cribrosa in the postnatal period. This suggests that lamina cribrosa is a barrier to myelination [2-4]. Myelinated retinal nerve ibers (MRNFs) originate as a result of abnormal migration of oligodendrocyte-like glial cells into the retina prior to the development of the barrier function of the lamina cribrosa [5]. -

“A Prospective Study of Visual Outcome of Open Globe Ocular Injuries at Kims Hubli”
“A PROSPECTIVE STUDY OF VISUAL OUTCOME OF OPEN GLOBE OCULAR INJURIES AT KIMS HUBLI” BY DR. RAVI SHANKAR M Dissertation submitted to the RAJIV GANDHI UNIVERSITY OF HEALTH SCIENCES, KARNATAKA, BENGALURU. In partial fulfillment of the requirements for the degree of MASTER OF SURGERY In OPHTHALMOLOGY Under the guidance of Dr. UDAY SRIDHAR MULGUND M.S. ASSOCIATE PROFESSOR DEPARTMENT OF OPHTHALMOLOGY KARNATAKA INSTITUTE OF MEDICAL SCIENCES HUBBALLI, 580021 2018 I RAJIV GANDHI UNIVERSITY OF HEALTH SCTENCES, KARNATAKA DECLAITATIOI\ BY THE CAi\DIDATE i herebr cieclare that tliis clissertation'thesis cntitied "A lrltOSPEC'l.tVE S'l'tlD\' ol" \'lStrAI- otr'l'(,oME ol.' OPL.N GLoIltr- oCULAR IN.IURIIIS A-t' KINIS llllBl.I" is a bonaflde ancl getruine research u,orli carried out br,me Lrncler the gttidiince o1' Dr. tIDAY SIIIDIIAR MtJLG[JNID. rr.s. Associate Profbssor. tr)cpartttrcttt o1'Ophthahrolosr'. Karnataka hrstitute of N{edical Scierrccs. Hubballi. ("; JLa-*-ka--r'' Date:.25f rolr+ - Dr. I{AVI SIIANI(AIi M Place: HLrbballi. [)ost graclLratc stuc]ent- I)epartnrent of Ophthahlologr'. Iian-ratalia InstitLrte of Medical Sciences Htrbballi. KARNATAKA INSTITUTE OF MEDICAL SCIENCES, HUBBALLI. CERTIFICATE BY THE GUIDE This is to certify that the dissertation entitled "A PROSPECTM STUDY OF VISUAL OUTCOME OF OPEN GLOBE OCULAR INJURIES AT KIMS HUBLT" is a bonafide research work done by Dr. RAVI SHANKAR M in partial fulfi11ment of the requirement for degree of MASTER oF SURGERY in OPIITHALMOLOGY. Date:.d.S-/LoltV Dr. UDAY SRIDHAR VIULGUND, nr.s. Place: Hubballi. Associate Professor, Department of Ophthahnology, I(an-rataka Institute of Medical Sciences, Hubballi. -

Glaucoma : Science and Practice
www.dbeBooks.com - An Ebook Library MRSNFM-i-xiv 8/30/02 9:40 AM Page i Glaucoma Science and Practice MRSNFM-i-xiv 8/30/02 9:40 AM Page ii This page intentionally left blank MRSNFM-i-xiv 8/30/02 9:40 AM Page iii Glaucoma Science and Practice Edited by John C. Morrison, M.D. Irvin P. Pollack, M.D. Professor of Ophthalmology Professor of Ophthalmology Oregon Health and Science University The Johns Hopkins University And And Director of the Glaucoma Service Emeritus The Fred P. Thompson Glaucoma Clinic Ophthalmologist-In-Chief and and Casey Eye Institute Director Krieger Eye Institute Portland, Oregon Sinai Hospital of Baltimore Baltimore Maryland Thieme New York • Stuttgart MRSNFM-i-xiv 8/30/02 9:40 AM Page iv Consulting Editor: Esther Gumpert Editorial Assistant: Owen Zurhellen Director, Production and Manufacturing: Anne Vinnicombe Production Editor: Becky Dille Marketing Director: Phyllis Gold Sales Manager: Ross Lumpkin Chief Financial Officer: Peter van Woerden President: Brian D. Scanlan Compositor: Emilcomp\Prepare Ltd. Printer: Four Colour Imports, Ltd. Library of Congress Cataloging-in-Publication Data Glaucoma : a clinical guide / [edited by] John C. Morrison, Irvin P. Pollack p. ; cm. Includes bibliograpical references. ISBN 0-86577-915-5 (TMP : alk. paper) -- ISBN 3131246715 (GTV : alk. paper) 1. Glaucoma. I. Morrison, John C., 1951 - II. Pollack, Irvin P. [DNLM: 1. Glaucoma. WW 290 G54935 2003] RE871 .G5437 2003 617.7'41--dc21 2002075001 Copyright © 2003 by Thieme Medical Publishers, Inc. This book, including all parts thereof, is legally protected by copyright. Any use, exploitation or commercialization outside the narrow limits set by copyright legislation, without the publisher’s consent, is illegal and liable to prosecution. -

Current Molecular Understanding of Axenfeld-Rieger Syndrome
Current molecular understanding of Axenfeld-Rieger syndrome. Hjalt, Tord; Semina, Elena V Published in: Expert Reviews in Molecular Medicine DOI: 10.1017/S1462399405010082 2005 Link to publication Citation for published version (APA): Hjalt, T., & Semina, E. V. (2005). Current molecular understanding of Axenfeld-Rieger syndrome. Expert Reviews in Molecular Medicine, 7(25), 1-17. https://doi.org/10.1017/S1462399405010082 Total number of authors: 2 General rights Unless other specific re-use rights are stated the following general rights apply: Copyright and moral rights for the publications made accessible in the public portal are retained by the authors and/or other copyright owners and it is a condition of accessing publications that users recognise and abide by the legal requirements associated with these rights. • Users may download and print one copy of any publication from the public portal for the purpose of private study or research. • You may not further distribute the material or use it for any profit-making activity or commercial gain • You may freely distribute the URL identifying the publication in the public portal Read more about Creative commons licenses: https://creativecommons.org/licenses/ Take down policy If you believe that this document breaches copyright please contact us providing details, and we will remove access to the work immediately and investigate your claim. LUND UNIVERSITY PO Box 117 221 00 Lund +46 46-222 00 00 expert reviews http://www.expertreviews.org/ in molecular medicine Current molecular understanding of Axenfeld–Rieger syndrome Tord A. Hjalt and Elena V. Semina Axenfeld–Rieger syndrome (ARS) is a rare autosomal dominant inherited disorder affecting the development of the eyes, teeth and abdomen. -

A Robust Method for Addressing Pupil Dilation in Iris Recognition
A ROBUST METHOD FOR ADDRESSING PUPIL DILATION IN IRIS RECOGNITION By Raghunandan Pasula A THESIS Submitted to Michigan State University in partial fulfillment of the requirements for the degree of Computer Science – Master of Science 2016 ABSTRACT A ROBUST METHOD FOR ADDRESSING PUPIL DILATION IN IRIS RECOGNITION By Raghunandan Pasula The rich texture of the iris is being used as a biometric cue in several human recognition systems. Iris recognition systems are fairly robust to small changes in illumination and pose. However there are a number of factors that still adversely affect the performance of an iris matcher. These include occlusion, large deviation in gaze, low image resolution, long acquisition distance and pupil dilation. Large differences in pupil size increases the dissimilarity between iris images of the same eye. In this work, the degradation of match scores due to pupil dilation is systematically studied using Hamming Distance histograms. A novel rule-based fusion technique based on the aforemen- tioned study is proposed to alleviate the effect of pupil dilation. The proposed method computes a new distance score at every pixel location based on the similarities between IrisCode bits that were generated using Gabor Filters at different resolutions. Experiments show that the proposed method increases the genuine accept rate from 76% to 90% at 0.0001% false accept rate when comparing images with large differences in pupil sizes in the WVU-PLR dataset. The proposed method is also shown to improve the performance of iris recognition on other non-ideal iris datasets. In summary, the use of multi-resolution Gabor Filters in conjunction with a rule-based integration of decisions at the pixel (bit) level is observed to improve the resilience of iris recognition to differences in pupil size. -

Developmental Glaucoma
Our vision: Is for Australians to be free of glaucoma blindness Developmental Glaucoma Developmental Glaucoma is an umbrella term for a glaucoma due to a relatively rare group of eye disorders characterised by abnormal development of the front part of the eye known as the anterior chamber. People with this underlying anterior segment dysgenesis (ASD) have a significantly increased risk of glaucoma developing. ASD is often caused by a change (mutation) in a gene that drives the development of the front of the eye, usually affecting both eyes, they may also be found in varying severity in multiple members of a family. Although present at birth some of these conditions may not be discovered until a routine eye examination of an older child or adult is performed. Glaucoma can occur at any age. Ophthalmologists may use the term Anterior Segment Dysgenesis to cover several subgroups, the terminology is a little confused at times and some authors adopt the term Axenfeld-Rieger Syndrome after the notable Ophthalmologists that first described families with the condition and its glaucoma complications. 1. Axenfeld Anomaly · Strands connecting iris to Schwalbe’s line (peripheral cornea) 2. Rieger anomaly · Abnormal pupil shape and location (corectopia) · Extra holes in the iris / multiple pupils (polycoria) · Thin Iris (Iris Hypoplasia) 3. Rieger syndrome – iris anomalies and other body anomalies: · Distinctive facial features – widely spaced eyes (hypertelorism) · Dental abnormalities – small teeth, fewer than normal teeth · Extra skin folds around the belly button (redundant umbilical skin) Also included under the broad term anterior segment dysgenesis can be: 4. Aniridia · Partial or complete absence of iris development 5. -

Whole Exome Sequencing in Coloboma/Microphthalmia: Identification of Novel and Recurrent Variants in Seven Genes
G C A T T A C G G C A T genes Article Whole Exome Sequencing in Coloboma/Microphthalmia: Identification of Novel and Recurrent Variants in Seven Genes Patricia Haug 1 , Samuel Koller 1 , Jordi Maggi 1 , Elena Lang 1,2, Silke Feil 1, Agnès Wlodarczyk 1, Luzy Bähr 1, Katharina Steindl 3, Marianne Rohrbach 4 , Christina Gerth-Kahlert 2,† and Wolfgang Berger 1,5,6,*,† 1 Institute of Medical Molecular Genetics, University of Zurich, 8952 Schlieren, Switzerland; [email protected] (P.H.); [email protected] (S.K.); [email protected] (J.M.); [email protected] (E.L.); [email protected] (S.F.); [email protected] (A.W.); [email protected] (L.B.) 2 Department of Ophthalmology, University Hospital and University of Zurich, 8091 Zurich, Switzerland; [email protected] 3 Institute of Medical Genetics, University of Zurich, 8952 Schlieren, Switzerland; [email protected] 4 Division of Metabolism and Children’s Research Centre, University Children’s Hospital Zurich, 8032 Zurich, Switzerland; [email protected] 5 Neuroscience Center Zurich (ZNZ), University and ETH Zurich, 8006 Zurich, Switzerland 6 Zurich Center for Integrative Human Physiology (ZIHP), University of Zurich, 8006 Zurich, Switzerland * Correspondence: [email protected] † Both authors contributed equally to this work. Abstract: Coloboma and microphthalmia (C/M) are related congenital eye malformations, which can cause significant visual impairment. Molecular diagnosis is challenging as the genes associated to date with C/M account for only a small percentage of cases. Overall, the genetic cause remains unknown in up to 80% of patients. -

Monocular Vs Binocular Diplopia BRENDA BODEN, CO PARK NICOLLET PEDIATRIC and ADULT STRABISMUS CLINIC Monocular Diplopia
Monocular vs Binocular Diplopia BRENDA BODEN, CO PARK NICOLLET PEDIATRIC AND ADULT STRABISMUS CLINIC Monocular Diplopia Patient sees double vision with ONE eye open Second image appears as an OVERLAP or GHOST image Monocular Diplopia How to test? Cover test: cover each eye and ask the patient if they see single or double Pinhole: monocular diplopia will likely resolve Monocular Diplopia Causes Refractive Cornea abnormalities High astigmatism Keratoconus Tear Film Insufficiency Lens abnormalities Early tear break up time Lens opacities Dry eye syndrome IOL decentrations where the edge of lens is within the visual axis Abnormalities in blink Change in refractive error (anisometropia) Retinal Pathology s/p ocular surgery Maculopathy due to fluid, hemorrhage, or fibrosis (epiretinal membranes are the most Refractive surgery can cause irregular symptomatic) astigmatism and ocular aberrations Polycoria after iridectomy Monocular Diplopia Additional Testing Refractive Macular Pathology Pinhole, optical aberrations can be caused from Fundus exam irregular astigmatism OCT Refract with retinoscopy or over hard contact Amsler Grid lens Let patient dial in astigmatism axis Cornea abnormalities Slit lamp exam Tear Film Insufficiency Corneal topography instruments Early tear film break up time or Schirmer test Use artificial tear to see if symptoms resolve Binocular Diplopia Patient sees double vision with BOTH eyes open A A Vertical and Horizontal Diplopia Vertical Diplopia Binocular Diplopia How to test? Covering -

A Simple Surgical Technique to Repair Large Iridodialysis
68 DJO P-ISSN 0972-0200 A Simple Surgical Technique to Repair Large Iridodialysis Manpreet Kaur, Ashish Bajaj, Madhavi Sharma Sankara Eye Hospital, Ludhiana, Punjab, India A large and clinically symptomatic iridodialysis often requires surgical repair. In literature, many complex and surgically complicated techniques have been described which are not possible for a general ophthalmologist to replicate in routine operation theater settings. We describe a simple technique Summary of repairing a large iatrogenic iridodialysis and implantation of a posterior-iris-fixated intraocular lens (IOL) in a single-sitting. We found it to be a safe, less traumatic, simple surgery which requires minimum instrumentation, provides maximum patient comfort and has satisfactory cosmetic results. Delhi J Ophthalmol 2017;28;68-9; Doi; http://dx.doi.org/10.7869/djo.299 Brief Communication Keywords: large iridodialysis, coredialysis, intraocular iris-claw lens Introduction Iridodialysis is the separation of iris root from its attachment at the ciliary body. Etiologically, the most common cause is ocular trauma, followed by complicated intraocular surgery and rarely spontaneous or congenital variety may be noted. Its pathogenesis is explained by the fact that the iris root is the thinnest and weakest portion of the iris stroma, hence more prone for detachment from the ciliary body after any traumatic insult having impact at the iris root.1 A small localised and clinically insignificant (no diplopia or visual disturbances) iridodialysis may not require any surgical intervention. However, a large and clinically symptomatic iridodialysis often require surgical repair. The upper eyelid covers the superior iridodialysis region and prevents the symptoms while the inferior and infero-nasal ones are usually symptomatic.