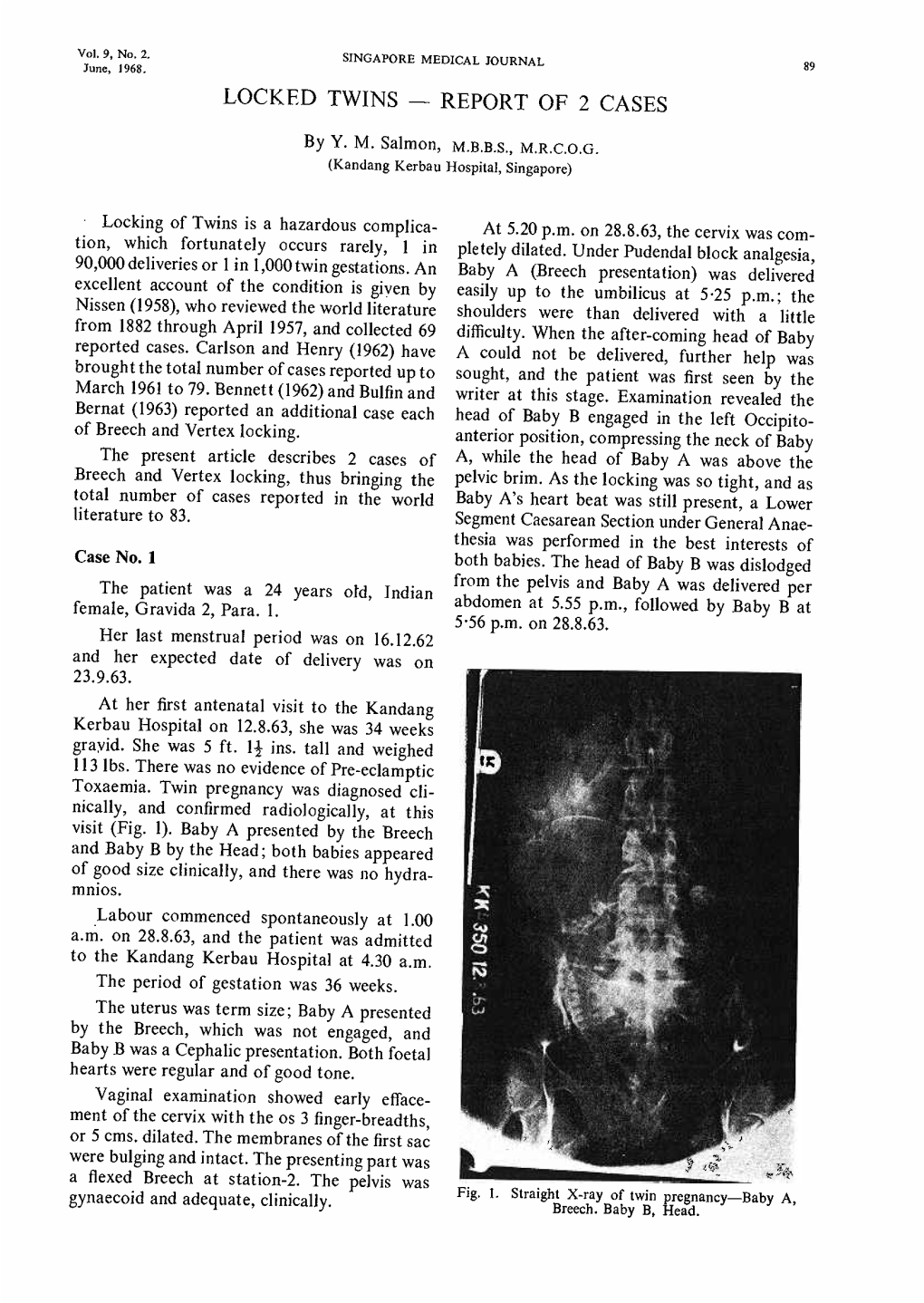
Locked Twins - Report of 2 Cases
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

ABCDE Acronym Blood Transfusion 231 Major Trauma 234 Maternal
Cambridge University Press 978-0-521-26827-1 - Obstetric and Intrapartum Emergencies: A Practical Guide to Management Edwin Chandraharan and Sir Sabaratnam Arulkumaran Index More information Index ABCDE acronym albumin, blood plasma levels 7 arterial blood gas (ABG) 188 blood transfusion 231 allergic anaphylaxis 229 arterio-venous occlusions 166–167 major trauma 234 maternal collapse 12, 130–131 amiadarone, overdose 178 aspiration 10, 246 newborn infant 241 amniocentesis 234 aspirin 26, 180–181 resuscitation 127–131 amniotic fluid embolism 48–51 assisted reproduction 93 abdomen caesarean section 257 asthma 4, 150, 151, 152, 185 examination after trauma 234 massive haemorrhage 33 pain in pregnancy 154–160, 161 maternal collapse 10, 13, 128 atracurium, drug reactions 231 accreta, placenta 250, 252, 255 anaemia, physiological 1, 7 atrial fibrillation 205 ACE inhibitors, overdose 178 anaerobic metabolism 242 automated external defibrillator (AED) 12 acid–base analysis 104 anaesthesia. See general anaesthesia awareness under anaesthesia 215, 217 acidosis 94, 180–181, 186, 242 anal incontinence 138–139 ACTH levels 210 analgesia 11, 100, 218 barbiturates, overdose 178 activated charcoal 177, 180–181 anaphylaxis 11, 227–228, 229–231 behaviour/beliefs, psychiatric activated partial thromboplastin time antacid prophylaxis 217 emergencies 172 (APTT) 19, 21 antenatal screening, DVT 16 benign intracranial hypertension 166 activated protein C 46 antepartum haemorrhage 33, 93–94. benzodiazepines, overdose 178 Addison’s disease 208–209 See also massive -

Determinants, Incidence and Perinatal Outcomes of Multiple Pregnancy Deliveries in a Low-Resource Setting, Mpilo Central Hospital, Bulawayo, Zimbabwe
MOJ Women’s Health Review Article Open Access Determinants, incidence and perinatal outcomes of multiple pregnancy deliveries in a low-resource setting, Mpilo Central Hospital, Bulawayo, Zimbabwe Abstract Volume 8 Issue 2 - 2019 Background: Multiple pregnancies are high risk pregnancies compared to singletons. Solwayo Ngwenya They may result in poor feto-maternal outcomes. Traditionally, these pregnancies Department of Obstetrics and Gynecology, Mpilo Central are associated with anaemia, preeclampsia, preterm deliveries and postpartum Hospital, Zimbabwe haemorrhage. In low-resource settings, these women and their babies may face increased risks of poor perinatal outcomes. The objective of this study was to Correspondence: Solwayo Ngwenya, Department of document for the first time the determinants, incidence and perinatal outcomes of Obstetrics and Gynecology, Mpilo Central Hospital, P.O. Box multiple pregnancies for Mpilo Central Hospital. 2096, Vera Road, Mzilikazi , Bulawayo, Matabeleland, Zimbabwe, Tel +263 9 214965, Email Methods: This was a retrospective descriptive study covering the period between 1 January 2017 and 31 December 2017 in a tertiary teaching hospital. A paper data Received: December 31, 2018 | Published: March 05, 2019 collection sheet was used to collect the information. All twin/triplet deliveries >24 weeks gestation born at the labour ward were included in the study. The data was then analysed. Results: The incidence of multiple pregnancy at Mpilo Central Hospital was 1.7%. The 20-25 year old age group had the highest percentage at 25.5%. Nulliparous women had the highest percentage at 28.4% of the patients. Booked/referred patients constituted the majority at 45.4%, followed by instutional booked at 39.0%. -

Mortality Perinatal Subset, 2013
ICD-10 Mortality Perinatal Subset (2013) Subset of alphabetical index to diseases and nature of injury for use with perinatal conditions (P00-P96) Conditions arising in the perinatal period Note - Conditions arising in the perinatal period, even though death or morbidity occurs later, should, as far as possible, be coded to chapter XVI, which takes precedence over chapters containing codes for diseases by their anatomical site. These exclude: Congenital malformations, deformations and chromosomal abnormalities (Q00-Q99) Endocrine, nutritional and metabolic diseases (E00-E99) Injury, poisoning and certain other consequences of external causes (S00-T99) Neoplasms (C00-D48) Tetanus neonatorum (A33 2a) A -ablatio, ablation - - placentae (see alsoAbruptio placentae) - - - affecting fetus or newborn P02.1 2a -abnormal, abnormality, abnormalities - see also Anomaly - - alphafetoprotein - - - maternal, affecting fetus or newborn P00.8 - - amnion, amniotic fluid - - - affecting fetus or newborn P02.9 - - anticoagulation - - - newborn (transient) P61.6 - - cervix NEC, maternal (acquired) (congenital), in pregnancy or childbirth - - - causing obstructed labor - - - - affecting fetus or newborn P03.1 - - chorion - - - affecting fetus or newborn P02.9 - - coagulation - - - newborn, transient P61.6 - - fetus, fetal 1 ICD-10 Mortality Perinatal Subset (2013) - - - causing disproportion - - - - affecting fetus or newborn P03.1 - - forces of labor - - - affecting fetus or newborn P03.6 - - labor NEC - - - affecting fetus or newborn P03.6 - - membranes -
Multiple Gestation DEFINITION
Multiple Gestation DEFINITION Any pregnancy which two or more embryos or fetuses present in the uterus at same time. It is consider as a complication of pregnancy due to : ∗ The mean gestational age of delivery of twins is approximately 36w. ∗ The perinatal mortality &morbidity increase. TERMINOLOGY ∗ Singletons - one fetus ∗ Twins - tow fetuses. ∗ Triplets - three fetuses. ∗ Quadruplets - four fetuses. ∗ Quintuplets - five fetuses. ∗ Sextuplets - six fetuses. ∗ Septuplets - seven fetuses. INCIDIENCE AND EPIDEMIOLOGY ∗ The incidence of multiple pregnancy is approximately 3% (increase annually due to ART ). ∗ Monozygotic twins ( approx. 4 in 1000 births ). ∗ Triplet pregnancies ( approx. 1 in 8000 births ). ∗ Conjoined twins ( approx. 1 in 60,000 births ). ∗ Multiple gestation increase morbidity & mortality for both the mother & the fetuses. ∗ The perinatal mortality in the developed countries Twins = 5 – 10 % births. Triplets = 10 – 20 % births ∗ Hellin’s Law Twin = 1:80 Triplets = 1:80² Quadruplets = 1:80³ RISK FACTORS (only for dizygotic pregnancy) ∗ Ethnicity (afroamerican race > caucasian race > asian race) ∗ Maternal age > 35 years (due to increase gonadotrophins production) ∗ Increases with parity ∗ Heredity usually on maternal side ∗ Induction of ovulation, 10% with clomide and 30% with gonadotrophins IMPORTANT NOTES ! ∗ Monozygotic twins having same sex & blood group ∗ Process of formation of chorion is earlier than formation of amnion ∗ Dizygotic twins must be dichorionic/diamniotic. ∗ There is no dichorionic/ monoamniotic. DIZYGOTIC PREGNANCY Dizygotic twins (fraternal) : ∗ Most common represents 2/3 of cases. ∗ Fertilization of more than one egg by more than one sperm. ∗ Non identical ,may be of different sex. ∗ Two chorion and two amnion. ∗ Placenta may be separate or fused. ∗ “each fetus is contained within a complete amniotic- chorionic membrane “ DIZYGOTIC PREGNANCY MONOZYGOTIC PREGNANCY ∗ Constitutes 1/3 of twins ∗ These twins are multiple gestations resulting from cleavage of a single, fertilized ovum. -
Obstetric Cases
OBSTETRIC CASES Dr Ishita Saini Important tips: Settings : GP : Rural / Metro Hospital Age of the patient Presenting complaint (vitals unstable , bleeding, pain , vomiting) hemodynamic stability (resuscitation room , iv line, take blood for investigation and manage accordingly) Tasks Obstetrics history: Menstrual history: LMP (corresponding to gestational age or not), regularity, confirm pregnancy Office test- Pregnancy symptoms (morning sickness, nausea vomiting, breast tenderness) if pregnancy not confirmed. History of any miscarriages or previous pregnancies. How was delivery? NVD/CS? Sexual history: STI? Contraception? PAP smear? Regular antenatal checks? Blood group? Folic acid (0.5 mg/ day),USG at 18-20 weeks (single pregnancy/multiple, placenta position) Sweet drink test and 26/28 weeks (OGTT diagnostic), bug test (GBS) at 36 weeks. Passed 20 weeks- baby kicking well or not Support – support to be taken through out pregnancy and delivery. Smoking, alcohol, illicit drugs, Pap smear (can be done after 20 weeks) any medical conditions? Surgeries? Regular Medicine? 5P’s Period Pills Previous pregnancy Pap Smear Partner Obstetrics examination: General appearance : Pallor, Icterus, clubbing, cyanosis, edema Vitals: Blood pressure, temperature, RR, SpO2 Per Abdomen examination: Before 12 weeks : any mass ( multiple pregnancy, H. mole). After 12 weeks : Fundal height (from symphysis pubis to upper part of abdomen), FHR : 110-160 (in distress do CTG), Lie and presentation. Pelvic exam: Inspection : bleeding, rash, discharge, vesicles Sterile speculum exam: cervical os : open (inevitable abortion, incomplete abortion, preterm labour. Closed (threatened abortion) Per vaginal and bimanual exam: Don’t go for PV exam after 20 weeks. Contraindications PROM APH hemorrhages (Placenta previa, abruptio placenta) not sexually active females. -
Abnormalities of Labor and Delivery
Abnormalities of labour and delivery Artúr Beke MD PhD Semmelweis University Department of Obstetrics and Gynecology Department of Obstetrics and Gynecology Baross Street Abnormalities of labor and delivery • 1. Fetal malpositions and malpresentations • 2. Uterine dystocia • 3. Shoulder dystocia • 4. Premature rupture of the membranes • 5. Fetal distress • 6. Preterm delivery • 7. Twin delivery Artur Beke - Abnormalities of Labour and Delivery - 2019 1. Fetal malposition and malpresentations Artur Beke - Abnormalities of Labour and Delivery - 2019 Fetal malposition and malpresentations • A./ Abnormal presentation – Breech presentation – Transverse or oblique lie (shoulder presentation) • B./ Abnormal position – High sagittal position – Obliquity • C./ Abnormalities of flexion – Deflexion of the head • D./ Abnormalities of rotation Artur Beke - Abnormalities of Labour and Delivery - 2019 A./ ABNORMAL PRESENTATION • Cephalic presentation 96.5% • Breech presentation 3.0% • Transverse or oblique lie 0.5% Artur Beke - Abnormalities of Labour and Delivery - 2019 Breech presentation • Fetal buttocks or lower extremities present • 3% of all deliveries • At the 30th week 25% of fetuses • After 36th week no change in position Artur Beke - Abnormalities of Labour and Delivery - 2019 Types of breech presentation • Frank breech - Extended legs (Simple) (65%) • Complete breech - Flexed legs (25%) • Incomplete breech - Footling or knee presentation (10%) Artur Beke - Abnormalities of Labour and Delivery - 2019 Diagnosis of breech presentation • Leopold -

Outcome of Labor in Twin Gestation at a Tertiary Institution in a Developing Nation: a 15-Year Review Olukayode Akinlaja1* and Rose Anorlu2
Akinlaja, Obstet Gynecol cases Rev 2014, 1:1 ISSN: 2377-9004 Obstetrics and Gynaecology Cases and Reviews Review article: Open Access Outcome of Labor in Twin Gestation at a Tertiary Institution in a Developing Nation: A 15-Year Review Olukayode Akinlaja1* and Rose Anorlu2 1College of Medicine, University of Tennessee Health Science Center, USA 2Lagos University Teaching Hospital, Lagos, Nigeria *Corresponding author: Olukayode A. Akinlaja, MD, College of Medicine, University of Tennessee Health Science Center, USA, Tel: 4237787489 growth restriction, locked twins, retained 2nd twin, congenital Abstract anomalies, cord prolapse with twin-twin transfusion and twin Objective: To describe our experience with twin gestation in a reversed arterial perfusion syndromes seen with monochorionic developing nation tertiary institution. placentation while maternal complications include hyperemesis Method: All cases of twin gestation at the Lagos University Teaching gravidarum, anemia, pregnancy induced hypertension, pre- Hospital over a 15-year period were retrospectively reviewed. eclampsia, eclampsia, polyhydramnios, preterm delivery, placental Results: There were 642 twin births out of a total of 28,472 Previa, postpartum hemorrhage, increased prenatal admission and deliveries, a ratio of 1:44. Peak age at occurrence was 28 with only operative deliveries [8]. 6% (39) being grand multipara. 66.4% (426) delivered preterm at about 36 weeks and 74.5% (478) had the leading twin in cephalic Despite the improvement in maternity and neonatal services, the presentation while the mean birth weight for twin A was 2.43kg high risk of perinatal morbidity and mortality associated makes it and twin B 2.3kg with 14.8%(95) having discordant weight. Only imperative for efforts to be intensified to ensure optimal care. -

Dr. Shushila Kharkwal Locked Twins-A Rarity ABSTRACT Gynaecology Dr
Original Research Paper VOLUME-6 | ISSUE-3 | MARCH - 2017 • ISSN No 2277 - 8179 | IF : 4.176| IC Value : 78.46 Gynaecology locked twins-a rarity KEYWORDS: locked twins, monochorionic monoamniotic twins, Dr. Shushila Professor , Department of OBG, MLB Medical College, Jhansi, India Kharkwal Dr. Sanjaya Sharma Professor& Head , Department of OBG, MLB Medical College, Jhansi, India Dr. Heena Khan JR-3,Department of OBG, MLB Medical College, Jhansi, India Dr. Rajkumar Mishra JR-3,Department of OBG, MLB Medical College, Jhansi, India ABSTRACT Locked twins usually occur when the after-coming head of the first beech fetus is locked with the head of the second cephalic fetus. A case of locked twins delivered by caesarean section is reported with one twin surviving. patient was an unbooked case and had undiagnosed twin pregnancy with head arrest of first twin in obstructed labour. Fetal morbidity and mortality can be avoided in such situations by identifying the potential cases, radiological diagnosis and timely done caesarean section. Introduction pelvis. In twin locking, the inferior aspect of each twin's chin is Locked twins usually occur when the after-coming head of the first apposed to each other in a vertical axis. beech fetus is locked with the head of the second cephalic fetus. is complication of twin delivery occurs rarely 1 in 90,000 deliveries or 1 In recent years, the trend has been for greater use caesarean sections in every 1000 twin deliveries. We report a rare condition of an and ultrasound in managing twin deliveries. It rarely happens in unbooked case of interlocked twins in advanced second stage of current obstetric practice , since the presentation of both twins can labour with obstructed labour. -

Locked Twins 4
LOCKED TWINS (Case Reports) by PRAFUL H. MUNSHI, * M.D. and JYOTIKA c. SHAH,** M.D., D.G.O., D.A. Being a rare condition the occur ted with a history of 9 months' amenorrhoea rence of locked twins is very interest and labour pains. She had 4 full-term nor mal deliveries, all alive. The patient was ing. According to Braun, as stated by fairly well built and nourished. There was Munro Kerr, it only occurred once in mild degree of anaemia and slight oedema 90,000 deliveries in the two Vienna was present over the legs. Pulse was 100/ clinics. According to Harder, it is not min. and B.P. was 150/ 90. Systemic exam ination detected nothing abnormal. The so uncommon. He derived the latter abdomen was found bigger than usual. Fun fact from his observation in the last dal height was 16" while abdominal girth few years. Nissen had reviewed about was 44". Multiple foetal parts were felt 70 collected cases of locked twins. Ac and 2 heads at the lower pole of cording to him, 45 cases of locked uterus. Two separate foetal heart sounds twins, both babies having vertical lie, were heard. The cervix was 2 ems dilated. The membranes were bulging. The pre have been described till 1957. Law sentation could not be properly made out. rence (Leeds) described 3 · cases of Pelvis was normal. locked twins and tabulated 28 previ A diagnosis of twin pregnancy was made ously recorded cases. The types of tentatively and the patient was observed locking in 31 cases were as follows:- vigilantly. -

Fetal Interlocking Complicating Twin Pregnancy: a Case Report Aniekan M
Trop J Obstet Gynaecol, 23 (2), October 2006 Fetal Interlocking Complicating Twin Pregnancy: A Case Report Aniekan M. Abasiattai, Emem A. Bassey and Aniefiok J. Umoiyoho Department of Obstetrics & Gynaecology, University Uyo Teaching Hospital, Uyo, Nigeria Abstract Fetal interlocking is a potentially catastrophic intrapartum situation and an extremely rare complication of multiple pregnancy. This is the case report of a 27 year old primigravida who presented at the University of Uyo teaching hospital after a traditional birth attendant had failed to deliver the after coming head of her baby. Clinical examination revealed locked twins, with demise of the first twin. The patient was successfully managed with decapitation of the first twin while the second twin was delivered by vacuum extraction with good Apgar scores. This report also reviews literature on interlocked twins and its management. Key Words: Fetal Interlocking, Twin Pregnancy [Trop J Obstet Gynaecol, 2006, 23:184-185] Introduction Fetal interlocking is an extremely rare complication of from the introitus. The after coming head was felt multiple pregnancy and a potentially catastrophic above the head of the second twin in the pelvis. There intrapartum complication 1-4. It has been estimated to was no cord pulsation. The pelvis was ajudged to be occur in less than 1 in 1000 twin deliveries 5,6. it prevents adequate for vaginal delivery. A diagnosis of locked spontaneous delivery and is associated with a fetal twins with demise of the first twin was made. A mortality rate greater than 31% 5,7. It occurs more decision to decapitate the first twin and deliver the commonly in mono-amniotic twin pregnancy, in second twin was then taken. -

Locked Twins: a Rarity
Case Report Locked Twins: A Rarity Borah T, Das A Department Obstetrics and Gynecology, North Eastern Indira Gandhi Regional Institute of Health and Medical Sciences, Mawdiangdiang, Shillong, Meghalaya, India Address for correspondence: Abstract Dr. Tulon Borah, Department of Obstetrics and Gynecology, Locked twins is a rare, hazardous obstetric complication. Herein, we report the rare condition NEIGRIHMS, Shillong, of an unbooked case of locked twin that attended our labor room in late stage of labor with Meghalaya ‑ 793 018 India. arrested after‑coming head of the first twin, which was dead. Caesarean section was performed E‑mail: [email protected] to save the second baby. Antenatal diagnosis of twin gestation with leading twin breech and second twin cephalic presentation raises index of suspicion of potential locked twin. Timely done caesarean delivery could have avoided the fetal death. Keywords: Breech presentation, Interlocking twin, Perinatal death Introduction lower segment caesarean section (LSCS) was performed in the interest of the surviving baby. After disimpaction of the head Locked twins usually occur when the after-coming head of vaginally, the second baby weighing 1.2 kg was delivered the first breech fetus is locked with the head of the second abdominally by breech. The baby was then handed over to the cephalic fetus. Of the different etiological factors, the most pediatrician. The first baby weighing 1 kg, which was already important are the ageand parity of the mother and the size dead, was delivered vaginally. Placental examination showed of the twins. A large pelvis with relatively small infants and it to be a monochorionic diamniotic twin. -

Twin Births and Their Complications in Women of Low Socioeconomic Profile Original Article
Original Article Twin births and their complications in women of low socioeconomic profile Saima Aziz, Nargis Soomro Department Obstetrics & Gynaecology, Dow University of Health Sciences & Civil Hospital Karachi. Corresponding Author: Saima Aziz. Email: [email protected] Abstract Objective: To determine the frequency of twin births and their foetomaternal complications in women of low socioeconomic profile. Methods: The cross-sectional study was conducted from January 2009 to December 2010 at the Obstetrics and Gynaecolgy Unit I, Civil Hospital, Karachi. Patients with twin pregnancy giving birth beyond 24 weeks, were selected by non-probability purposive sampling. Data on patient characteristics, gestation, antepartum and peripartum complications, chorionicity, mode of delivery and perinatal outcome was recorded and analysed through SPSS 16. Results: Out of 6077 deliveries during the study period, 119 twin births gave a frequency of 19.58/1000 births. Patients' mean age was 27.51±4.2 years, mean parity 2.4±2.2 and mean gestational age was 34.76±3.4 weeks. Unbooked and referred patients were 96 (80.67%). Final paired outcome was alive twin pairs in 74 (62.18%) cases, stillbirth in 7 (5.88%), neonatal deaths in 10 (8.40%). Perinatal mortality rate was 277/1000 twin births. Most frequent foetal complications were low birth weight (n=84; 70.58%), pre-term births (n=70; 58.82%) and intrauterine growth restriction (n=59; 49.57%). The second twin was at significantly higher risk (p< 0.05). Monochorionic twins had significantly high rates of stillbirths than dichorionic (p = 0.023). Most frequent maternal complications comprised pre-term labour (n=56; 47.05%), severe anaemia (n=22; 18.48%), hypertensive disorders (n=19; 15.96%) and postpartum haemorrhage (n=10; 8.40%).