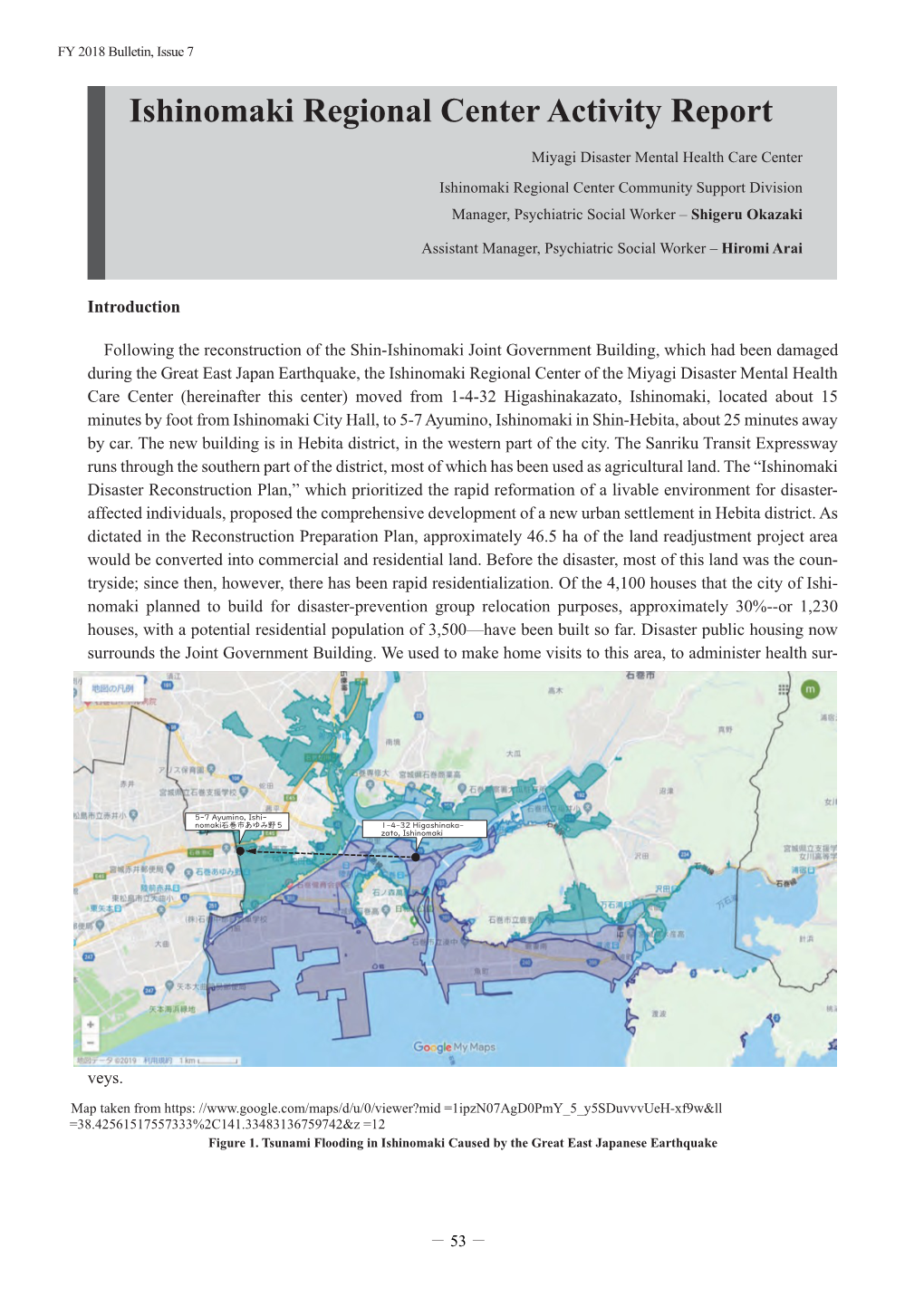
Ishinomaki Regional Center Activity Report
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Matsushima Bay As an Early Holocene Coastal Mega-Landslide, Northeast Japan
Matsushima Bay as an Early Holocene coastal mega-landslide, Northeast Japan Shuichi Hasegawa (Kagawa University, Japan) Timihiro Sawada (Sawa Soft Science, Japan) Ranjan Kumar Dahal (Kagawa University, Japan and Tribhuvan University, Nepal) Atsuko Nonomura (Kagawa University, Japan) Minoru Yamanaka (Kagawa University, Japan) Abstract. Matsushima, a group of island at Matsushima Bay visited both Matsushima and Kisakata. He composed three in Miyagi Prefecture, northeast Japan, is one of the three haiku poems for Kisakata, but he could not express his famous scenic spots of Japan. It is composed of more than excitement in a haiku poem for Matsushima. 200 islands in Matsushima Bay and the islands just out into Matsushima and Matsushima Bay have long been the sea. Topographically Matsushima Bay suddenly breaks considered as a typical submerged coast, but they are inferred the gently concaved coastline from Sendai Bay to Ishinomaki to have been formed by a coastal mega-landslide in middle Bay. Matsushima and Matsushima Bay have been considered Holocene age from geological and topographical inferences. as a typical submerged coast, but they are inferred to have been formed by a coastal mega-landslide in middle Holocene age from geological and topographical evidences. Keywords. Mega-landslide, Holocene, Jomon transgression, Active fault, topography 1. Introduction Mega-landslides due to volcanic activities and earthquakes have caused severe damage to the surrounding areas. Sector collapse of volcanoes is one of the most destructive landslides. Debris avalanche deposits from a sector collapse generally form strange topography punctuated by hundreds of small hills, ridges and closed depressions. The 1792 Mayuyama sector collapse of Unzen volcano in Kyushu, southern Japan, caused debris avalanche which flowed through ancient Shimabara City and entered the sea. -
The 34Th Issue
H F H J News Letter 34 2015 April Habitat for Humanity Japan Newsletter Issue 34 News from the Field Four Years with Tohoku Jimmy Carter Work Project An Interview with Model Arisa Kamada Carter Work Project Miyagi Jimmy Carter Work Project 2015 in Nepal! Each year since 1984, former President Carter and his wife, Rosalynn, give a week of their time to help us improve and build homes. The Jimmy & Rosalynn Carter Work Project helps raise awareness of the critical need for simple, decent and affordable housing. This year, the 32nd annual Jimmy & Rosalynn Carter Work Project will be held in Pokhara, Nepal for 6 days from November 1 to 6. Nepal is located at the Himalayan foot, and is said to be one of the poorest countries in the world. There are many ways to be a part of this exciting event. How can I participate? Traveling hammer – Volunteer – We will Invitation Nepali dinner Let's do a good deed build 100 houses for the dinner for a good cause. with the hammer of with 2,000 volunteers with the Carters. hope which in a week at travels around the Himalayan foot. the Asia After Pacific region! Before Youth Build Asia-Pacific region Youths unite against poverty housing The people who cannot live in decent houses reach 1.6 Habitat mobilized 800,000 volunteers from 11 countries billion worldwide, and it is said that half of them live here and supported 1,700 households. This year, we expanded in the Asia-Pacific region. Habitat Youth BUILD (HYB) is a its scale with 15 countries participating. -

Strategies of the 77 Bank, Ltd Growth Strategy
Strategies of The 77 Bank, Ltd Growth Strategy Best Consulting Bank Human Resource Development In order to become a bank that is truly supported by its customers and to establish a solid management base for the future, we have set the image of the bank we aspire to become as the following, and actively trained specialist resources. Interview 01 “Best Consulting Bank” that responds to customersʼ needs by offering the optimum solutions Striving to solve the issues of quality assurance Corporate Support Department and manpower shortage on the front line of manufacturing. Kei Akama I was assigned to Tohoku Electronics Industry Co., Ltd. with Tohoku Electronics Industry has about 1,000 employees in the headquarters in Ishinomaki City, Miyagi Prefecture for one year entire group, I was forced to be keenly aware of the issue of the under the Local Company Trainee program that started in 2018. shortage of manpower at the manufacturing front line. I believe I was assigned to the Quality Assurance Department, where I that these valuable experiences as a trainee at a local company dealt with automobile manufacturers and interacted with manu- can be utilized in my current work. I am currently working in the facturing sites to ensure the quality of automobile-related parts. Corporate Support Office, providing support mainly to custom- I was interested in the manufacturing industry, including ers in the fishery processing industry in the coastal areas of the automobiles and machinery, and I thought I had acquired some prefecture that are still on the road to recovery from the Great prior knowledge before I was transferred to the company, but I East Japan Earthquake. -

Historical Fish Specimens Collected from the Tohoku District by the Saito Ho-On Kai Museum of Natural History
Bull. Natl. Mus. Nat. Sci., Ser. A, 35(1), pp. 9–54, March 22, 2009 Historical Fish Specimens Collected from the Tohoku District by the Saito Ho-on Kai Museum of Natural History Keiichi Matsuura1, Gento Shinohara2 and Masanori Nakae1 1 Collection Center, National Museum of Nature and Science, 3–23–1 Hyakunin-cho, Shinjuku-ku, Tokyo, 169–0073 Japan E-mail: [email protected]; [email protected] 2 Department of Zoology, National Museum of Nature and Science, 3–23–1 Hyakunin-cho, Shinjuku-ku, Tokyo, 169–0073 Japan E-mail: [email protected] Abstract The fish collection of the Saito Ho-on Kai Museum of Natural History was transferred to the National Museum of Nature and Science, Tokyo in February 2006. Ninety percent of the fish collection contains specimens collected from the Tohoku District during the period from 1930 to 1933 when natural environments of Japan were in good condition for various groups of fishes. The fish specimens from the Tohoku District were classified into 361 species/subspecies of 273 genera belonging to 131 families of 31 orders. A list of the species is shown with remarks on distribution. Key words: Fish specimens, Saito Ho-on Kai Museum, Tohoku District, inventory. stead of natural sicence. The museum has tried to Introduction keep its activity at the level before the war, but it The Saito Ho-on Kai Museum was established failed to do so because of financial difficulties. In in November 1933 in Sendai City, Miyagi Pre- 2005, the Saito Ho-on Kai Museum of Natural fecture, Japan. -

TOMODACHI J&J Disaster Nursing Training Program
TOMODACHI J&J Disaster Nursing Training Program Commemorative publication *Please refrain from using information or images included in this publication or posting on social networking sites or other online services without the permission of the U.S.-Japan Council (Japan) or Johnson & Johnson. Study Disaster Nursing Japan is a nation frequently affected by earthquakes and other disasters. Many precious lives were lost in 2011 after the Tohoku earthquake, the Great East Japan Earthquake. However, many lives were also saved by the doctors and nurses from around the country who rushed to the area to lend a hand. The TOMODACHI J&J Disaster Nursing Training Program was launched in 2015, and in the following three years, a total of 28 students have joined the program to study disaster nursing. The program provides them with a deeper understanding of what it means to provide nursing care in a time of disaster, and the knowledge they need to do so. It is our greatest wish that these students will lead the field of disaster nursing in Japan into the future. Table of Contents 03 What is the TOMODACHI Initiative? 25 Future of the Program 27 Future Direction 05 History of the Program 29 Post-program Life for Participants 07 Program Participants 31 Special Thanks 13 Program Mentors 34 Sponsorship and Support 15 Program Flow 17 Pre-Trip Seminars 19 U.S. Study Tour 23 Post-Trip Seminars 01 02 What’s “TO MODACHI”? The TOMODACHI Initiative is a public-private partnership between the U.S.-Japan Council and the U.S. Embassy in Tokyo, with support from the Government of Japan. -

Increasing Incidence of Tuberculosis Infection in the Coastal Region of Northern Miyagi After the Great East Japan Earthquake
Tohoku J. Exp. Med., 2016, 238, 187-195Increasing Incidence of TB Infection after Tohoku Disaster 187 Increasing Incidence of Tuberculosis Infection in the Coastal Region of Northern Miyagi after the Great East Japan Earthquake Masahiro Sakurai,1 Tatsuya Takahashi,1 Miyako Ohuchi,1 Yuki Terui,1 Kouji Kiryu2 and Kazuo Shikano1 1Division of Health and Welfare, Miyagi Prefectural Government, Ishinomaki, Miyagi, Japan 2Division of Health and Welfare, Metropolitan Government, Tokyo, Japan On March 11, 2011, the Great East Japan Earthquake struck off the northeast coast of Japan. Within an hour of the earthquake, devastating tsunamis swept over the coastal region of the Miyagi Prefecture, facing Pacific Ocean. Accordingly, more than 400,000 residents were forced to stay at evacuation shelters. We investigated the changes in tuberculosis prevalence after the disaster. Annual data for all tuberculosis patients between April 1, 2009 and March 31, 2013 were extracted from the database of the Miyagi Prefectural Government. In the coastal region of Northern Miyagi, the number of tuberculosis patients increased in the post-disaster period (p < 0.001, 9.6 vs.19.1 per 100,000 people), compared to the pre-disaster period. In contrast, its prevalence did not change in the inland region of Northern Miyagi and the coastal and inland regions of Southern Miyagi. Importantly, in the inland and coastal regions of Northern Miyagi, the number of patients with latent tuberculosis infection (LTBI) increased in the post- disaster period (p < 0.001). Furthermore, in the coastal shelters, 11 evacuees with the history of contacting tuberculosis patients were diagnosed with LTBI, whereas no cases of LTBI patients were observed in the inland shelters. -

2016 Economic Census for Business Activity (Definitive Report) Tabulations Across Industries Summary of Census Results
2016 Economic Census for Business Activity (Definitive Report) Tabulations across Industries Summary of Census Results I Overview ..................................................................................................................................... 1 II Situations of Number of Enterprises, etc., Sales, and Added Value .......................................... 3 1. Number of Enterprises, etc., Sales, and Added Value ........................................................... 3 2. Added Value Ratio ................................................................................................................. 13 3. Sales by Business Activity ..................................................................................................... 14 4. Capital Investment ................................................................................................................. 18 5. Electronic Commerce (e-commerce) ..................................................................................... 24 6. Situation of Added Value by Prefecture ................................................................................ 27 III Situations of Number of Establishments and Number of Persons Engaged ............................. 29 1. Number of Establishments and Number of Persons Engaged by Industry Division.............. 29 2. Number of Persons Engaged by Status in Employment ........................................................ 33 3. Number of Establishments and Number of Persons Engaged by Size of Persons Engaged -

Response to the Great East Japan Earthquake in the Three Years from March 2011
Response to the Great East Japan Earthquake in the Three Years from March 2011 JICA has continued related supportive activities during Yolanda in the Philippines), which struck the middle part of the three years from the right after the earthquake of the Philippines on November 8 and 9, 2013, JICA provided March 11, 2011, to the present. In the beginning, the main information on the study of reconstruction processes from activity was direct support, including shelter for evacuees, large-scale disasters, and officials from Higashimatsushima dispatch of JICA staff and former volunteers, coordination of City, Miyagi Prefecture, visited the damage area and gave international organizations from overseas, and cooperation advice based on the experiences of the Great East Japan with NGOs, which played a central part in people’s support Earthquake. to the damage area. At the present time JICA engages JICA uses Japan’s experience of recovery and recon- in information-sharing and submission, compilation of struction from large-scale disasters, including the Great lessons learned from reconstruction efforts, and support to East Japan Earthquake, for international cooperation to international conferences. developing countries. Regarding the damage by Typhoon Haiyan (called (1) Accommodation of people unable to return home, shelter for evacuees, provision of disaster 1. prevention supplies and storage space, and donation of money collected Tohoku Earthquake (2) Dispatch of JICA staff to NGOs, municipalities, and universities, offering of office space -

Assessment of Tsunami Flood Situation from the Great East Japan Earthquake 55
Assessment of Tsunami Flood Situation from the Great East Japan Earthquake 55 Assessment of Tsunami Flood Situation from the Great East Japan Earthquake Hidetoshi NAKAJIMA and Mamoru KOARAI Abstract The massive tsunami from the 2011 off the Pacific Coast of Tohoku Earthquake (hereinafter referred to as the “Tohoku Pacific Coast Earthquake”) that occurred on March 11, 2011, caused devastating damages along the Pacific Coast. The GSI immediately formed an emergency team and started investigating to uncover the situation of tsunami damage. We emphasized on promptness in the beginning of the survey, created the "Tsunami flood area overview map" with a purpose of improving the accuracy in our best effort over time, and kept on distributing the maps to the municipalities of the affected areas, the national disaster response headquarters etc, while also releasing this information on the GSI website. In addition to calculating the areas of inundation by the municipalities and by land use, an attempt was made to analyze the distance and elevation reached by tsunami in coastal Miyagi Prefecture. Furthermore, elevation was measured precisely by aerial laser survey mainly on areas where ground subsidence occurred due to the earthquake, and high precision elevation data and the digital elevation topographic map have been prepared/provided. 1. Creating an inundation area overview map There are two types of error cause which are 1.1 Method of creation "interpretation error" and "error in transferring onto Immediately after the tsunami disasters triggered by topographic map". Since single (aerial) photographs are the Tohoku Pacific Coast Earthquake on March 11th, the used for the interpretation, difference in landform GSI decided to create an "Tsunami flood area overview interpretation skills has little effect on the former, whereas map" to find out the situation of tsunami damage, and landform interpretation skills would be required to minimize created a damage overview map and also discussed about the latter. -

Feel More Alive / in Higashi-Matsushima
Tohoku Shinkansen Shinkansen Tohoku Tohoku 4 Ishinomaki city Tsukidate IC JR Rikuu-East Line 47 45 Furukawa IC 108 JR Ishinomaki Line Sanriku Expressway Furukawa Misato Town Tohoku Expressway Naruse Ishinomaki Onagawa Oku-Matsushima IC JR Senseki Line Tomiya JCT Ishinomaki port IC JR Senzan Line Rifu JCT Sendai Higashi-Matsushima City Sendai Minami IC Higashi- 4 Wakabayashi JCT Matsushima City Sanriku Expressway Murata JCT Rikuzen-Akai Station Yamoto IC Higashi-Yamoto Station To Ishinomaki Higashi-Matsushima City Hall 45 Yamoto station Naruse Oku-Matsushima IC Japan Air Self-Defense Force, Matsushima Air Base Naruse JR Senseki Line River your Higashi-Matsushima guidebook! Discovery Center Higashi-Matsushima City Hall, Naruse Office Kazuma station Higashi-Matsushima Tourist Association Yamoto Seaside Park Rikuzen-Ono Station Town of Matsushima Yoshida River To Matsushima・ Nobiru Station Sendai Rikuzen-Otsuka Station Higashimatsushima City Great East Japan Earthquake Recovery Memorial Park Tona Station Ishinomaki Bay Oku-Matsushima Nobiru Beach Lane Hotel Oku-Matsushima Clubhouse Matsushima Bay KIBOTCHA Oku-Matsushima Pleasure Boat Information Center (in Aomina) Otakamori Satohama The Historical Museum of Jomon Village, Miyato Oku-Matsushima Island Murohama Oku-Matsushima Experience Network Ohama Sagakei Gorge Feel More Alive / Tsukihama in Higashi-Matsushima Transportation Guide Sendai station Tohoku Shinkansen Tokyo JR Senseki-Tohoku Line about 95 minutes about 40 minutes To the land of whispering winds and blue seas JR Senseki Line Matsushima -

Press Release
Press Release Press Release (This is provisional translation. Please refer to the original text written in Japanese.) April 25, 2012 Policy Planning and Communication Division, Inspection and Safety Division, Department of Food Safety To Press and those who may concern, Restriction of distribution of foods based on the Act on Special Measures Concerning Nuclear Emergency Preparedness, direction of Director-General of the Nuclear Emergency Response Headquarters Today, based on the results of inspections conducted until yesterday and in the lights of the Nuclear Safety Commission’s advice, the Nuclear Emergency Response Headquarters has issued restriction of distribution for Governors of Iwate and Miyagi as follows. (1) Log-grown shiitake (outdoor cultivation) produced in Ichinoseki-shi, Kamaishi-shi, Oshu-shi, Hiraizumi-cho and Otsuchi-cho, Iwate prefecture. (2) Log-grown shiitake (outdoor cultivation) produced in Tome-shi and Higashimatsushima-shi, Miyagi prefecture. 1. With regard to Iwate prefecture, the restriction of distribution of Log-grown shiitake (outdoor cultivation) produced in Ichinoseki-shi, Kamaishi-shi, Oshu-shi, Hiraizumi-cho and Otsuchi-cho is instructed today. (1) The Instruction of the Nuclear Emergency Response Headquarters is attached as attachment 1. (2) The concept of management at Iwate Prefecture after ordering the restriction of distribution is attached as attachment 2. 2. With regard to Miyagi prefecture, the restriction of distribution of Log-grown shitake (outdoor cultivation) produced in Tome-shi and Higashimatsushima-shi is instructed today. (1) The Instruction of the Nuclear Emergency Response Headquarters is attached as attachment 3. (2) The concept of management at Miyagi Prefecture after ordering the restriction of distribution is attached as attachment 4. -

Sega Sammy Holdings Inc
Review of Activities Looking back with a “Key Person” Review of Activities up to the Second Quarter Tomo, latest title in the Pachislot Hokuto No Ken series, This year’s newly released titles start strong! began operations on September 7! Keep an eye on Hortensia SAGA, Operations began on September 7, 2015 for Pa- MONSTER GEAR and Sen-no-kaizoku! chislot Hokuto No Ken Tomo, the latest title in the SEGA Games SEGA Networks Company’s product line is Pachislot Hokuto No Ken series, which recorded growing ever more plentiful, with a collection of games in the highest number of unit sales in pachislot history genres and worlds that meet the needs of diversifying player Hortensia SAGA with the launch of its first generation title in 2003. base. ©SEGA / f4samurai This machine was developed as the culmination of Released in April 2015, Hortensia SAGA surpassed 3 mil- the series with “inheritance of the classic” and lion downloads in October. This RPG is an epic tale of war, “evolution of the classic” as its concepts. In addi- in which players learn about the history woven by myriad tion to inheriting the most beloved gameplay in pa- knights at the mercy of fates in the war. chislot history from the first generation Pachislot MONSTER GEAR (released in May) also surpassed 3 mil- Hokuto No Ken, and expanding upon the game- lion downloads in August. Anyone can enjoy the authentic MONSTER GEAR play of the previous title Pachislot Hokuto No Ken hunting action immediately, with the easy controls of this ©SEGA Chapter of Resurrection, its unique housing livens new era hunting action RPG from SEGA.