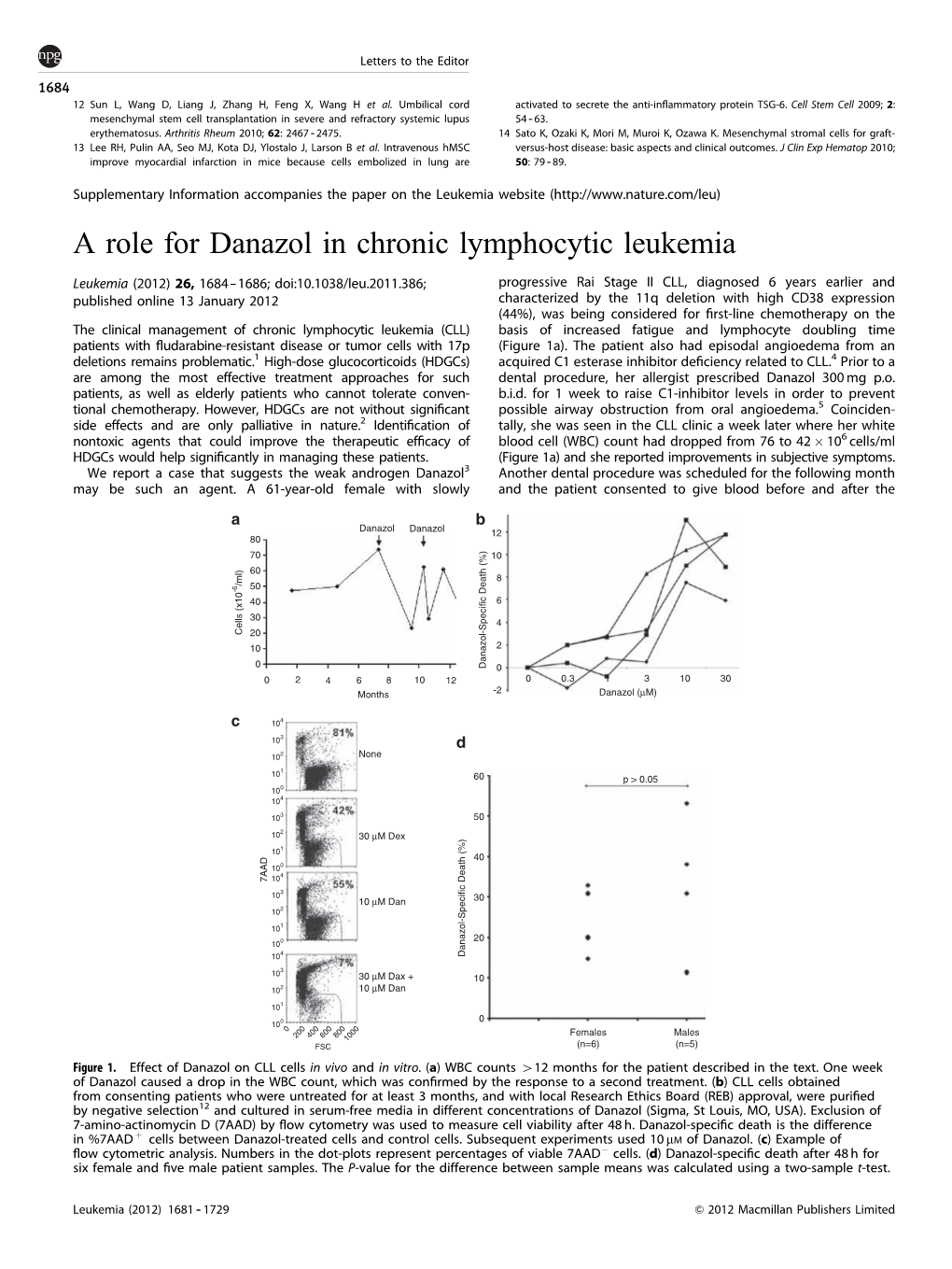
A Role for Danazol in Chronic Lymphocytic Leukemia
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Mifepristone
1. NAME OF THE MEDICINAL PRODUCT Mifegyne 200 mg tablets 2. QUALITATIVE AND QUANTITATIVE COMPOSITION Each tablet contains 200-mg mifepristone. For the full list of excipients, see section 6.1 3. PHARMACEUTICAL FORM Tablet. Light yellow, cylindrical, bi-convex tablets, with a diameter of 11 mm with “167 B” engraved on one side. 4. CLINICAL PARTICULARS For termination of pregnancy, the anti-progesterone mifepristone and the prostaglandin analogue can only be prescribed and administered in accordance with New Zealand’s abortion laws and regulations. 4.1 Therapeutic indications 1- Medical termination of developing intra-uterine pregnancy. In sequential use with a prostaglandin analogue, up to 63 days of amenorrhea (see section 4.2). 2- Softening and dilatation of the cervix uteri prior to surgical termination of pregnancy during the first trimester. 3- Preparation for the action of prostaglandin analogues in the termination of pregnancy for medical reasons (beyond the first trimester). 4- Labour induction in fetal death in utero. In patients where prostaglandin or oxytocin cannot be used. 4.2 Dose and Method of Administration Dose 1- Medical termination of developing intra-uterine pregnancy The method of administration will be as follows: • Up to 49 days of amenorrhea: 1 Mifepristone is taken as a single 600 mg (i.e. 3 tablets of 200 mg each) oral dose, followed 36 to 48 hours later, by the administration of the prostaglandin analogue: misoprostol 400 µg orally or per vaginum. • Between 50-63 days of amenorrhea Mifepristone is taken as a single 600 mg (i.e. 3 tablets of 200 mg each) oral dose, followed 36 to 48 hours later, by the administration of misoprostol. -

Areas of Future Research in Fibroid Therapy
9/18/18 Cumulative Incidence of Fibroids over Reproductive Lifespan RFTS Areas of Future Research Blacks Blacks UFS Whites in Fibroid Therapy CARDIA Age 33-46 William H. Catherino, MD, PhD Whites Professor and Chair, Research Division Seveso Italy Uniformed Services University Blacks Whites Associate Program Director Sweden/Whites (Age 33-40) Division of REI, PRAE, NICHD, NIH The views expressed in this article are those of the author(s) and do not reflect the official policy or position of the Department of the Army, Department of Defense, or the US Government. Laughlin Seminars Reprod Med 2010;28: 214 Fibroids Increase Miscarriage Rate Obstetric Complications of Fibroids Complication Fibroid No Fibroid OR Abnormal labor 49.6% 22.6% 2.2 Cesarean Section 46.2% 23.5% 2.0 Preterm delivery 13.8% 10.7% 1.5 BreecH position 9.3% 4.0% 1.6 pp Hemorrhage 8.3% 2.9% 2.2 PROM 4.2% 2.5% 1.5 Placenta previa 1.7% 0.7% 2.0 Abruption 1.4% 0.7% 2.3 Guben Reprod Biol Odds of miscarriage decreased with no myoma comparedEndocrinol to myoma 2013;11:102 Biderman-Madar ArcH Gynecol Obstet 2005;272:218 Ciavattini J Matern Fetal Neonatal Med 2015;28:484-8 Not Impacting the Cavity Coronado Obstet Gynecol 2000;95:764 Kramer Am J Obstet Gynecol 2013;209:449.e1-7 Navid Ayub Med Coll Abbottabad 2012;24:90 Sheiner J Reprod Med 2004;49:182 OR = 0.737 [0.647, 0.840] Stout Obstet Gynecol 2010;116:1056 Qidwai Obstet Gynecol 2006;107:376 1 9/18/18 Best Studied Therapies Hysterectomy Option over Time Surgical Radiologic Medical >100 years of study Hysterectomy Open myomectomy GnRH agonists 25-34 years of study Endometrial Ablation GnRH agonists 20-24 years of study Laparoscopic myomectomy Uterine artery embolization Retinoic acid 10-19 years of study Uterine artery obstruction SPRMs: Mifepristone, ulipristal Robotic myomectomy GnRH antagonists 5-9 years of study Cryomyolysis MRI-guided high frequency ultrasound SPRMs: Asoprisnil, Telapristone, Laparoscopic ablation Vilaprisan SERMs: Tamoxifen, Raloxifene, Letrozole, Genistein Pitter MC, Simmonds C, Seshadri-Kreaden U, Hubert HB. -

Anabolic Steroids/Androgens Pa Summary
ANABOLIC STEROIDS/ANDROGENS PA SUMMARY PREFERRED Anadrol-50, Danazol, Fluoxymesterone, Methitest, Oxandrolone, Testosterone Cypionate Injection, Testosterone Enanthate Injection NON-PREFERRED Android, Testred LENGTH OF AUTHORIZATION: Varies NOTE: All preferred and non-preferred agents require prior authorization. See PA criteria labeled “Topical Testosterone” for Androderm, Androgel, Striant, and Testim. The criteria details below are for the outpatient pharmacy program. If an injectable medication is being administered in a physician’s office then the criteria information below does not apply. Instead, the physician’s office must bill this drug through the DCH physician’s injectable program and not the outpatient pharmacy program. Information regarding the physician’s injectable program can be located at www.mmis.georgia.gov. PA CRITERIA: For Anadrol-50 Approvable for the following diagnoses: anemia caused by deficient red blood cell production, acquired or congenital aplastic anemia, myelofibrosis, hypoplastic anemia due to administration of myelotoxic drugs Also approvable for HIV or AIDS wasting when significant weight loss is documented in members currently receiving nutritional support For Danazol Approvable for the following diagnoses: endometriosis, fibrocystic breast disease, hereditary angioedema For Fluoxymesterone, Methyltestosterone (Android, Methitest, Testred), Testosterone Cypionate or Enanthate Injection Approvable in male members 12 years of age or older for the following diagnoses: primary hypogonadism, secondary -

Ep 2446888 A2
(19) & (11) EP 2 446 888 A2 (12) EUROPEAN PATENT APPLICATION (43) Date of publication: (51) Int Cl.: 02.05.2012 Bulletin 2012/18 A61K 31/569 (2006.01) (21) Application number: 11010272.0 (22) Date of filing: 12.07.2006 (84) Designated Contracting States: (71) Applicant: DMI Biosciences, Inc. AT BE BG CH CY CZ DE DK EE ES FI FR GB GR Englewood, CO 80110-3948 (US) HU IE IS IT LI LT LU LV MC NL PL PT RO SE SI SK TR (72) Inventor: Bar-Or, David Designated Extension States: Englewood, Colorado 80110 (US) AL BA HR MK RS (74) Representative: Schaeberle, Steffen (30) Priority: 12.07.2005 US 69872305 P Hoefer & Partner 24.08.2005 US 71115705 P Patentanwälte 24.08.2005 US 71115805 P Pilgersheimer Strasse 20 81543 München (DE) (62) Document number(s) of the earlier application(s) in accordance with Art. 76 EPC: Remarks: 06787393.5 / 1 919 290 This application was filed on 29-12-2011 as a divisional application to the application mentioned under INID code 62. (54) Use of danazol for the treatment of uveitis (57) The present invention relates to the treatment of an inflammatory disease or condition of the eye such as uveitis with danazof or a pharmacologically-acceptable salt or ester thereof. EP 2 446 888 A2 Printed by Jouve, 75001 PARIS (FR) EP 2 446 888 A2 Description FIELD OF THE INVENTION 5 [0001] The present invention relates to the treatment of diseases and conditions with an effective amount of a steroid having those formulas given below, or a pharmacologically-acceptable salt or ester thereof. -

Hirsutism and Polycystic Ovary Syndrome (PCOS)
Hirsutism and Polycystic Ovary Syndrome (PCOS) A Guide for Patients PATIENT INFORMATION SERIES Published by the American Society for Reproductive Medicine under the direction of the Patient Education Committee and the Publications Committee. No portion herein may be reproduced in any form without written permission. This booklet is in no way intended to replace, dictate or fully define evaluation and treatment by a qualified physician. It is intended solely as an aid for patients seeking general information on issues in reproductive medicine. Copyright © 2016 by the American Society for Reproductive Medicine AMERICAN SOCIETY FOR REPRODUCTIVE MEDICINE Hirsutism and Polycystic Ovary Syndrome (PCOS) A Guide for Patients Revised 2016 A glossary of italicized words is located at the end of this booklet. INTRODUCTION Hirsutism is the excessive growth of facial or body hair on women. Hirsutism can be seen as coarse, dark hair that may appear on the face, chest, abdomen, back, upper arms, or upper legs. Hirsutism is a symptom of medical disorders associated with the hormones called androgens. Polycystic ovary syndrome (PCOS), in which the ovaries produce excessive amounts of androgens, is the most common cause of hirsutism and may affect up to 10% of women. Hirsutism is very common and often improves with medical management. Prompt medical attention is important because delaying treatment makes the treatment more difficult and may have long-term health consequences. OVERVIEW OF NORMAL HAIR GROWTH Understanding the process of normal hair growth will help you understand hirsutism. Each hair grows from a follicle deep in your skin. As long as these follicles are not completely destroyed, hair will continue to grow even if the shaft, which is the part of the hair that appears above the skin, is plucked or removed. -

Antiprogestins, a New Form of Endocrine Therapy for Human Breast Cancer1
[CANCER RESEARCH 49, 2851-2856, June 1, 1989] Antiprogestins, a New Form of Endocrine Therapy for Human Breast Cancer1 Jan G. M. Klijn,2Frank H. de Jong, Ger H. Bakker, Steven W. J. Lamberts, Cees J. Rodenburg, and Jana Alexieva-Figusch Department of Medical Oncology (Division of Endocrine Oncology) [J. G. M. K., G. H. B., C. J. K., J. A-F.J, Dr. Daniel den Hoed Cancer Center, and Department of Endocrinology ¡F.H. d. J., S. W. ]. L.J, Erasmus University, Rotterdam, The Netherlands ABSTRACT especially pronounced effects on the endometrium, decidua, ovaries, and hypothalamo-pituitary-adrenal axis. With regard The antitumor, endocrine, hematological, biochemical, and side effects of chronic second-line treatment with the antiprogestin mifepristone (RU to clinical practice, the drug has currently been used as a contraceptive agent or abortifacient as a result of its antipro 486) were investigated in 11 postmenopausal patients with metastatic breast cancer. We observed one objective response, 6 instances of short- gestational properties (2, 22-24). Based on its antiglucocorti term stable disease, and 4 instances of progressive disease. Mean plasma coid properties, this drug has been used or has been proposed concentrations of adrenocorticotropic hormone (/' < 0.05), cortisol (/' < for treatment of conditions related to excess corticosteroid 0.001), androstenedione (/' < 0.01), and estradici (P < 0.002) increased production such as Cushing's syndrome (19, 25-27) and for significantly during treatment accompanied by a slight decrease of sex treatment of lymphomas (24) and glaucoma (28); because of its hormone binding globulin levels, while basal and stimulated gonadotropi effects on the immune system, the drug has been suggested to levels did not change significantly. -

Guidance on Bioequivalence Studies for Reproductive Health Medicines
Medicines Guidance Document 23 October 2019 Guidance on Bioequivalence Studies for Reproductive Health Medicines CONTENTS 1. Introduction........................................................................................................................................................... 2 2. Which products require a bioequivalence study? ................................................................................................ 3 3. Design and conduct of bioequivalence studies .................................................................................................... 4 3.1 Basic principles in the demonstration of bioequivalence ............................................................................... 4 3.2 Good clinical practice ..................................................................................................................................... 4 3.3 Contract research organizations .................................................................................................................... 5 3.4 Study design .................................................................................................................................................. 5 3.5 Comparator product ....................................................................................................................................... 6 3.6 Generic product .............................................................................................................................................. 6 3.7 Study subjects -

Mifepristone (Korlym)
Drug and Biologic Coverage Policy Effective Date ............................................ 1/1/2021 Next Review Date… ..................................... 1/1/2022 Coverage Policy Number ............................... IP0092 Mifepristone (Korlym®) Table of Contents Related Coverage Resources Overview .............................................................. 1 Coverage Policy ................................................... 1 Reauthorization Criteria ....................................... 2 Authorization Duration ......................................... 2 Conditions Not Covered....................................... 2 Background .......................................................... 3 References .......................................................... 4 INSTRUCTIONS FOR USE The following Coverage Policy applies to health benefit plans administered by Cigna Companies. Certain Cigna Companies and/or lines of business only provide utilization review services to clients and do not make coverage determinations. References to standard benefit plan language and coverage determinations do not apply to those clients. Coverage Policies are intended to provide guidance in interpreting certain standard benefit plans administered by Cigna Companies. Please note, the terms of a customer’s particular benefit plan document [Group Service Agreement, Evidence of Coverage, Certificate of Coverage, Summary Plan Description (SPD) or similar plan document] may differ significantly from the standard benefit plans upon which these Coverage -

The Clinical Efficacy of Progesterone Antagonists in Breast Cancer ------ .__..__
8 The clinical efficacy of progesterone antagonists in breast cancer --------_.__..__. Walter Jonat, Marius Giurescu, John FR Robertson CONTENTS • Introduction • Onapristone • Mlfepristone • Summary INTRODUCTION indication of a functional PgR.4 As described in Chapter 14, substantial in vitro and in vivo The search for active and safe alternatives to evidence suggests that PgR serves as a biologi current systemic therapies is one of the main cally important molecule in breast cancer objectives of current breast cancer research. behaviour. Moreover, preclinical studies indi Over the last three decades since the discovery cate that blockade of PgR function inhibits pro of the estrogen receptor (ER), the development liferation and induces apoptosis (see Chapter of new endocrine agents has in the main been 14). Therefore, clinically practical PgR inhibitors aimed at either preventing the production of have been developed. These are overtly active estrogens (e.g. ovarian ablation with small molecuk'S that appear to function by gonadotropin-releasing hormone (GnRH) ana binding to PgR and inhibiting pathways down logues, aromatase inhibition) or blocking their stream of PgR. Two agents, onapristone and effect by competition for ER (e.g. selective ER mifepristone, have been evaluated in clinical modulators (SERMs) and pure antiestrogens). trials, and, as described below, have activity in Such developments have focused, indirectly or patients with metastatic disease. Although com directly, on the ER as a target for manipulation mercial support for these two agents has of tumour growth. This approach is supported recently waned, the concept of PgR inhibition by the finding that the response to such thera in breast cancer is sufficiently well founded to pies is related to the expression of ER by breast justify its inclusion in any textbook of endocrine tumours.13 However, it is also known that therapy. -

WO 2013/163758 Al 7 November 2013 (07.11.2013) P O P C T
(12) INTERNATIONAL APPLICATION PUBLISHED UNDER THE PATENT COOPERATION TREATY (PCT) (19) World Intellectual Property Organization I International Bureau (10) International Publication Number (43) International Publication Date WO 2013/163758 Al 7 November 2013 (07.11.2013) P O P C T (51) International Patent Classification: (72) Inventor; and A61K 31/416 (2006.01) C12Q 1/00 (2006.01) (71) Applicant : BOYD, Shelley Romayne [CA/CA]; Unit A61P 27/02 (2006.01) A61B 3/10 (2006.01) 2106, 112 George Street, Toronto, Ontario M5A 2M5 (CA). (21) International Application Number: PCT/CA2013/050335 (74) Agents: MARLES, Jennifer A. et al; 480-601 West Cor dova Street, Vancouver, British Columbia V6B 1G1 (CA). (22) International Filing Date: 30 April 2013 (30.04.2013) (81) Designated States (unless otherwise indicated, for every kind of national protection available): AE, AG, AL, AM, (25) Filing Language: English AO, AT, AU, AZ, BA, BB, BG, BH, BN, BR, BW, BY, (26) Publication Language: English BZ, CA, CH, CL, CN, CO, CR, CU, CZ, DE, DK, DM, DO, DZ, EC, EE, EG, ES, FI, GB, GD, GE, GH, GM, GT, (30) Priority Data: HN, HR, HU, ID, IL, IN, IS, JP, KE, KG, KM, KN, KP, 61/640,854 1 May 2012 (01.05.2012) US KR, KZ, LA, LC, LK, LR, LS, LT, LU, LY, MA, MD, 61/641,393 2 May 2012 (02.05.2012) US ME, MG, MK, MN, MW, MX, MY, MZ, NA, NG, NI, 61/693,226 24 August 2012 (24.08.2012) us NO, NZ, OM, PA, PE, PG, PH, PL, PT, QA, RO, RS, RU, 61/792,436 15 March 2013 (15.03.2013) us RW, SC, SD, SE, SG, SK, SL, SM, ST, SV, SY, TH, TJ, TM, TN, TR, TT, TZ, UA, UG, US, UZ, VC, VN, ZA, ZM, ZW. -

Endometriosis
CLINICAL REVIEW Endometriosis Follow the link from the online version of this article to obtain certi ed continuing 1 2 3 medical education credits Martha Hickey, Karen Ballard, Cindy Farquhar 1 Endometriosis is a relatively common and potentially Department of Obstetrics and SOURCES AND SELECTION CRITERIA Gynaecology, University of debilitating condition affecting women of reproductive We searched Medline and Pubmed, used personal archives Melbourne and the Royal Women’s age. Prevalence is difficult to determine, firstly because of Hospital, Melbourne, Victoria, of references, and consulted with other experts to inform Australia 3052 variability in clinical presentation, and, secondly because this manuscript. When available, data from systematic 2Faculty of Health and Medical the only reliable diagnostic test is laparoscopy, when endo- reviews and randomised controlled trials were used. We Sciences, University of Surrey, metriotic deposits can be visualised and histologically also used expert guidelines such as the recent European Guildford, Surrey, UK Society of Human Reproduction and Embryology (ESHRE) 3 confirmed. Population based studies report a prevalence Department of Obstetrics and consensus.4 Gynaecology, University of of around 1.5% compared with 6-15% in hospital based 1 Auckland, Auckland, New Zealand studies. Endometriosis can be asymptomatic, but those Correspondence to: M Hickey with symptoms generally present early in reproductive What are the causes of endometriosis? [email protected] life and improve after menopause. Symptomatic endome- The pathogenesis of endometriosis is unknown, but lead- Cite this as: BMJ 2104;348:g1752 triosis can result in long term adverse effects on personal ing theories include retrograde menstruation, altered doi: 10.1136/bmj.g1752 relationships, quality of life, and work productivity. -

Mifepristone in the Central Nucleus of the Amygdala Reduces Yohimbine Stress-Induced Reinstatement of Ethanol-Seeking
Neuropsychopharmacology (2012) 37, 906–918 & 2012 American College of Neuropsychopharmacology. All rights reserved 0893-133X/12 www.neuropsychopharmacology.org Mifepristone in the Central Nucleus of the Amygdala Reduces Yohimbine Stress-Induced Reinstatement of Ethanol-Seeking 1 1,2 1 1 ,1 Jeffrey A Simms , Carolina L Haass-Koffler , Jade Bito-Onon , Rui Li and Selena E Bartlett* 1 Preclinical Development Group, Ernest Gallo Clinic and Research Center at University of California San Francisco, Emeryville, CA, USA; 2 Clinical Pharmacology and Experimental Therapeutics, University of California San Francisco, Byers Hall, San Francisco, CA, USA Chronic ethanol exposure leads to dysregulation of the hypothalamic-pituitary-adrenal axis, leading to changes in glucocorticoid release and function that have been proposed to maintain pathological alcohol consumption and increase vulnerability to relapse during abstinence. The objective of this study was to determine whether mifepristone, a glucocorticoid receptor antagonist, plays a role in ethanol self-administration and reinstatement. Male, Long–Evans rats were trained to self-administer either ethanol or sucrose in daily 30 min operant self-administration sessions using a fixed ratio 3 schedule of reinforcement. Following establishment of stable baseline responding, we examined the effects of mifepristone on maintained responding and yohimbine-induced increases in responding for ethanol and sucrose. Lever responding was extinguished in separate groups of rats and animals were tested for yohimbine-induced reinstatement and corticosterone release. We also investigated the effects of local mifepristone infusions into the central amygdala (CeA) on yohimbine-induced reinstatement of ethanol- and sucrose-seeking. In addition, we infused mifepristone into the basolateral amygdala (BLA) in ethanol-seeking animals as an anatomical control.