Accessibility Standards Activities
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Orthotics Fact Sheet
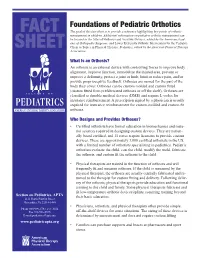
Foundations of Pediatric Orthotics FACT The goal of this fact sheet is to provide a reference highlighting key points of orthotic management in children. Additional information on pediatric orthotic management can be located in the Atlas of Orthoses and Assistive Devices, edited by the American Acad- emy of Orthopedic Surgeons, and Lower Extremity Orthotic Intervention for the Pediatric SHEET Client in Topics in Physical Therapy: Pediatrics, edited by the American Physical Therapy Association. What Is an Orthosis? An orthosis is an external device with controlling forces to improve body alignment, improve function, immobilize the injured area, prevent or improve a deformity, protect a joint or limb, limit or reduce pain, and/or provide proprioceptive feedback. Orthoses are named for the part of the body they cover. Orthoses can be custom molded and custom fitted (custom fitted from prefabricated orthoses or off the shelf). Orthoses are classified as durable medical devices (DME) and require L-codes for insurance reimbursement. A prescription signed by a physician is usually required for insurance reimbursement for custom-molded and custom-fit orthoses. Who Designs and Provides Orthoses? • Certified orthotists have formal education in biomechanics and mate- rial sciences required in designing custom devices. They are nation- ally board certified, and 11 states require licensure to provide custom devices. There are approximately 3,000 certified orthotists in the US, with a limited number of orthotists specializing in pediatrics. Pediatric orthotists evaluate the child, cast the child, modify the mold, fabricate the orthosis, and custom fit the orthosis to the child. • Physical therapists are trained in the function of orthoses and will frequently fit and measure orthoses. -

Lower Extremity Orthoses in Children with Spastic Quadriplegic Cerebral Palsy Implications for Nurses, Parents, and Caregivers
NOR200210.qxd 5/5/11 5:53 PM Page 155 Lower Extremity Orthoses in Children With Spastic Quadriplegic Cerebral Palsy Implications for Nurses, Parents, and Caregivers Kathleen Cervasio Understanding trends in the prevalence of children with cerebral prevalence for cerebral palsy in the United States is palsy is vital to evaluating and estimating supportive services for 2.4 per 1,000 children, an increase over previously re- children, families, and caregivers. The majority of children with ported data (Hirtz, Thurman, Gwinn-Hardy, Mohammad, cerebral palsy require lower extremity orthoses to stabilize their Chaudhuri, & Zalusky, 2007). Cerebral palsy is primar- muscles. The pediatric nurse needs a special body of knowledge ily a disorder of movement and posture originating in to accurately assess, apply, manage, teach, and evaluate the use the central nervous system with an incidence of 2.5 per 1,000 live births with spastic quadriplegia being the of lower extremity orthoses typically prescribed for this vulnera- common type of cerebral palsy (Blair & Watson, 2006). ble population. Inherent in caring for these children is the need This nonprogressive neurological disorder is defined as to teach the child, the family, and significant others the proper a variation in movement, coordination, posture, and application and care of the orthoses used in hospital and com- gait resulting from brain injury around birth (Blair & munity settings. Nursing literature review does not provide a Watson, 2006). Numerous associated comorbidities are basis for evidence in designing and teaching orthopaedic care usually present with cerebral palsy requiring various for children with orthoses. A protocol for orthoses management interventions. -
A Year of Progress “Every Day You May Make Progress
2007 Annual Report of the Amputee Coalition of America A Year of Progress “Every day you may make progress. Every step may be fruitful. Yet there will stretch out before you an ever- lengthening, ever-ascending, ever-improving path. You know you will never get to the end of the journey. But this, so far from discouraging, only adds to the joy and glory of the climb.” — Sir Winston Churchill 1 our mission To reach out to people with limb loss and to empower them through education, support and advocacy. In Support of Our Mission Advocacy Education ACA advocates for the rights of people with limb ACA publishes inMotion, First Step and other magazines loss or a limb difference. This includes access to, and that comprehensively address areas of interest and delivery of, information, quality care, appropriate concern to amputees and those who care for and about devices, reimbursement, and the services required to them. lead empowered lives. ACA develops and distributes educational resources, ACA promotes full implementation of the Americans booklets, videotapes, and fact sheets to enhance the with Disabilities Act and other legislation that guaran- knowledge and coping skills of people affected by am- tees full participation in society for all people, regard- putation or congenital limb differences. less of disability. ACA’s National Limb Loss Information Center is a com- ACA sensitizes professionals, the general public and prehensive source of information about amputation policymakers to the issues, needs and concerns of and rehabilitation. amputees. ACA provides technical help, resources and training for Support local amputee educational and support organizations. -

Orthotics Catalog Custom Fit and Off-The-Shelf Products in 1919 Otto Bock Had a Vision for Helping People Be More Mobile and Independent
Orthotics Catalog Custom fit and off-the-shelf products In 1919 Otto Bock had a vision for helping people be more mobile and independent. His vision sparked the foundation of a century old company that still bears his name. Nearly 100 years later, Ottobock has locations in more than 149 countries, serving thousands of clinicians and patients with unique prosthetic, orthotic, and mobility devices. In North America, we have partnered with the O&P community since 1958. We regularly lobby for legislation that supports the O&P industry and the patients you care for. And we develop products that keep you on the cutting edge of orthotics. Today we are applying our advanced technology to orthotics to help stabilize injuries, provide post-operative support, and to help people to walk again. Our orthotic innovations will help place you on the cutting edge of orthotic solutions. To order any of our products or services, contact your local sales representative or Ottobock directly. United States 800 328 4058 [email protected] professionals.ottobockUS.com Canada 800 665 3327 [email protected] professionals.ottobock.ca Contents Knee . 5 Ligament Braces . 6 Patellofemoral Braces and Supports . 21 Post-Operative Braces . 25 Spine . 31 Thoracolumbar Sacral Orthoses (TLSOs) . 32 Hyperextension Orthoses . 34 Lumbar Sacral Orthoses (LSOs) . 40 Lumbar Orthoses . 54 Spinal Corsets . 63 Sacroiliac Supports . 66 Cervical . 69 Cervical Thoracic Orthoses . 70 Cervical Orthoses . 73 Foot and Ankle . 79 Ankle Braces and Supports . 80 Walker Boots . 84 Plantar Fasciitis Supports . 94 Shoulder . 101 Shoulder Immobilizers . 102 Shoulder Stabilizers . 105 Upper Extremity . 109 Elbow Supports . 110 Wrist, Hand Braces and Supports . -

Making a Makerspace? Guidelines for Accessibility and Universal Design
Making a Makerspace? Guidelines for Accessibility and Universal Design Many engineering departments, libraries, and Student Voices universities are launching new initiatives to create Why are accessible makerspaces important, makerspaces, physical spaces where students, and how do we involve more students with faculty, and the broader community can gather disabilities? and share resources and knowledge, work on projects, network, and build. In creating these • “Makerspaces are about community. innovative spaces we should apply principles of We need to ensure everyone from the universal design to ensure the spaces, tools, and community can participate.” community are accessible to as many individuals as possible. • “Makerspaces are often used to help build new assistive technology and increase Universal design encourages the design of space, accessibility; however, many of these spaces products, and processes not just for the average and tools remain inaccessible. We need to user, but for people with a broad range of abilities, make sure disabled people can access these ages, reading levels, learning styles, languages, spaces and create the products and designs cultures, and other characteristics. Makerspaces that they actually want.” foster innovation, and we want to ensure that individuals of all backgrounds and abilities can actively contribute to the design process. We Planning and Policies advocate for participatory design (interactions. Create a culture of inclusion and universal design acm.org/archive/view/march-april-2015/design-for- as early as possible. During your planning process user-empowerment) where individuals from diverse consider the following questions: backgrounds bring their unique experiences and • Are people with a variety of disabilities in- perspectives to the design process. -

Assistive Technology That's Free
AT That’s Free By Andrew Leibs Before the digital age, assistive technology was hard to miss, and hard to buy. Classmates would see a sight-impaired student’s boxy video magnifier or hear her computer talk. These were costly, clunky solutions usually acquired through special education. Today, we have the inverse: sleek laptops, tablets, and smartphones now have so much processing power, manufacturers can enfold functionality – e.g., screen reading, magnification, audio playback – that once necessitated separate software or machines. All Windows and iOS devices have more built-in accessibility than most users will ever need or know they have. And what’s not built into the operating system is usually available as a free mobile app, web service, or downloadable application. Here’s a quick look at some of the assistive applications you either have or can quickly snag to make reading, writing, online research, and information sharing more accessible or efficient. Accessibility Built Into Microsoft Windows & Office The Microsoft Windows operating system provides three main accessibility applications: Narrator, a screen reader; Magnifier, a text and image enlarger; and On-Screen Keyboard, an input option for persons who are unable to type on a standard keyboard. The programs are located in the system’s Ease of Access Center. To get there, click Start, Control Panel, and then Ease of Access Center. The Center lets you change accessibility settings, activate built-in command tools, and fill out a questionnaire to receive personalized recommendations. • Narrator is a screen reader that lets users operate their PC without a display. Narrator reads all onscreen text aloud, provides verbal cues to navigate programs, and has keyboard shortcuts for choosing what's read, e.g., “Insert + F8” will read the current document. -

Foot Orthotics Page 1 of 6
Version 5.0 Johns Hopkins HealthCare LLC Policy Number CMS15.04 Medical Policy Effective Date 05/01/2020 Medical Policy Review Date 02/18/2020 Subject Revision Date 02/18/2020 Foot Orthotics Page 1 of 6 Keywords: Foot Orthotics, Orthotics Table of Contents Page Number I. ACTION 1 II. POLICY DISCLAIMER 1 III. POLICY 1 IV. POLICY CRITERION 2 V. BACKGROUND 3 VI. CODING DISCLAIMER 4 VII. CODING INFORMATION 4 VIII. REFERENCE STATEMENT 5 IX. REFERENCES 5 X. APPROVALS 6 I. ACTION New Policy X Revising Policy Number CMS15.04 Superseding Policy Number Archiving Policy Number Retiring Policy Number II. POLICY DISCLAIMER Johns Hopkins HealthCare LLC (JHHC) provides a full spectrum of health care products and services for Employer Health Programs, Priority Partners, Advantage MD, and US Family Health Plan. Each line of business possesses its own unique contract and guidelines which, for benefit and payment purposes, should be consulted first to know what benefits are available for coverage. Specific contract benefits, guidelines or policies supersede the information outlined in this policy. III. POLICY For Advantage MD, refer to: Medicare Coverage Database: • Local Coverage Determination (LCD) L33641 Orthopedic Footwear • Local Coverage Article A52481 Orthopedic Footwear • Local Coverage Determination (LCD) L33369 Therapeutic Shoes for Persons with Diabetes • Local Coverage Article A52501 Therapeutic Shoes for Persons with Diabetes For Employer Health Programs (EHP) refer to: • Plan specific Summary Plan Descriptions (SPD's) For Priority Partners -

Rehabilitation of People with Physical Disabilities in Developing Countries
Rehabilitation of people with physical disabilities in developing countries Program Report for Collaborative Agreement: DFD-A-00-08-00309-00 September 30, 2008 – December 31, 2015 Author: Sandra Sexton March 2016 ISPO Registered Office: International Society for Prosthetics and Orthotics (ISPO) c/o ICAS ApS Trekronervej 28 Strøby Ergede 4600 Køge Denmark Correspondence: International Society for Prosthetics and Orthotics 22-24 Rue du Luxembourg BE-1000 Brussels, Belgium Telephone: +32 2 213 13 79 Fax: +32 2 213 13 13 E-mail: [email protected] Website: www.ispoint.org ISBN 978-87-93486-00-3 1 Contents Page 1. Executive summary 3 2. List of acronyms 4 3. Acknowledgements 5 4. Introduction and background 6 4.1 Prosthetics and orthotics in developing countries 6 4.2 The prosthetics and orthotics workforce 6 5. Program activities, progress and results 7 5.1 Scholarships 7 5.2 Measuring the impact of training in prosthetics and orthotics 13 5.3 Enhancement of prosthetics and orthotics service provision 18 6. Budget and expenditure 22 7. References 23 2 1. Executive Summary Prosthetics and orthotics services enable people with physical impairments of their limbs or spine the opportunity to achieve greater independence to participate in society. Alarmingly, such services are not available to an estimated 9 out of 10 people with disabilities globally due to a shortage of personnel, service units and health rehabilitation infrastructures1. To try and address this situation, our International Society for Prosthetics and Orthotics (ISPO) members have been working towards development of the prosthetics and orthotics sector since our Society’s inception in the 1970s. -
SCOPE of PRACTICE ABC Scope of Practice Committee
Orthotic Prosthetic & Pedorthic SCOPE OF PRACTICE ABC Scope of Practice Committee Rick G. Parr, CPO, FAAOP, Chairman Michael J. Allen, CPO, FAAOP Chelsey B. Anderson, CPO, FAAOP Jennifer A. Bick, CO Stephen B. Fletcher, CPO Erin O’Brien, CPO, FAAOP Michael S. Rees, C.Ped., CFo John H. Reynolds, CPO, FAAOP Heather E. Swiggum, CP Steven R. Whiteside, CO, FAAOP Catherine A. Carter, ABC Executive Director 330 John Carlyle Street, Suite 210 Alexandria, VA 22314 703-836-7114 ABCop.org Effective January 2019 This edition supersedes all previous editions. All rights reserved. No part of this document may be produced in any form without written permission of the ©2019 by the American Board for Certification in Orthotics, Prosthetics & Pedorthics, Inc. American Board for Certification in Orthotics, Prosthetics & Pedorthics, Inc. Table of Contents Forward ......................................................................................................................................1 ABC Credentials .......................................................................................................................2 Delineation of Scopes of Practice ABC Certified Orthotist/Prosthetist ................................................................................3 ABC Certified Pedorthist...................................................................................................6 ABC Certified Fitter-Orthotics .........................................................................................9 ABC Certified Fitter-Therapeutic -

Newsletter 2014 Spring
Access to Independence of Cortland County, Inc. Nothing More, Nothing Less For All People ACCESS NEWS With Disabilities Spring 2014 NUMBER XXXX ATI Recognizes Volunteers ATI Celebrates Founding Day ATI Awarded Grants On April 10, ATI recognized the On May 8, ATI recognized its Over the last several months, contributions of its volunteers by 16th anniversary as a nonprofit cor- ATI has been awarded a number of hosting them to pizza, wings and poration by hosting 50 former and small grants from area foundations salad. ATI also presented special current Board Members to a cele- in support of specific program and awards of appreciation to two indi- bration luncheon. operations initiatives. viduals who went above and be- On May 8, 1998, founding Board On February 19, ATI received yond over the past six months: Sara Members included: Thomas Miller, $2,000 from the Ralph R. Wilkins Askew and Rene Waddy. Lorriane Janke and Christopher Far- Foundation towards the cost of in- Over the past six months, 45 kas. Frances Pizzola was the found- stalling a new network server and individuals have volunteered their ing volunteer Director. At the time productivity software for consumer time at ATI for a total of 1,156 ATI was housed in Room 200 of the and staff computers. hours. Volunteers donated their County Office Building. On March 31, ATI received time in various ways, including: ATI’s roots go back to the 1980’s $2,000 from the Triad Foundation providing clerical support, partici- when it was known as the Cortland to provide support for ATI’s 2014 pating in advocacy efforts, partici- County Accessibility Committee Disability Employment Awareness pating on the Board of Directors, (CCAC). -

Disability Rights Movement —The ADA Today
COVER STORY: ADA Today The Disability Rights Movement —The ADA Today Karen Knabel Jackson navigates Washington DC’s Metro. by Katherine Shaw ADA legislation brought f you’re over 30, you probably amazing changes to the landscape—expected, understood, remember a time in the and fostering independence, access not-too-distant past when a nation, but more needs and self-suffi ciency for people curb cut was unusual, there to be done to level the with a wide range of disabilities. were no beeping sounds at playing fi elds for citizens Icrosswalks on busy city street with disabilities. Yet, with all of these advances, corners, no Braille at ATM court decisions and inconsistent machines, no handicapped- policies have eroded the inten- accessible bathroom stalls at the airport, few if tion of the ADA, lessening protections for people any ramps anywhere, and automatic doors were with disabilities. As a result, the ADA Restoration common only in grocery stores. Act of 2007 (H.R. 3195/S. 1881) was introduced last year to restore and clarify the original intent Today, thanks in large part to the Americans with of the legislation. Hearings have been held in both Disabilities Act (ADA), which was signed into law the House and Senate and the bill is expected to in 1990, these things are part of our architectural pass in 2008. 20 Momentum • Fall.2008 Here’s how the ADA works or doesn’t work for some people with MS today. Creating a A no-win situation Pat had a successful career as a nursing home admin- istrator in the Chicago area. -

ARTICLE Crip Technoscience Manifesto
ARTICLE Crip Technoscience Manifesto Aimi Hamraie Vanderbilt University [email protected] Kelly Fritsch Carleton University [email protected] Abstract As disabled people engaged in disability community, activism, and scholarship, our collective experiences and histories have taught us that we are effective agents of world-building and -dismantling toward more socially just relations. The grounds for social justice and world-remaking, however, are frictioned; technologies, architectures, and infrastructures are often designed and implemented without committing to disability as a difference that matters. This manifesto calls attention to the powerful, messy, non-innocent, contradictory, and nevertheless crucial work of what we name as “crip technoscience,” practices of critique, alteration, and reinvention of our material-discursive world. Disabled people are experts and designers of everyday life. But we also harness technoscience for political action, refusing to comply with demands to cure, fix, or eliminate disability. Attentive to the intersectional workings of power and privilege, we agitate against independence and productivity as requirements for existence. Instead, we center technoscientific activism and critical design practices that foster disability justice. Hamraie, A., & Fritsch, K. (2019). Crip technoscience manifesto. Catalyst: Feminism, Theory, Technoscience, 5(1), 1-34. http://www.catalystjournal.org | ISSN: 2380-3312 © Aimi Hamraie and Kelly Fritsch, 2019 | Licensed to the Catalyst Project under a Creative Commons Attribution Non-Commercial No Derivatives license Hamraie and Fritsch Catalyst: Feminism, Theory, Technoscience 5(1) 2 Introduction As disabled people engaged in disability community, activism, and scholarship, our collective experiences and histories have taught us that we are effective agents of world-building and -dismantling toward more socially just relations.