Branching Pattern Variations of the Celiac Trunk And
Total Page:16
File Type:pdf, Size:1020Kb

Load more
Recommended publications
-

Gross Anatomical Studies on the Arterial Supply of the Intestinal Tract of the Goat
IOSR Journal of Agriculture and Veterinary Science (IOSR-JAVS) e-ISSN: 2319-2380, p-ISSN: 2319-2372. Volume 10, Issue 1 Ver. I (January. 2017), PP 46-53 www.iosrjournals.org Gross Anatomical Studies on the Arterial Supply of the Intestinal Tract of the Goat Reda Mohamed1, 2*, ZeinAdam2 and Mohamed Gad2 1Department of Basic Veterinary Sciences, School of Veterinary Medicine, Faculty of Medical Sciences, University of the West Indies, Trinidad and Tobago. 2Anatomy and Embryology Department, Faculty of Veterinary Medicine, Beni Suef University Egypt. Abstract: The main purpose of this study was to convey a more precise explanation of the arterial supply of the intestinal tract of the goat. Fifteen adult healthy goats were used. Immediately after slaughtering of the goat, the thoracic part of the aorta (just prior to its passage through the hiatus aorticus of the diaphragm) was injected with gum milk latex (colored red) with carmine. The results showed that the duodenum was supplied by the cranial pancreaticoduodenal and caudal duodenal arteries. The jejunum was supplied by the jejunal arteries. The ileum was supplied by the ileal; mesenteric ileal and antimesenteric ileal arteries. The cecum was supplied by the cecal artery. The ascending colon was supplied by the colic branches and right colic arteries. The transverse colon was supplied by the middle colic artery. The descending colon was supplied by the middle and left colic arteries. The sigmoid colon was supplied by the sigmoid arteries. The rectum was supplied by the cranial; middle and caudal rectal arteries. Keywords: Anatomy,Arteries, Goat, Intestine I. Introduction Goats characterized by their high fertility rate and are of great economic value; being a cheap meat, milk and some industrial substances. -

PERIPHERAL VASCULATURE Average Vessel Diameter
PERIPHERAL VASCULATURE Average Vessel Diameter A Trio of Technologies. Peripheral Embolization Solutions A Single Solution. Fathom™ Steerable Guidewires Total Hypotube Tip Proximal/ UPN Length (cm) Length (cm) Length (cm) Distal O.D. Hepatic, Gastro-Intestinal and Splenic Vasculature 24 8-10 mm Common Iliac Artery 39 2-4 mm Internal Pudendal Artery M00150 900 0 140 10 10 cm .016 in 25 6-8 mm External Iliac Artery 40 2-4 mm Middle Rectal M00150 901 0 140 20 20 cm .016 in 26 4-6 mm Internal Iliac Artery 41 2-4 mm Obturator Artery M00150 910 0 180 10 10 cm .016 in 27 5-8 mm Renal Vein 42 2-4 mm Inferior Vesical Artery 28 43 M00150 911 0 180 20 20 cm .016 in 15-25 mm Vena Cava 2-4 mm Superficial Epigastric Artery 29 44 M00150 811 0 200 10 10 cm pre-shaped .014 in 6-8 mm Superior Mesenteric Artery 5-8 mm Femoral Artery 30 3-5 mm Inferior Mesenteric Artery 45 2-4 mm External Pudendal Artery M00150 810 0 200 10 10 cm .014 in 31 1-3 mm Intestinal Arteries M00150 814 0 300 10 10 cm .014 in 32 Male 2-4 mm Superior Rectal Artery A M00150 815 0 300 10 10 cm .014 in 33 1-3 mm Testicular Arteries 1-3 mm Middle Sacral Artery B 1-3 mm Testicular Veins 34 2-4 mm Inferior Epigastric Artery Direxion™ Torqueable Microcatheters 35 2-4 mm Iliolumbar Artery Female 36 2-4 mm Lateral Sacral Artery C 1-3 mm Ovarian Arteries Usable 37 D UPN Tip Shape RO Markers 3-5 mm Superior Gluteal Artery 1-3 mm Ovarian Veins Length (cm) 38 2-4 mm Inferior Gluteal Artery E 2-4 mm Uterine Artery M001195200 105 Straight 1 M001195210 130 Straight 1 M001195220 155 Straight 1 Pelvic -

Vessels and Circulation
CARDIOVASCULAR SYSTEM OUTLINE 23.1 Anatomy of Blood Vessels 684 23.1a Blood Vessel Tunics 684 23.1b Arteries 685 23.1c Capillaries 688 23 23.1d Veins 689 23.2 Blood Pressure 691 23.3 Systemic Circulation 692 Vessels and 23.3a General Arterial Flow Out of the Heart 693 23.3b General Venous Return to the Heart 693 23.3c Blood Flow Through the Head and Neck 693 23.3d Blood Flow Through the Thoracic and Abdominal Walls 697 23.3e Blood Flow Through the Thoracic Organs 700 Circulation 23.3f Blood Flow Through the Gastrointestinal Tract 701 23.3g Blood Flow Through the Posterior Abdominal Organs, Pelvis, and Perineum 705 23.3h Blood Flow Through the Upper Limb 705 23.3i Blood Flow Through the Lower Limb 709 23.4 Pulmonary Circulation 712 23.5 Review of Heart, Systemic, and Pulmonary Circulation 714 23.6 Aging and the Cardiovascular System 715 23.7 Blood Vessel Development 716 23.7a Artery Development 716 23.7b Vein Development 717 23.7c Comparison of Fetal and Postnatal Circulation 718 MODULE 9: CARDIOVASCULAR SYSTEM mck78097_ch23_683-723.indd 683 2/14/11 4:31 PM 684 Chapter Twenty-Three Vessels and Circulation lood vessels are analogous to highways—they are an efficient larger as they merge and come closer to the heart. The site where B mode of transport for oxygen, carbon dioxide, nutrients, hor- two or more arteries (or two or more veins) converge to supply the mones, and waste products to and from body tissues. The heart is same body region is called an anastomosis (ă-nas ′tō -mō′ sis; pl., the mechanical pump that propels the blood through the vessels. -

Colon Operative Standards
282 SECTION IV | COLON F G E F FIGURE 16-7 (Continued). patients with hereditary nonpolyposis colon cancer, as they have a higher incidence of synchronous and metachronous colonic tumors than do patients with sporadic colorectal cancer. As calculated by life table analysis, the risk for metachronous cancer among patients with hereditary nonpolyposis is as high as 40% at 10 years. Simi- larly, for colon cancer patients with familial adenomatous polyposis, surgical resec- tion should consist of either total abdominal colectomy or total proctocolectomy. The choice between these two operations depends on the burden of polypoid disease in the rectum and the patient’s preference for close surveillance. 7,8,9 Finally, individuals who develop colon cancer in the setting of long-standing ulcerative colitis require a total proctocolectomy. The oncologic principles of colon cancer surgery as outlined in this chapter, including the attention to surgical margins and the need for proximal vascular ligation, should be adhered to bilaterally, not just for the portion of colon in which the tumor has been identifi ed.10,11 3. PROXIMAL VASCULAR LIGATION AND REGIONAL LYMPHADENECTOMY Recommendation: Resection of the tumor-bearing bowel segment and radical lymphadenectomy should be performed en bloc with proximal vascular ligation at the origin of the primary feeding vessel(s). Copyright © 2015 Wolters Kluwer Health, Inc. Unauthorized reproduction of the article is prohibited. 226_ACS_Ch16.indd6_ACS_Ch16.indd 228282 44/3/15/3/15 22:58:58 AAMM CHAPTER 16 | Colon Resection 283 Type of Data: Prospective and retrospective observational studies. Strength of Recommendation: Moderate. Rationale The standard of practice for the treatment of stage I to III (nonmetastatic) colon can- cer is complete margin-negative resection (R0 resection) of the tumor-bearing bowel combined with en bloc resection of the intact node-bearing mesentery (i.e., regional lymphadenectomy). -

Anomalous Vascular Peritoneal Band Causing Small Bowel Obstruction in an Adult
CASE REPORT Anomalous Vascular Peritoneal Band Causing Small Bowel Obstruction in an Adult Suzanne Nyakirugumi, Mathenge Nduhiu Nyeri County Referral Hospital, Nyeri, Kenya Correspondence to: Dr. Suzanne Nyakirugumi; Email:[email protected] Summary Peritoneal bands resulting in small bowel obstruction in band. This is the first reported case in Sub-Saharan adults are rare. We present a case study of a 39-year-old Africa. male who presented with a 10-day history of signs and symptoms of intestinal obstruction. The patient had no history of abdominal trauma or surgery. Intraoperatively, Keywords: Small bowel obstruction, Congenital bands, the small bowel obstruction was caused by a vascularized Peritoneal bands, Vascular bands, Inferior mesenteric peritoneal band that had a membrane. The band formed a artery, Superior mesenteric artery closed loop and caused the small bowel to herniate and Ann Afr Surg. 2020; 17(2):85-87 lead to mechanical obstruction. In the band was an DOI: http://dx.doi.org/10.4314/aas.v17i2.10 anomalous artery that connected the ileocolic artery to Conflicts of Interest: None the descending branch of the left colic artery. The Funding: None mainstay for diagnosis is an exploratory laparoscopy or © 2020 Author. This work is licensed under the Creative laparotomy. The definitive treatment is transection of the Commons Attribution 4.0 International License. Introduction past. He also had no comorbidity. The patient was alert We present a case study of a 39-year-old male with a 10- and sick looking on physical examination. His pulse rate day history of obstipation resulting from a vascular was 109 beats per minute, respiratory rate was 22 breaths anomalous peritoneal band. -
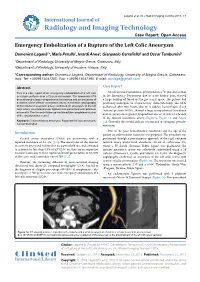
Emergency Embolization of a Rupture of the Left Colic Aneurysm
Laganà et al. Int J Radiol Imaging Technol 2015, 1:1 International Journal of Radiology and Imaging Technology Case Report: Open Access Emergency Embolization of a Rupture of the Left Colic Aneurysm Domenico Laganà1*, Maria Petullà1, Ierardi Anna2, Gianpaolo Carrafiello2 and Oscar Tamburrini1 1Department of Radiology, University of Magna Grecia, Catanzaro, Italy 2Department of Radiology, University of Insubria, Varese, Italy *Corresponding author: Domenico Laganà, Department of Radiology, University of Magna Grecia, Catanzaro, Italy, Tel: +3909613647285, Fax: +3909613647395, E-mail: [email protected] Abstract Case Report This is a case report of an emergency embolization of a left colic An ultrasound examination, performed on a 72-year-old woman aneurysm performed on a 72-year-old woman. The abdominal CTA in the Emergency Department due to acute lumbar pain, showed scan showed a large retroperitoneal hematoma and an aneurysm of a large buildup of blood in the pre-sacral space. The patient had a branch of the inferior mesenteric artery. A selective angiography previously undergone to a laparoscopic cholecystectomy. The CTA, of the inferior mesenteric artery confirmed an aneurysm of the left performed after two hours, due to a sudden hemorrhagic shock colic artery. An endovascular ligation was performed with platinum (arterial pressure 90/50), showed a large retroperitoneal hematoma microcoils. The 3-month follow-up confirmed the complete exclusion of the aneurysmatic vessel. and an aneurysm at greater longitudinal axis of 18 mm of a branch of the inferior mesenteric artery (Figure1a, Figure 1b and Figure Keywords: Visceral artery aneurysm, Ruptured left colic aneurysm, 1c). Generally this would indicate a traumatic or iatrogenic pseudo- Coil embolization aneurysm. -

Concurrent Origin of Right Gastroepiploic and Left Colic Arteries from Inferior Pancreaticoduodenal Artery: Rare Variation of Splanchnic Anastomosis
DOI: 10.5958/2319-5886.2015.00142.3 International Journal of Medical Research & Health Sciences www.ijmrhs.com Volume 4 Issue 3 Coden: IJMRHS Copyright @2015 ISSN: 2319-5886 Received: 27th Apr 2015 Revised: 10th May 2015 Accepted: 25th May 2015 Case report CONCURRENT ORIGIN OF RIGHT GASTROEPIPLOIC AND LEFT COLIC ARTERIES FROM INFERIOR PANCREATICODUODENAL ARTERY: RARE VARIATION OF SPLANCHNIC ANASTOMOSIS *Mutalik Maitreyee M Assistant Professor, Department of Anatomy, MIMER Medical College, Talegaon Dabhade, Pune, India *Corresponding author email: [email protected] ABSTRACT In the present case, inferior pancreaticoduodenal artery, the first branch of superior mesenteric artery, was exceptionally giving rise to right gastroepiploic artery and left colic artery simultaneously. Right gastroepiploic artery is a branch of foregut artery, while left colic artery is a branch of hindgut artery. Concurrent origin of branches of foregut as well as hindgut arteries from a midgut artery i.e. superior mesenteric artery is very rare. Usual left colic artery from inferior mesenteric artery was also present but was supplying smaller area than usual. It can be explained as persistence of unusual channels and obliteration of usual ones along the dorsal splanchnic anastomosis during the embryonic development. The field of vascularization of superior mesenteric artery was extended beyond its usual boundaries both proximally as well as distally, which is clinically important as unawareness of the variations may lead to significant morbidity and mortality. Keywords: Bypass graft, Colic artery, Gastroepiploic artery, Pancreaticoduodenal artery, Splanchnic anastomosis, Mesenteric artery INTRODUCTION Fields of vascularization of celiac trunk (CT), gastroduodenal artery (GDA), arising from hepatic superior mesenteric artery (SMA), and inferior branch of CT (foregut artery). -
Variations in the Origin and Colic Branches of the Superior Mesenteric Artery
VARIATIONS IN THE ORIGIN AND COLIC BRANCHES OF THE SUPERIOR MESENTERIC ARTERY Dissertation Submitted to THE TAMIL NADU DR. M.G.R. MEDICAL UNIVERSITY CHENNAI in partial fulfillment of the regulations for the award of the degree of M.S. (Anatomy) BRANCH - V THE TAMILNADU DR. M.G.R. MEDICAL UNIVERSITY CHENNAI, INDIA. MARCH 2008 Certificate This is to certify that the dissertation title, ‘Variations in the Origin and Colic branches of the Superior Mesenteric Artery’ is an original work done by Dr. M. Nirmaladevi, PG Student, Stanley Medical College, Chennai-1, under my supervision and guidance. Dr. Mythili Bhaskaran, M.D., Dr. Sudha Seshayyan, M.S., Dean Professor and HOD Stanley Medical College Department of Anatomy Chennai-1 Stanley Medical College Chennai-1 Place: Chennai-1 Date: DECLARATION I solemnly declare that this dissertation "Variations in the Origin and Colic branches of the Superior Mesenteric Artery" was written by me in the Department of Anatomy, Govt. Stanley Medical College and Hospital, Chennai, under the guidance and supervision of Prof. Dr. Sudha Seshayyan, M.S., Professor and Head of the Department of Anatomy, Govt. Stanley Medical College, Chennai - 600 001. This dissertation is submitted to The Tamil Nadu Dr. M.G.R. Medical University, Chennai in partial fulfillment of the University regulations for the award of degree of M.S. Anatomy - Branch V examinations to be held in March 2008. Place : Chennai. Date : (Dr.M.Nirmala Devi) ACKNOWLEDGEMENT I have been overwhelmed by the support and guidance that I have received from a large number of people in completing this study and I would like to take this opportunity to thank each one of them. -

Nodal Drainage Pathways in Primary Rectal Cancer: Anatomy of Regional and Distant Nodal Spread
Abdominal Radiology (2019) 44:3527–3535 https://doi.org/10.1007/s00261-019-02094-0 SPECIAL SECTION: RECTAL CANCER Nodal drainage pathways in primary rectal cancer: anatomy of regional and distant nodal spread Harmeet Kaur1 · Randy D. Ernst1 · Gaiane M. Rauch1 · Mukesh Harisinghani2 Published online: 18 October 2019 © Springer Science+Business Media, LLC, part of Springer Nature 2019 Abstract Nodal involvement is a signifcant prognostic factor in rectal cancer and difcult to assess preoperatively. An understanding of the patterns of nodal spread from diferent regions of the rectum can assist in this process and is essential for the purposes of surgical planning. In this article we defne patterns of spread to mesenteric and pelvic sidewall nodal subgroups and discuss the importance of accurate anatomic localization of nodes for the purposes of staging and surgical planning. Keywords Rectal cancer · Rectal adenocarcinoma · Lymph node · MRI · CT Introduction The anatomic defnition of the rectum specifes its supe- rior or upper extent as the point of coalescence of the taenia Lymph node spread is an important prognostic factor in rec- to form a continuous outer longitudinal muscle layer in the tal cancer. An understanding of lymphatic drainage path- rectum. Inferiorly the anatomic rectum ends at the dentate ways from diferent regions of the rectum, the most common line, which also is the point of transition between columnar nodal groups’ involved and accurate localization of these epithelium lining the rectum and the squamous epithelium nodes to mesenteric, pelvic sidewall and retroperitoneal lining the anatomic anal canal, which extends down from the compartments is important in the accurate staging and sur- dentate line to the anal verge [1]. -

Original Article
ORIGINAL ARTICLE A STUDY OF ARTERIAL SUPPLY OF VERMIFORM APPENDIX IN HUMANS Hosmani Veeresh 1, Halasagi S. S2 1. Assistant Professor, Dept. of Anatomy, Srinivas Institute of Medical Sciences and Research Center, Mukka, Mangalore. 2. Associate Professor, Dept. of Anatomy, Srinivas Institute of Medical Sciences and Research Center, Mukka, Mangalore. CORRESPONDING AUTHOR Dr. Hosmani Veeresh, Assistant professor, Dept. of Anatomy, Srinivas institute of medical sciences and Research Center. Mukka, Mangalore E-mail: [email protected], Ph: 0091 08904390833 ABSTRACT: The surgical procedures like appendicectomy, demands a precise knowledge of vascular anatomy of ileocolic region. The aim of this study is to study the arterial supply of the appendix, findings of which may reveal more anatomical facts about the arteries of appendix and their variations. Total 52 specimens of caecum and appendix with their arteries intact were collected, cleaned and dissected. The ileocolic artery and its branches to the appendix were traced carefully and observations were recorded. The ileocolic artery arises independently from superior mesenteric artery in 96.88% of cases and ends by dividing into superior and inferior division in 93.76% of cases. The appendicular artery arises from inferior division in 46.88%, ileal branch 28.13%, ileocolic artery 18.75% and from arterial arcade in 6.25% of cases. 21.87% of cases showed additional appendicular artery. KEYWORDS: Caecum, appendix, ileocolic artery, appendicular artery. INTRODUCTION: Vascular anomalies always pose a great challenge to the anatomists and surgeons. The surgical trauma to the sustaining blood vessels is irreparable and lead to fatal necrosis of the part involved. Surgical procedures like appendicectomy, which is one of the common surgical procedures in case of appendicitis, appendicular carcinoid tumors etc. -

Variant Arterial Supply of the Descending Colon by the Coeliac Trunk: a Case Report
medicina Case Report Variant Arterial Supply of the Descending Colon by the Coeliac Trunk: A Case Report Sandra Petzold 1,†, Silke Diana Storsberg 2,†, Karin Fischer 1 and Sven Schumann 3,* 1 Institute of Anatomy, Medical Faculty, Otto-von-Guericke-University Magdeburg, 39120 Magdeburg, Germany; [email protected] (S.P.); karin.fi[email protected] (K.F.) 2 Institute for Anatomy and Clinical Morphology, School of Medicine, Faculty of Health, Witten/Herdecke University, 58448 Witten, Germany; [email protected] 3 University Medical Center, Institute for Microscopic Anatomy and Neurobiology, Johannes Gutenberg-University, 55131 Mainz, Germany * Correspondence: [email protected] † Contributed equally. Abstract: Background and Objectives: Knowledge of arterial variations of the intestines is of great importance in visceral surgery and interventional radiology. Materials and Methods: An unusual variation in the blood supply of the descending colon was observed in a Caucasian female body donor. Results: In this case, the left colic artery that regularly derives from the inferior mesenteric artery supplying the descending colon was instead a branch of the common hepatic artery. Conclusions: Here, we describe the very rare case of an aberrant left colic artery arising from the common hepatic artery in a dissection study. Keywords: left colic artery; aberrant left colic artery; common hepatic artery; arterial variations; mesenteric arteries; large intestines Citation: Petzold, S.; Storsberg, S.D.; Fischer, K.; Schumann, S. Variant 1. Introduction Arterial Supply of the Descending Accurate knowledge of large intestine vascular anatomy is of fundamental impor- Colon by the Coeliac Trunk: A Case tance, particularly in visceral surgery and interventional radiology. -

Session I - Anterior Abdominal Wall - Rectus Sheath
ABDOMEN Session I - Anterior abdominal wall - Rectus sheath Surface landmarks Dissection Costal margins- right & left S u p e r f i c i a l f a s c i a ( f a t t y l a y e r, Pubic symphysis, tubercle membranous layer) Anterior superior iliac spine External oblique muscle Iliac crest Superficial inguinal ring Umbilicus, linea semilunaris Linea alba Mid-inguinal point & Lateral and anterior cutaneous branches of lower intercostal nerves Midpoint of inguinal ligament Anterior wall of rectus sheath Transpyloric & transtubercular planes Rectus abdominis & pyramidalis Right & left lateral (vertical) planes Superior & inferior epigastric vessels Nine abdominal regions – right & left hypochondriac, epigastric, right & left Posterior wall, arcuate line lumbar, umbilical, right & left iliac fossae, Internal oblique & transversus abdominis hypogastric muscles Region of external genitalia (tenth region) Fascia transversalis Terms of common usage for regions in the abdomen — Self-study Abdomen proper, pelvis, perineum, loin, Attachments, nerve supply & actions of groin, flanks external oblique, internal oblique, t r a n s v e r s u s a b d o m i n i s , r e c t u s abdominis, pyramidalis Bones Formation, contents and applied Lumbar vertebrae, sacrum, coccyx anatomy of rectus sheath Nerve supply, blood supply & lymphatic drainage of anterior abdominal wall ABDOMEN Session II - Inguinal Canal Dissection Self-study Aponeurosis of external oblique Boundaries of inguinal canal Superficial inguinal ring Contents of inguinal canal (in males and Inguinal