Testicular Artery Arising from an Aberrant Right Renal Artery
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

PERIPHERAL VASCULATURE Average Vessel Diameter
PERIPHERAL VASCULATURE Average Vessel Diameter A Trio of Technologies. Peripheral Embolization Solutions A Single Solution. Fathom™ Steerable Guidewires Total Hypotube Tip Proximal/ UPN Length (cm) Length (cm) Length (cm) Distal O.D. Hepatic, Gastro-Intestinal and Splenic Vasculature 24 8-10 mm Common Iliac Artery 39 2-4 mm Internal Pudendal Artery M00150 900 0 140 10 10 cm .016 in 25 6-8 mm External Iliac Artery 40 2-4 mm Middle Rectal M00150 901 0 140 20 20 cm .016 in 26 4-6 mm Internal Iliac Artery 41 2-4 mm Obturator Artery M00150 910 0 180 10 10 cm .016 in 27 5-8 mm Renal Vein 42 2-4 mm Inferior Vesical Artery 28 43 M00150 911 0 180 20 20 cm .016 in 15-25 mm Vena Cava 2-4 mm Superficial Epigastric Artery 29 44 M00150 811 0 200 10 10 cm pre-shaped .014 in 6-8 mm Superior Mesenteric Artery 5-8 mm Femoral Artery 30 3-5 mm Inferior Mesenteric Artery 45 2-4 mm External Pudendal Artery M00150 810 0 200 10 10 cm .014 in 31 1-3 mm Intestinal Arteries M00150 814 0 300 10 10 cm .014 in 32 Male 2-4 mm Superior Rectal Artery A M00150 815 0 300 10 10 cm .014 in 33 1-3 mm Testicular Arteries 1-3 mm Middle Sacral Artery B 1-3 mm Testicular Veins 34 2-4 mm Inferior Epigastric Artery Direxion™ Torqueable Microcatheters 35 2-4 mm Iliolumbar Artery Female 36 2-4 mm Lateral Sacral Artery C 1-3 mm Ovarian Arteries Usable 37 D UPN Tip Shape RO Markers 3-5 mm Superior Gluteal Artery 1-3 mm Ovarian Veins Length (cm) 38 2-4 mm Inferior Gluteal Artery E 2-4 mm Uterine Artery M001195200 105 Straight 1 M001195210 130 Straight 1 M001195220 155 Straight 1 Pelvic -

Bilateral Variations of the Testicular Vessels: Embryological Background and Clinical Implications
Case Report Bilateral Variations of the Testicular Vessels: Embryological Background and Clinical Implications Yogesh Diwan, Rikki Singal1, Deepa Diwan, Subhash Goyal1, Samita Singal2, Mausam Kapil1 Department of Anatomy, Indira Gandhi Medical College, Shimla, 1Surgery and 2Radiology, Maharishi Markandeshwer Institute of Medical Sciences and Research, Mullana, Ambala, India ABSTRACT Variations of the testicular vessels were observed during routine dissection of the posterior abdominal wall in a male North Indian cadaver. On the right side, the testicular vein drained into the right renal vein and the right testicular artery passed posterior to the inferior vena cava. The left testicular vein was composed of the lateral and medial testicular veins which drained into the left renal vein independently. Left renal vein had received an additional tributary, first lumbar vein, and the left testicular artery had hooked this additional tributary to run along its normal course. KEY WORDS: Inferior vena cava, renal vein, testicular artery, testicular vein INTRODUCTION vessels are relatively constant, occasional developmental and anatomical variations have been reported. However, The testicular arteries arise anteriorly from the abdominal variations of the testicular veins associated with variations aorta, a little inferior to the renal arteries. The vertebral level of the testicular arteries are seldom seen.[3] of their origin varies from the 1st to the 3rd lumbar vertebrae. Each passes inferolaterally under the parietal peritoneum In the present report, we investigate the drainage, course, on the psoas major. The right testicular artery commonly tributaries of the testicular veins, the origin and course of passes ventrally to the inferior vena cava. Each artery crosses the testicular arteries, and discuss their embryogenesis and anterior to the genitofemoral nerve, ureter and the lower clinical significance. -

Arched Left Gonadal Artery Over the Left Renal Vein Associated with Double Left Renal Artery Ranade a V, Rai R, Prahbu L V, Mangala K, Nayak S R
Case Report Singapore Med J 2007; 48(12) : e332 Arched left gonadal artery over the left renal vein associated with double left renal artery Ranade A V, Rai R, Prahbu L V, Mangala K, Nayak S R ABSTRACT Variations in the anatomical relationship of the gonadal arteries to the renal vessels are frequently reported. We present, on a male cadaver, an unusual origin and course of a left testicular artery arching over the left renal vein along with double renal arteries. The development of this anomaly is discussed in detail. Compression of the left renal vein between the abdominal aorta and the superior mesenteric artery usually induces left renal vein hypertension, resulting in varicocele. We propose that the arching of left testicular artery over the left renal vein could be an additional possible cause of the left renal vein compression. Therefore, knowledge of the possible existence of arching gonadal vessels in relation to the renal vein could be of paramount importance to vascular surgeons and urologists during surgery in Fig. 1 Photograph shows the left testicular artery along with the retroperitoneal region. double left renal arteries after reflecting the inferior vena cava Department of downwards. Anatomy, 1. Left testicular artery; 2. Left kidney; 3. Left renal vein; Kasturba Medical 4. Inferior vena cava; 5. Abdominal aorta; 8. Superior left College, Keywords: anomalous gonadal vessels, Mangalore 575004, arched left gonadal artery, gonadal artery renal artery; 9. Inferior left renal artery; and 10. Double left Karnataka, renal vein. -

Colon Operative Standards
282 SECTION IV | COLON F G E F FIGURE 16-7 (Continued). patients with hereditary nonpolyposis colon cancer, as they have a higher incidence of synchronous and metachronous colonic tumors than do patients with sporadic colorectal cancer. As calculated by life table analysis, the risk for metachronous cancer among patients with hereditary nonpolyposis is as high as 40% at 10 years. Simi- larly, for colon cancer patients with familial adenomatous polyposis, surgical resec- tion should consist of either total abdominal colectomy or total proctocolectomy. The choice between these two operations depends on the burden of polypoid disease in the rectum and the patient’s preference for close surveillance. 7,8,9 Finally, individuals who develop colon cancer in the setting of long-standing ulcerative colitis require a total proctocolectomy. The oncologic principles of colon cancer surgery as outlined in this chapter, including the attention to surgical margins and the need for proximal vascular ligation, should be adhered to bilaterally, not just for the portion of colon in which the tumor has been identifi ed.10,11 3. PROXIMAL VASCULAR LIGATION AND REGIONAL LYMPHADENECTOMY Recommendation: Resection of the tumor-bearing bowel segment and radical lymphadenectomy should be performed en bloc with proximal vascular ligation at the origin of the primary feeding vessel(s). Copyright © 2015 Wolters Kluwer Health, Inc. Unauthorized reproduction of the article is prohibited. 226_ACS_Ch16.indd6_ACS_Ch16.indd 228282 44/3/15/3/15 22:58:58 AAMM CHAPTER 16 | Colon Resection 283 Type of Data: Prospective and retrospective observational studies. Strength of Recommendation: Moderate. Rationale The standard of practice for the treatment of stage I to III (nonmetastatic) colon can- cer is complete margin-negative resection (R0 resection) of the tumor-bearing bowel combined with en bloc resection of the intact node-bearing mesentery (i.e., regional lymphadenectomy). -

Triple Renal Arteries of the Left Kidney with Aberrant Left Gonadal Artery
Innovative Journal of Medical and Health Science 3 : 4 July – August. (2013) 197 - 200. Contents lists available at www.innovativejournal.in INNOVATIVE JOURNAL OF MEDICAL AND HEALTH SCIENCE Journal homepage: http://www.innovativejournal.in/index.php/ijmhs TRIPLE RENAL ARTERIES OF THE LEFT KIDNEY WITH ABERRANT LEFT GONADAL ARTERY 1 2 3 3 4 Dr. Sreekanth Tallapaneni , DR. Chandramala , Shashank Kumar Srivastav , Shaik Zakir Hussain , Samia Azaz . Department of Anatomy, Shadan Institute of Medical Sciences, Teaching Hospital & Research Centre. Hyderabad. ARTICLE INFO ABSTRACT Corresponding Author: Objective: Dr. Sreekanth T, Associate Professor, The purpose of this case report is to bring into light about three renal Department of Anatomy, Shadan arteries supplying the left kidney which is a rarity. The cranial and caudal Institute of Medical Sciences, accessory renal arteries were of aortic in origin and had significance lumen Teaching Hospital & Research Centre. size. The cranial artery terminated into two segmental arteries. The caudal Peerancheruvu Hyderabad. renal artery gave rise to the left gonadal artery and the point of emergence of it showed a deep kink. Materials And Methods: A formalin – fixed elderly male cadaver along with Routine instruments including Scalpel, Blade, Surgical forceps, Anatomical Forceps, Dissector, Metallic Scale with Calibrations along with a Key words: (Accessory renal artery) pair of gloves were used. The anterior abdominal wall was dissected layer (Tortuous) (Left gonadal artery) by layer. The reflection of the peritoneum was traced both horizontally and (segmental branches) vertically The visceral organs like liver, stomach & intestines were all studied in Situ and dissected out. The duodenum, pancreas and spleen were all dissected away from the abdominal cavity and the peritoneum was stripped to visualize the kidneys. -
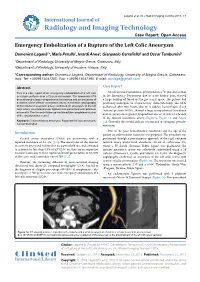
Emergency Embolization of a Rupture of the Left Colic Aneurysm
Laganà et al. Int J Radiol Imaging Technol 2015, 1:1 International Journal of Radiology and Imaging Technology Case Report: Open Access Emergency Embolization of a Rupture of the Left Colic Aneurysm Domenico Laganà1*, Maria Petullà1, Ierardi Anna2, Gianpaolo Carrafiello2 and Oscar Tamburrini1 1Department of Radiology, University of Magna Grecia, Catanzaro, Italy 2Department of Radiology, University of Insubria, Varese, Italy *Corresponding author: Domenico Laganà, Department of Radiology, University of Magna Grecia, Catanzaro, Italy, Tel: +3909613647285, Fax: +3909613647395, E-mail: [email protected] Abstract Case Report This is a case report of an emergency embolization of a left colic An ultrasound examination, performed on a 72-year-old woman aneurysm performed on a 72-year-old woman. The abdominal CTA in the Emergency Department due to acute lumbar pain, showed scan showed a large retroperitoneal hematoma and an aneurysm of a large buildup of blood in the pre-sacral space. The patient had a branch of the inferior mesenteric artery. A selective angiography previously undergone to a laparoscopic cholecystectomy. The CTA, of the inferior mesenteric artery confirmed an aneurysm of the left performed after two hours, due to a sudden hemorrhagic shock colic artery. An endovascular ligation was performed with platinum (arterial pressure 90/50), showed a large retroperitoneal hematoma microcoils. The 3-month follow-up confirmed the complete exclusion of the aneurysmatic vessel. and an aneurysm at greater longitudinal axis of 18 mm of a branch of the inferior mesenteric artery (Figure1a, Figure 1b and Figure Keywords: Visceral artery aneurysm, Ruptured left colic aneurysm, 1c). Generally this would indicate a traumatic or iatrogenic pseudo- Coil embolization aneurysm. -

Concurrent Origin of Right Gastroepiploic and Left Colic Arteries from Inferior Pancreaticoduodenal Artery: Rare Variation of Splanchnic Anastomosis
DOI: 10.5958/2319-5886.2015.00142.3 International Journal of Medical Research & Health Sciences www.ijmrhs.com Volume 4 Issue 3 Coden: IJMRHS Copyright @2015 ISSN: 2319-5886 Received: 27th Apr 2015 Revised: 10th May 2015 Accepted: 25th May 2015 Case report CONCURRENT ORIGIN OF RIGHT GASTROEPIPLOIC AND LEFT COLIC ARTERIES FROM INFERIOR PANCREATICODUODENAL ARTERY: RARE VARIATION OF SPLANCHNIC ANASTOMOSIS *Mutalik Maitreyee M Assistant Professor, Department of Anatomy, MIMER Medical College, Talegaon Dabhade, Pune, India *Corresponding author email: [email protected] ABSTRACT In the present case, inferior pancreaticoduodenal artery, the first branch of superior mesenteric artery, was exceptionally giving rise to right gastroepiploic artery and left colic artery simultaneously. Right gastroepiploic artery is a branch of foregut artery, while left colic artery is a branch of hindgut artery. Concurrent origin of branches of foregut as well as hindgut arteries from a midgut artery i.e. superior mesenteric artery is very rare. Usual left colic artery from inferior mesenteric artery was also present but was supplying smaller area than usual. It can be explained as persistence of unusual channels and obliteration of usual ones along the dorsal splanchnic anastomosis during the embryonic development. The field of vascularization of superior mesenteric artery was extended beyond its usual boundaries both proximally as well as distally, which is clinically important as unawareness of the variations may lead to significant morbidity and mortality. Keywords: Bypass graft, Colic artery, Gastroepiploic artery, Pancreaticoduodenal artery, Splanchnic anastomosis, Mesenteric artery INTRODUCTION Fields of vascularization of celiac trunk (CT), gastroduodenal artery (GDA), arising from hepatic superior mesenteric artery (SMA), and inferior branch of CT (foregut artery). -

Bilateral Origin of the Testicular Arteries from the Lower Polar Accessory Renal Arteries
Int. J. Morphol., 30(4):1316-1320, 2012. Bilateral Origin of the Testicular Arteries from the Lower Polar Accessory Renal Arteries Origen Bilateral de las Arterias Testiculares desde las Arterias Renales Polares Inferiores Accesorias Eleni Panagouli; Evangelos Lolis & Dionysios Venieratos PANAGOULI, E.; LOLIS, E. & VENIERATOS, D. Bilateral origin of the testicular arteries from the lower polar accessory renal arteries. Int. J. Morphol., 30(4):1316-1320, 2012. SUMMARY: The gonadal arteries (testicular or ovarian arteries) emerge normally from the lateral aspect of the abdominal aorta, a little inferior to the renal arteries. Several other sites of origin of these arteries have been recorded with the renal and accessory renal arteries being the most common. In the present case report, the testicular arteries originated from the lower polar accessory renal arteries in both sides. The testicular veins followed had the usual origin and course, while an accessory renal vein was observed only in the right side. These anomalies were combined with an abnormal left ureter exiting from the lower pole of the kidney. Only one male cadaver among 77 adult human cadavers of Caucasian origin presented this set of variations (frequency: ≤ 1.3%). Variations of renal and gonadal vessels are important, as their presence could result in vascular injury of any accessory or aberrant vessel if the surgeon does not identify them. KEY WORDS: Gonadal arteries; Kidney; Ureter; Abdominal aorta. INTRODUCTION The gonadal arteries (GA), described as one of the anatomic variation of the renal arteries (RA) (Tarzamni et paired branches of the abdominal aorta (AA), emerge al., 2008) with an incidence, which ranges from 8.7 % to normally a little inferior to the renal arteries (Standring et 75.7 % (Satyapal et al., 2001). -

Variation in the Origin of the Testicular Arteries and Drainage of the Right Testicular Vein
Int. J. Morphol., 29(2):614-616, 2011. Variation in the Origin of the Testicular Arteries and Drainage of the Right Testicular Vein Variación en el Origen de las Arterias Testiculares y el Drenaje de la Vena Testicular Derecha *Royana Singh; **Amit Jaiswal; *S. N. Shamal & ***S. P. Singh SINGH, R.; JAISWAL, A.; SHAMAL, S. N. & SINGH, S. P. Variation in the origin of the testicular arteries and drainage of the right testicular vein. Int. J. Morphol., 29(2):614-616, 2011. SUMMARY: During routine dissection of a 42 year old male Indian cadaver posterior abdominal wall, variations in the testicular vessels were observed. The right testicular artery arose from the right accessory renal artery, which originated from the ventral aspect of the abdominal aorta. The left testicular artery originated from the ventral aspect of the aorta in almost the same horizontal line as the right accessory renal artery, just below the superior mesenteric artery and 1.79 cm, above the origin of the renal arteries. The right vein drained into the right accessory renal vein instead of the inferior vena cava, while the left testicular vein drained into the left renal vein. The presence of variation of both the testicular arteries as well as the testicular vein is seldom seen together. KEY WORDS: Accessory Renal Artery; Renal artery; Renal vein; Testicular artery; Testicular Vein. INTRODUCTION MATERIAL AND METHOD The testicular arteries arise from the ventral aspect During the routine dissection of 10 cadavers for the of the abdominal aorta below the renal artery at the level of undergraduate classes, a 42 year old male cadaver of Indian the second lumbar vertebra. -
Variations in the Origin and Colic Branches of the Superior Mesenteric Artery
VARIATIONS IN THE ORIGIN AND COLIC BRANCHES OF THE SUPERIOR MESENTERIC ARTERY Dissertation Submitted to THE TAMIL NADU DR. M.G.R. MEDICAL UNIVERSITY CHENNAI in partial fulfillment of the regulations for the award of the degree of M.S. (Anatomy) BRANCH - V THE TAMILNADU DR. M.G.R. MEDICAL UNIVERSITY CHENNAI, INDIA. MARCH 2008 Certificate This is to certify that the dissertation title, ‘Variations in the Origin and Colic branches of the Superior Mesenteric Artery’ is an original work done by Dr. M. Nirmaladevi, PG Student, Stanley Medical College, Chennai-1, under my supervision and guidance. Dr. Mythili Bhaskaran, M.D., Dr. Sudha Seshayyan, M.S., Dean Professor and HOD Stanley Medical College Department of Anatomy Chennai-1 Stanley Medical College Chennai-1 Place: Chennai-1 Date: DECLARATION I solemnly declare that this dissertation "Variations in the Origin and Colic branches of the Superior Mesenteric Artery" was written by me in the Department of Anatomy, Govt. Stanley Medical College and Hospital, Chennai, under the guidance and supervision of Prof. Dr. Sudha Seshayyan, M.S., Professor and Head of the Department of Anatomy, Govt. Stanley Medical College, Chennai - 600 001. This dissertation is submitted to The Tamil Nadu Dr. M.G.R. Medical University, Chennai in partial fulfillment of the University regulations for the award of degree of M.S. Anatomy - Branch V examinations to be held in March 2008. Place : Chennai. Date : (Dr.M.Nirmala Devi) ACKNOWLEDGEMENT I have been overwhelmed by the support and guidance that I have received from a large number of people in completing this study and I would like to take this opportunity to thank each one of them. -

Nodal Drainage Pathways in Primary Rectal Cancer: Anatomy of Regional and Distant Nodal Spread
Abdominal Radiology (2019) 44:3527–3535 https://doi.org/10.1007/s00261-019-02094-0 SPECIAL SECTION: RECTAL CANCER Nodal drainage pathways in primary rectal cancer: anatomy of regional and distant nodal spread Harmeet Kaur1 · Randy D. Ernst1 · Gaiane M. Rauch1 · Mukesh Harisinghani2 Published online: 18 October 2019 © Springer Science+Business Media, LLC, part of Springer Nature 2019 Abstract Nodal involvement is a signifcant prognostic factor in rectal cancer and difcult to assess preoperatively. An understanding of the patterns of nodal spread from diferent regions of the rectum can assist in this process and is essential for the purposes of surgical planning. In this article we defne patterns of spread to mesenteric and pelvic sidewall nodal subgroups and discuss the importance of accurate anatomic localization of nodes for the purposes of staging and surgical planning. Keywords Rectal cancer · Rectal adenocarcinoma · Lymph node · MRI · CT Introduction The anatomic defnition of the rectum specifes its supe- rior or upper extent as the point of coalescence of the taenia Lymph node spread is an important prognostic factor in rec- to form a continuous outer longitudinal muscle layer in the tal cancer. An understanding of lymphatic drainage path- rectum. Inferiorly the anatomic rectum ends at the dentate ways from diferent regions of the rectum, the most common line, which also is the point of transition between columnar nodal groups’ involved and accurate localization of these epithelium lining the rectum and the squamous epithelium nodes to mesenteric, pelvic sidewall and retroperitoneal lining the anatomic anal canal, which extends down from the compartments is important in the accurate staging and sur- dentate line to the anal verge [1]. -

Anatomy of the Abdominal Aorta in the Hoary Fox (Lycalopex Vetulus, Lund, 1842)
1 Anatomy of the abdominal aorta in the hoary fox (Lycalopex vetulus, Lund, 1842) Anatomia da aorta abdominal em raposa-do-campo (Lycalopex vetulus, Lund, 1842) Dara Rúbia Souza SILVA1; Mônica Duarte da SILVA1; Marcos Paulo Batista de ASSUNÇÃO1; Eduardo Paul CHACUR1; Daniela Cristina de Oliveira SILVA2; Roseâmely Angélica de Carvalho BARROS1; Zenon SILVA1 1 Universidade Federal de Goiás, Regional Catalão, Instituto de Biotecnologia, Departamento de Ciências Biológicas, Catalão – GO, Brazil 2 Universidade Federal de Uberlândia, Instituto de Ciências Biomédicas, Departamento de Anatomia Humana, Uberlândia – MG, Brazil Abstract The hoary fox (Lycalopex vetulus, Lund, 1842) is the smallest Brazilian canid, whose weight varies between 2 and 4 kg, has a slender body, a small head, and a short and blackened snout. Despite being considered an endemic species, little is known about the hoary fox as it is one of the seven less studied canids in the world. Thus, this study aimed to describe the anatomy of the abdominal aorta artery of the hoary fox and to compare it with the pre-established literature data in domestic canids. For this purpose, we used two adult hoary foxes without definite age. We collected the corpses of these animals along roadsides of Catalão-GO, being later fixed and conserved in a 10% formalin solution. The results showed that the abdominal aorta in hoary fox is at the ventral face of the lumbar region vertebral bodies, being slightly displaced to the left of the median plane. The first branch is visceral, named celiac artery, followed by a paired parietal branch: the phrenic abdominal arteries.