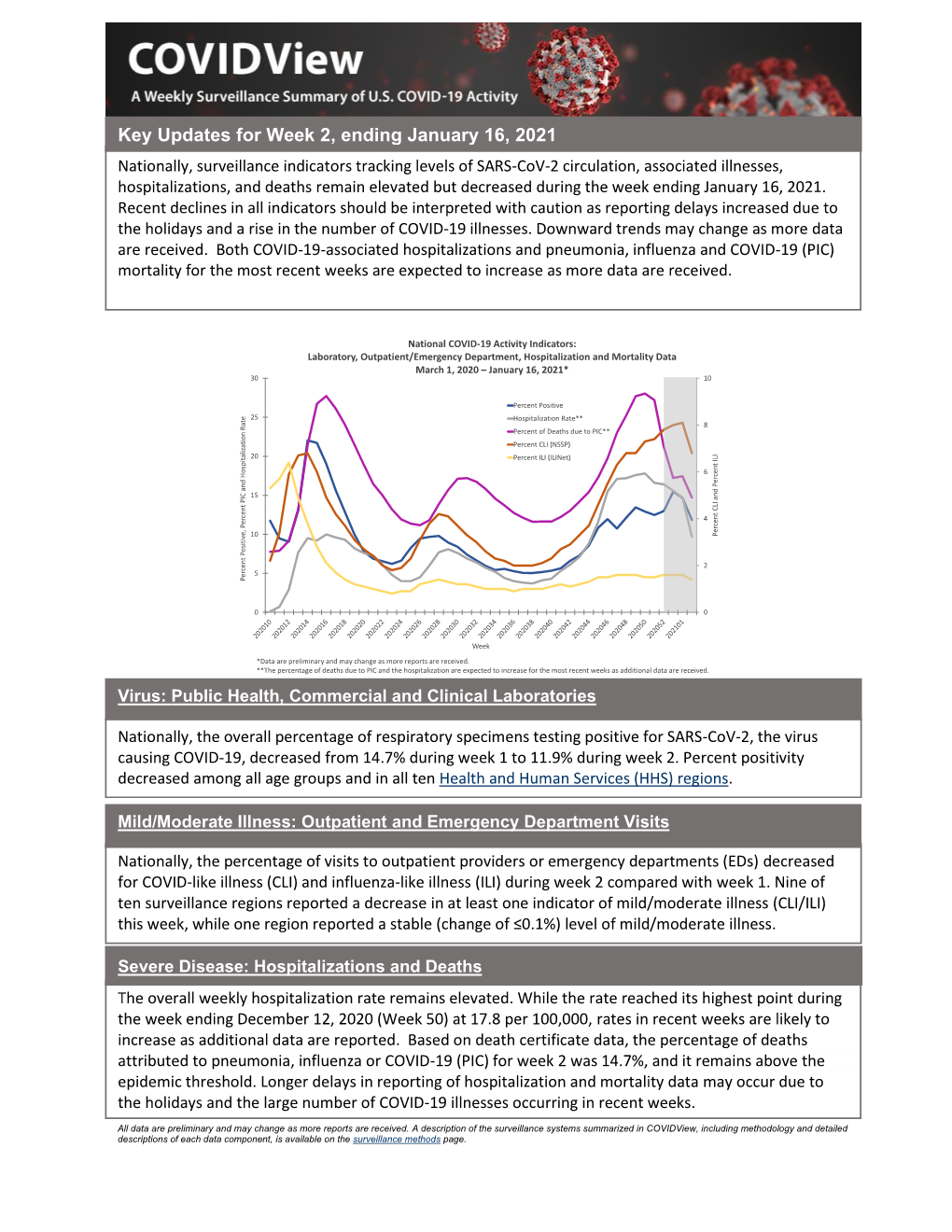
January 16, 2021
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

2021 7 Day Working Days Calendar
2021 7 Day Working Days Calendar The Working Day Calendar is used to compute the estimated completion date of a contract. To use the calendar, find the start date of the contract, add the working days to the number of the calendar date (a number from 1 to 1000), and subtract 1, find that calculated number in the calendar and that will be the completion date of the contract Date Number of the Calendar Date Friday, January 1, 2021 133 Saturday, January 2, 2021 134 Sunday, January 3, 2021 135 Monday, January 4, 2021 136 Tuesday, January 5, 2021 137 Wednesday, January 6, 2021 138 Thursday, January 7, 2021 139 Friday, January 8, 2021 140 Saturday, January 9, 2021 141 Sunday, January 10, 2021 142 Monday, January 11, 2021 143 Tuesday, January 12, 2021 144 Wednesday, January 13, 2021 145 Thursday, January 14, 2021 146 Friday, January 15, 2021 147 Saturday, January 16, 2021 148 Sunday, January 17, 2021 149 Monday, January 18, 2021 150 Tuesday, January 19, 2021 151 Wednesday, January 20, 2021 152 Thursday, January 21, 2021 153 Friday, January 22, 2021 154 Saturday, January 23, 2021 155 Sunday, January 24, 2021 156 Monday, January 25, 2021 157 Tuesday, January 26, 2021 158 Wednesday, January 27, 2021 159 Thursday, January 28, 2021 160 Friday, January 29, 2021 161 Saturday, January 30, 2021 162 Sunday, January 31, 2021 163 Monday, February 1, 2021 164 Tuesday, February 2, 2021 165 Wednesday, February 3, 2021 166 Thursday, February 4, 2021 167 Date Number of the Calendar Date Friday, February 5, 2021 168 Saturday, February 6, 2021 169 Sunday, February -

January 17, 2021 - VOLUME XXI - Bulletin #03
Saint Ann of the Dunes - Beverly Shores, Indiana 46301-0727 - January 16 - January 17, 2021 - VOLUME XXI - Bulletin #03 SECOND SUNDAY IN ORDINARY TIME Second Sunday in Ordinary Time 1 Samuel 3:3b-10, 19 SLEEP ON IT Sleep on it. It may be clearer in the morning. Many of the problems that seem unsolvable by day disintegrate with the dawn. It’s almost as if God speaks to us when we sleep. It happened to Samuel. Even while he was a young child, Samuel heard the voice of God calling him. But he did not know that it was God. CURRENT WEEK He told Eli the priest. Eli did not know that it was God. Not until God SECOND SUNDAY IN ORDINARY TIME spoke for the third time did Eli figure out the mystery. God was speaking • Saturday, January 16 - 6:00 PM to Samuel in his sleep. Intention: ALL SOULS REMEMBRANCE of David Hamilla and Eli gave Samuel some very simple advice: Listen. If God is trying to Terrence Murphy from Barbara Plampin speak to you, listen. Tell God you are listening. MASS FOR OUR LITHUANIAN COMMUNITY Too often our world is cluttered with unnecessary noise. We leave the • Sunday, January 17 - 1:00 PM television on when no one is watching. We turn on the radio behind our Intention: For the People of St. Ann conversation with a friend. We disturb our neighbors by playing music loudly in public or using car horns instead of doorbells. Sometimes we NEXT WEEK create so much noise it is hard to sleep. -
Flex Dates.Xlsx
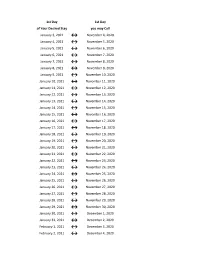
1st Day 1st Day of Your Desired Stay you may Call January 3, 2021 ↔ November 4, 2020 January 4, 2021 ↔ November 5, 2020 January 5, 2021 ↔ November 6, 2020 January 6, 2021 ↔ November 7, 2020 January 7, 2021 ↔ November 8, 2020 January 8, 2021 ↔ November 9, 2020 January 9, 2021 ↔ November 10, 2020 January 10, 2021 ↔ November 11, 2020 January 11, 2021 ↔ November 12, 2020 January 12, 2021 ↔ November 13, 2020 January 13, 2021 ↔ November 14, 2020 January 14, 2021 ↔ November 15, 2020 January 15, 2021 ↔ November 16, 2020 January 16, 2021 ↔ November 17, 2020 January 17, 2021 ↔ November 18, 2020 January 18, 2021 ↔ November 19, 2020 January 19, 2021 ↔ November 20, 2020 January 20, 2021 ↔ November 21, 2020 January 21, 2021 ↔ November 22, 2020 January 22, 2021 ↔ November 23, 2020 January 23, 2021 ↔ November 24, 2020 January 24, 2021 ↔ November 25, 2020 January 25, 2021 ↔ November 26, 2020 January 26, 2021 ↔ November 27, 2020 January 27, 2021 ↔ November 28, 2020 January 28, 2021 ↔ November 29, 2020 January 29, 2021 ↔ November 30, 2020 January 30, 2021 ↔ December 1, 2020 January 31, 2021 ↔ December 2, 2020 February 1, 2021 ↔ December 3, 2020 February 2, 2021 ↔ December 4, 2020 1st Day 1st Day of Your Desired Stay you may Call February 3, 2021 ↔ December 5, 2020 February 4, 2021 ↔ December 6, 2020 February 5, 2021 ↔ December 7, 2020 February 6, 2021 ↔ December 8, 2020 February 7, 2021 ↔ December 9, 2020 February 8, 2021 ↔ December 10, 2020 February 9, 2021 ↔ December 11, 2020 February 10, 2021 ↔ December 12, 2020 February 11, 2021 ↔ December 13, 2020 -

Julian Date Cheat Sheet for Regular Years
Date Code Cheat Sheet For Regular Years Day of Year Calendar Date 1 January 1 2 January 2 3 January 3 4 January 4 5 January 5 6 January 6 7 January 7 8 January 8 9 January 9 10 January 10 11 January 11 12 January 12 13 January 13 14 January 14 15 January 15 16 January 16 17 January 17 18 January 18 19 January 19 20 January 20 21 January 21 22 January 22 23 January 23 24 January 24 25 January 25 26 January 26 27 January 27 28 January 28 29 January 29 30 January 30 31 January 31 32 February 1 33 February 2 34 February 3 35 February 4 36 February 5 37 February 6 38 February 7 39 February 8 40 February 9 41 February 10 42 February 11 43 February 12 44 February 13 45 February 14 46 February 15 47 February 16 48 February 17 49 February 18 50 February 19 51 February 20 52 February 21 53 February 22 54 February 23 55 February 24 56 February 25 57 February 26 58 February 27 59 February 28 60 March 1 61 March 2 62 March 3 63 March 4 64 March 5 65 March 6 66 March 7 67 March 8 68 March 9 69 March 10 70 March 11 71 March 12 72 March 13 73 March 14 74 March 15 75 March 16 76 March 17 77 March 18 78 March 19 79 March 20 80 March 21 81 March 22 82 March 23 83 March 24 84 March 25 85 March 26 86 March 27 87 March 28 88 March 29 89 March 30 90 March 31 91 April 1 92 April 2 93 April 3 94 April 4 95 April 5 96 April 6 97 April 7 98 April 8 99 April 9 100 April 10 101 April 11 102 April 12 103 April 13 104 April 14 105 April 15 106 April 16 107 April 17 108 April 18 109 April 19 110 April 20 111 April 21 112 April 22 113 April 23 114 April 24 115 April -
2021 Bi-Weekly Paydates
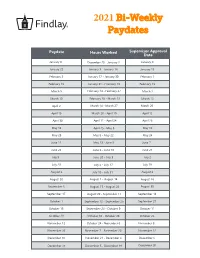
2021 Bi-Weekly Paydates Paydate Hours Worked Supervisor Approval Date January 8 December 20 - January 2 January 4 January 22 January 3 - January 16 January 15 February 5 January 17 - January 30 February 1 February 19 January 31 - February 13 February 15 March 5 February 14 - February 27 March 1 March 19 February 28 - March 13 March 15 April 2 March 14 - March 27 March 29 April 16 March 28 - April 10 April 12 April 30 April 11 - April 24 April 26 May 14 April 25 - May 8 May 10 May 28 May 9 - May 22 May 24 June 11 May 23 - June 5 June 7 June 25 June 6 - June 19 June 21 July 9 June 20 - July 3 July 2 July 23 July 4 - July 17 July 19 August 6 July 18 - July 31 August 2 August 20 August 1 - August 14 August 16 September 3 August 15 - August 28 August 30 September 17 August 29 - September 11 September 13 October 1 September 12 - September 25 September 27 October 15 September 26 - October 9 October 11 October 29 October 10 - October 23 October 25 November 12 October 24 - November 6 November 8 November 26 November 7 - November 20 November 22 December 10 November 21 - December 4 December 6 December 24 December 5 - December 18 December 20 2021 Bi-Weekly Paydate/Holiday Paydates January February March April Sun Mon Tues Wed Thurs Fri Sat Sun Mon Tues Wed Thurs Fri Sat Sun Mon Tues Wed Thurs Fri Sat Sun Mon Tues Wed Thurs Fri Sat 1 2 1 2 3 4 5 6 1 2 3 4 5 6 1 2 3 4 3 5 6 7 8 9 7 8 9 10 11 12 13 7 8 9 10 11 12 13 4 5 6 7 8 9 10 10 11 12 13 14 15 16 14 15 16 17 18 19 20 14 15 16 17 18 19 20 11 12 13 14 15 16 17 17 18 19 20 21 22 23 21 22 23 24 25 26 -

Pay Date Calendar
Pay Date Information Select the pay period start date that coincides with your first day of employment. Pay Period Pay Period Begins (Sunday) Pay Period Ends (Saturday) Official Pay Date (Thursday)* 1 January 10, 2016 January 23, 2016 February 4, 2016 2 January 24, 2016 February 6, 2016 February 18, 2016 3 February 7, 2016 February 20, 2016 March 3, 2016 4 February 21, 2016 March 5, 2016 March 17, 2016 5 March 6, 2016 March 19, 2016 March 31, 2016 6 March 20, 2016 April 2, 2016 April 14, 2016 7 April 3, 2016 April 16, 2016 April 28, 2016 8 April 17, 2016 April 30, 2016 May 12, 2016 9 May 1, 2016 May 14, 2016 May 26, 2016 10 May 15, 2016 May 28, 2016 June 9, 2016 11 May 29, 2016 June 11, 2016 June 23, 2016 12 June 12, 2016 June 25, 2016 July 7, 2016 13 June 26, 2016 July 9, 2016 July 21, 2016 14 July 10, 2016 July 23, 2016 August 4, 2016 15 July 24, 2016 August 6, 2016 August 18, 2016 16 August 7, 2016 August 20, 2016 September 1, 2016 17 August 21, 2016 September 3, 2016 September 15, 2016 18 September 4, 2016 September 17, 2016 September 29, 2016 19 September 18, 2016 October 1, 2016 October 13, 2016 20 October 2, 2016 October 15, 2016 October 27, 2016 21 October 16, 2016 October 29, 2016 November 10, 2016 22 October 30, 2016 November 12, 2016 November 24, 2016 23 November 13, 2016 November 26, 2016 December 8, 2016 24 November 27, 2016 December 10, 2016 December 22, 2016 25 December 11, 2016 December 24, 2016 January 5, 2017 26 December 25, 2016 January 7, 2017 January 19, 2017 1 January 8, 2017 January 21, 2017 February 2, 2017 2 January -

Due Date Chart 201803281304173331.Xlsx
Special Event Permit Application Due Date Chart for Events from January 1, 2019 - June 30, 2020 If due date lands on a Saturday or Sunday, the due date is moved to the next business day Event Date 30 Calendar days 90 Calendar Days Tuesday, January 01, 2019 Sunday, December 02, 2018 Wednesday, October 03, 2018 Wednesday, January 02, 2019 Monday, December 03, 2018 Thursday, October 04, 2018 Thursday, January 03, 2019 Tuesday, December 04, 2018 Friday, October 05, 2018 Friday, January 04, 2019 Wednesday, December 05, 2018 Saturday, October 06, 2018 Saturday, January 05, 2019 Thursday, December 06, 2018 Sunday, October 07, 2018 Sunday, January 06, 2019 Friday, December 07, 2018 Monday, October 08, 2018 Monday, January 07, 2019 Saturday, December 08, 2018 Tuesday, October 09, 2018 Tuesday, January 08, 2019 Sunday, December 09, 2018 Wednesday, October 10, 2018 Wednesday, January 09, 2019 Monday, December 10, 2018 Thursday, October 11, 2018 Thursday, January 10, 2019 Tuesday, December 11, 2018 Friday, October 12, 2018 Friday, January 11, 2019 Wednesday, December 12, 2018 Saturday, October 13, 2018 Saturday, January 12, 2019 Thursday, December 13, 2018 Sunday, October 14, 2018 Sunday, January 13, 2019 Friday, December 14, 2018 Monday, October 15, 2018 Monday, January 14, 2019 Saturday, December 15, 2018 Tuesday, October 16, 2018 2019 Tuesday, January 15, 2019 Sunday, December 16, 2018 Wednesday, October 17, 2018 Wednesday, January 16, 2019 Monday, December 17, 2018 Thursday, October 18, 2018 Thursday, January 17, 2019 Tuesday, December 18, 2018 -

Academic Calendar – Spring 2021 16-Week Courses (January 19-May 20) Faculty Development Days January 13-15 Canvas Course Site Opens January 15 Martin Luther King, Jr
Academic Calendar – Spring 2021 16-week courses (January 19-May 20) Faculty Development Days January 13-15 Canvas Course Site Opens January 15 Martin Luther King, Jr. Day (College Closed) January 18 Classes Begin January 19 Open Registration Ends January 20 Presidents’ Day (College Closed) February 15 College Development Day (No Classes) February 16 Midterm Grades Due 10:00 AM March 12 Spring Break (No Classes) March 14-21 Spring Break (College Closed) March 19-21 College Development Day (No Classes) April 1 Spring Holiday (College Closed) April 2 Summer/Fall Registration Begins April 20 Last Day to Drop/Withdraw May 7 Last Day of Instruction May 14 Final Assessments May 15-20 Commencement May 20 Final Grades Due@ 10:00 AM May 24 1st 8-week courses (January 19-March 13) Faculty Development Days January 13-15 Canvas Course Site Opens January 15 Martin Luther King, Jr. Day (College Closed) January 18 Classes Begin January 19 Open Registration Ends January 20 Midterm Grades Due 10:00AM February 12 Presidents’ Day (College Closed) February 15 College Development Day (No Classes) February 16 Last Day to Drop/Withdraw March 5 Final Assessments Last Day of Classes End of Classes March 13 Final Grades Due@ 10:00 AM March 22 14-week courses (February 1-May 15) Canvas Course Site Opens January 29 Classes Begin February 1 Open Registration Ends February 2 Presidents’ Day (College Closed) February 15 College Development Day (No Classes) February 16 Midterm Grades Due 10:00 AM March 12 Spring Break (No Classes) March 14-21 Spring Break(College Closed) -

2022 7 Day Working Days Calendar
2022 7 Day Working Days Calendar The Working Day Calendar is used to compute the estimated completion date of a contract. To use the calendar, find the start date of the contract, add the working days to the number of the calendar date (a number from 1 to 1000), and subtract 1, find that calculated number in the calendar and that will be the completion date of the contract Date Number of the Calendar Date Saturday, January 1, 2022 498 Sunday, January 2, 2022 499 Monday, January 3, 2022 500 Tuesday, January 4, 2022 501 Wednesday, January 5, 2022 502 Thursday, January 6, 2022 503 Friday, January 7, 2022 504 Saturday, January 8, 2022 505 Sunday, January 9, 2022 506 Monday, January 10, 2022 507 Tuesday, January 11, 2022 508 Wednesday, January 12, 2022 509 Thursday, January 13, 2022 510 Friday, January 14, 2022 511 Saturday, January 15, 2022 512 Sunday, January 16, 2022 513 Monday, January 17, 2022 514 Tuesday, January 18, 2022 515 Wednesday, January 19, 2022 516 Thursday, January 20, 2022 517 Friday, January 21, 2022 518 Saturday, January 22, 2022 519 Sunday, January 23, 2022 520 Monday, January 24, 2022 521 Tuesday, January 25, 2022 522 Wednesday, January 26, 2022 523 Thursday, January 27, 2022 524 Friday, January 28, 2022 525 Saturday, January 29, 2022 526 Sunday, January 30, 2022 527 Monday, January 31, 2022 528 Tuesday, February 1, 2022 529 Wednesday, February 2, 2022 530 Thursday, February 3, 2022 531 Friday, February 4, 2022 532 Date Number of the Calendar Date Saturday, February 5, 2022 533 Sunday, February 6, 2022 534 Monday, February -

Date of Close Contact Exposure
Date of Close Contact Exposure 7 days 10 days 14 days Monday, November 16, 2020 Tuesday, November 24, 2020 Friday, November 27, 2020 Tuesday, December 1, 2020 Tuesday, November 17, 2020 Wednesday, November 25, 2020 Saturday, November 28, 2020 Wednesday, December 2, 2020 Wednesday, November 18, 2020 Thursday, November 26, 2020 Sunday, November 29, 2020 Thursday, December 3, 2020 Thursday, November 19, 2020 Friday, November 27, 2020 Monday, November 30, 2020 Friday, December 4, 2020 Friday, November 20, 2020 Saturday, November 28, 2020 Tuesday, December 1, 2020 Saturday, December 5, 2020 Saturday, November 21, 2020 Sunday, November 29, 2020 Wednesday, December 2, 2020 Sunday, December 6, 2020 Sunday, November 22, 2020 Monday, November 30, 2020 Thursday, December 3, 2020 Monday, December 7, 2020 Monday, November 23, 2020 Tuesday, December 1, 2020 Friday, December 4, 2020 Tuesday, December 8, 2020 Tuesday, November 24, 2020 Wednesday, December 2, 2020 Saturday, December 5, 2020 Wednesday, December 9, 2020 Wednesday, November 25, 2020 Thursday, December 3, 2020 Sunday, December 6, 2020 Thursday, December 10, 2020 Thursday, November 26, 2020 Friday, December 4, 2020 Monday, December 7, 2020 Friday, December 11, 2020 Friday, November 27, 2020 Saturday, December 5, 2020 Tuesday, December 8, 2020 Saturday, December 12, 2020 Saturday, November 28, 2020 Sunday, December 6, 2020 Wednesday, December 9, 2020 Sunday, December 13, 2020 Sunday, November 29, 2020 Monday, December 7, 2020 Thursday, December 10, 2020 Monday, December 14, 2020 Monday, November -

2021 Working Day Calendar-5 Day-Alternative Format
2021 Working Days Calendar – 5 day The Working Day Calendar is used to compute the estimated completion date of a contract. To use the calendar, find the start date of the contract, add the working days to the number of the calendar date (a number from 1 to 1000), and subtract 1, find that calculated number in the calendar and that will be the completion date of the contract Date Number of the Calendar Date Friday, January 1, 2021 Non-working Day Saturday, January 2, 2021 Non-working Day Sunday, January 3, 2021 Non-working Day Monday, January 4, 2021 938 Tuesday, January 5, 2021 939 Wednesday, January 6, 2021 940 Thursday, January 7, 2021 941 Friday, January 8, 2021 942 Saturday, January 9, 2021 Non-working Day Sunday, January 10, 2021 Non-working Day Monday, January 11, 2021 943 Tuesday, January 12, 2021 944 Wednesday, January 13, 2021 945 Thursday, January 14, 2021 946 Friday, January 15, 2021 947 Saturday, January 16, 2021 Non-working Day Sunday, January 17, 2021 Non-working Day Monday, January 18, 2021 Non-working Day Tuesday, January 19, 2021 948 Wednesday, January 20, 2021 949 Thursday, January 21, 2021 950 Friday, January 22, 2021 951 Saturday, January 23, 2021 Non-working Day Sunday, January 24, 2021 Non-working Day Monday, January 25, 2021 952 Tuesday, January 26, 2021 953 Wednesday, January 27, 2021 954 Thursday, January 28, 2021 955 Friday, January 29, 2021 956 Saturday, January 30, 2021 Non-working Day Sunday, January 31, 2021 Non-working Day Monday, February 1, 2021 957 Tuesday, February 2, 2021 958 Wednesday, February 3, -
2 3 2 2 2 2 2 2 2 2 2 2 2 3 2 3 2 2 2 2 3 2 2 2 2 3 2 2 2 2 2015
2015-16 ALIEF INDEPENDENT SCHOOL DISTRICT Pay Dates and Cut-Off Dates For Hourly, Substitute and Supplemental Pay Supp/Timesheet Paydate Cut Off Period Covered Weeks due 2015 Monday, June 15 May 15 May 2 – May 15 2 May 20 Tuesday, June 30 June 5 May 16 – June 5 3 June 10 Wednesday, July 15 June 19 June 6 – June 19 2 June 24 Thursday, July 30 July 3 June 20 – July 3 2 July 8 Friday, August 14 July 17 July 4 - July 17 2 July 22 Monday, August 31 July 31 July 18 - July 31 2 August 5 Tuesday, September 15 August 14 August 1 – August 14 2 August 19 Wednesday, September 30 August 28 August 15 – August 28 2 September 2 Thursday, October 15 September 11 August 29 – September 11 2 September 16 Friday, October 30 September 25 September 12 – September 25 2 September 30 Friday, November 13 October 9 September 26 – October 9 2 October 14 Friday, November 20 October 23 October 10 – October 23 2 October 28 Tuesday, December 15 November 6 October 24 – November 6 2 November 11 Friday, December 18 November 27 November 7 – November 27 3 December 2 2016 Friday, January 15 December 11 November 28 – December 11 2 December 16 Friday, January 29 January 1 December 12 – January 1 3 January 6 Friday, February 12 January 15 January 2 – January 15 2 January 20 Monday, February 29 January 29 January 16 – January 29 2 February 3 Friday, March 11 February 12 January 30 – February 12 2 February 17 Thursday, March 31 February 26 February 13 – February 26 2 March 2 Friday, April 15 March 18 February 27 – March 18 3 March 23 Friday, April 29 April 1 March 19 – April 1 2 April 6 Friday, May 13 April 15 April 2 – April 15 2 April 20 Tuesday, May 31 29-Apr April 16 – April 29 2 May 4 Wednesday, June 15 May 13 April 30 – May 13 2 May 18 Thursday, June 30 June 3 May 14 – June 3 3 June 8 Thursday, July 14 June 17 June 4 – June 17 2 June 22 Thursday, July 28 July 1 June 18 – July 1 2 July 6 Monday, August 15 July 15 July 2 - July 15 2 July 20 Wednesday, August 31 July 29 July 16 - July 29 2 August 3 .