Findings of Inquest Into the Death of Julian Werner Wlodarczyk 1
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Environmental Officer
View metadata, citation and similar papers at core.ac.uk brought to you by CORE provided by GBRMPA eLibrary Sunfish Queensland Inc Freshwater Wetlands and Fish Importance of Freshwater Wetlands to Marine Fisheries Resources in the Great Barrier Reef Vern Veitch Bill Sawynok Report No: SQ200401 Freshwater Wetlands and Fish 1 Freshwater Wetlands and Fish Importance of Freshwater Wetlands to Marine Fisheries Resources in the Great Barrier Reef Vern Veitch1 and Bill Sawynok2 Sunfish Queensland Inc 1 Sunfish Queensland Inc 4 Stagpole Street West End Qld 4810 2 Infofish Services PO Box 9793 Frenchville Qld 4701 Published JANUARY 2005 Cover photographs: Two views of the same Gavial Creek lagoon at Rockhampton showing the extreme natural variability in wetlands depending on the weather. Information in this publication is provided as general advice only. For application to specific circumstances, professional advice should be sought. Sunfish Queensland Inc has taken all steps to ensure the information contained in this publication is accurate at the time of publication. Readers should ensure that they make the appropriate enquiries to determine whether new information is available on a particular subject matter. Report No: SQ200401 ISBN 1 876945 42 7 ¤ Great Barrier Reef Marine Park Authority and Sunfish Queensland All rights reserved. No part of this publication may be reprinted, reproduced, stored in a retrieval system or transmitted, in any form or by any means, without prior permission from the Great Barrier Reef Marine Park Authority. Freshwater Wetlands and Fish 2 Table of Contents 1. Acronyms Used in the Report .......................................................................8 2. Definition of Terms Used in the Report.........................................................9 3. -

Burnett Mary WQIP Ecologically Relevant Targets
Ecologically relevant targets for pollutant discharge from the drainage basins of the Burnett Mary Region, Great Barrier Reef TropWATER Report 14/32 Jon Brodie and Stephen Lewis 1 Ecologically relevant targets for pollutant discharge from the drainage basins of the Burnett Mary Region, Great Barrier Reef TropWATER Report 14/32 Prepared by Jon Brodie and Stephen Lewis Centre for Tropical Water & Aquatic Ecosystem Research (TropWATER) James Cook University Townsville Phone : (07) 4781 4262 Email: [email protected] Web: www.jcu.edu.au/tropwater/ 2 Information should be cited as: Brodie J., Lewis S. (2014) Ecologically relevant targets for pollutant discharge from the drainage basins of the Burnett Mary Region, Great Barrier Reef. TropWATER Report No. 14/32, Centre for Tropical Water & Aquatic Ecosystem Research (TropWATER), James Cook University, Townsville, 41 pp. For further information contact: Catchment to Reef Research Group/Jon Brodie and Steven Lewis Centre for Tropical Water & Aquatic Ecosystem Research (TropWATER) James Cook University ATSIP Building Townsville, QLD 4811 [email protected] © James Cook University, 2014. Except as permitted by the Copyright Act 1968, no part of the work may in any form or by any electronic, mechanical, photocopying, recording, or any other means be reproduced, stored in a retrieval system or be broadcast or transmitted without the prior written permission of TropWATER. The information contained herein is subject to change without notice. The copyright owner shall not be liable for technical or other errors or omissions contained herein. The reader/user accepts all risks and responsibility for losses, damages, costs and other consequences resulting directly or indirectly from using this information. -

The Freshwater Crayfish (Family Parastacidae) of Queensland
AUSTRALIAN MUSEUM SCIENTIFIC PUBLICATIONS Riek, E. F., 1951. The freshwater crayfish (family Parastacidae) of Queensland. Records of the Australian Museum 22(4): 368–388. [30 June 1951]. doi:10.3853/j.0067-1975.22.1951.615 ISSN 0067-1975 Published by the Australian Museum, Sydney nature culture discover Australian Museum science is freely accessible online at http://publications.australianmuseum.net.au 6 College Street, Sydney NSW 2010, Australia 11ft! FRESHWATER CRAYFISH (FAMILY PARASTACIDAE) OF QUEENSLAND WITH AN ApPENDIX DESORIBING OTHlm AV5'lHALIAN SPEClEf'. By E. F. HIEK. (;ommonwealth Scientific and Industrial l~csearch Organization - Divhdon of Entomology, Canberra, A.C.T. (Figures 1-13.) Freshwater crayfish occur in almost every body of fresh water from artificial damfl and natural billabongs (I>tanding water) to headwater creeks and large rivers (flowing water). Generally the species are of considerable size and therefore easily collected, but even so many of the larger forms are unknown scientifically. This paper deals with all the species that have been collected from Queensland. It also includes a few species from New South Wales and other States. No doubt additional species will be found and some of the mOre variable series, at present included under the one specific namc, will be further subdivided. From Queensland nine species are described as new, making a total of seventeen species (of three genera) recorded from that State. The type localities of all but two of these species are in Queensland but some are not restricted to the State. Clark's 1936 and subsequent papers have been used as the basis for further taxonomic studies of the Australian freshwater crayfish. -

12 Days the Great Tropical Drive
ITINERARY The Great Tropical Drive Queensland – Cairns Cairns – Cooktown – Mareeba – Undara – Charters Towers – Townsville – Ingham – Tully/Mission Beach – Innisfail – Cairns Drive from Cairns to Townsville, through World Heritage-listed reef and rainforests to golden outback savannah. On this journey you won’t miss an inch of Queensland’s tropical splendour. AT A GLANCE Cruise the Great Barrier Reef and trek the ancient Daintree Rainforest. Connect with Aboriginal culture as you travel north to the remote frontier of Cape Tribulation. Explore historic gold mining towns and the lush orchards and plantations of the Tropical Tablelands. Day trip to Magnetic, Dunk and Hinchinbrook Islands and relax in resort towns like Port Douglas and Mission Beach. This journey has a short 4WD section, with an alternative road for conventional vehicles. > Cairns – Port Douglas (1 hour) > Port Douglas – Cooktown (3 hours) > Cooktown – Mareeba (4.5 hours) DAY ONE > Mareeba – Ravenshoe (1 hour) > Ravenshoe – Undara Volcanic Beach. Continue along the Cook Highway, CAIRNS TO PORT DOUGLAS National Park (2.5 hours) Meander along the golden chain of stopping at Rex Lookout for magical views over the Coral Sea beaches. Drive into the > Undara Volcanic National Park – beaches stretching north from Cairns. Surf Charters Towers (5.5 hours) at Machans Beach and swim at Holloways sophisticated tropical oasis Port Douglas, and palm-fringed Yorkey’s Knob. Picnic which sits between World Heritage-listed > Charters Towers – Townsville (1.5 hours) beneath sea almond trees in Trinity rainforest and reef. Walk along the white Beach or lunch in the tropical village. sands of Four Mile Beach and climb > Townsville – Ingham (1.5 hours) Flagstaff Hill for striking views over Port Hang out with the locals on secluded > Ingham – Cardwell (0.5 hours) Douglas. -

With Its Unique Location Deep Within the Magnificent Daintree Rainforest, There’S an Abundance of Things to Do Both in and Around the Daintree Ecolodge
With its unique location deep within the magnificent Daintree Rainforest, there’s an abundance of things to do both in and around the Daintree Ecolodge. The region has some beautiful landmarks that are a must see during your time in the region. We have listed the top places to visit and experience to ensure you get the most out of your stay. Explore the beauty of the Daintree Rainforest on a guided ‘A Walk Through Time’ rainforest walk on the grounds of the Daintree Ecolodge. On a leisurely 1.5 hour stroll through the enchanted rainforest, discover the lodge’s private onsite waterfall. The waterfall and swimming hole is sacred to the Kuku Yalanji women who for thousands of years have bathed in its crystal-clear waters for healing and spiritual beliefs. Learn about the unique and amazing plants, insects, birds and other wildlife that surround us. Much of the wildlife you will see here cannot be found anywhere else in the world, with some species dating back 135 million years. The local Kuku Yalanji people have named the land on which the Daintree Ecolodge sits ‘Wawu-karrba’ which means ‘healing of the spirit.’ With approval from the local Indigenous tribe elders, each of the Daintree Wellness Spa treatments combine the wisdom of their culture, healing, medicines and spirituality. Using the pure waters of the pristine onsite waterfall and the powerful properties of nourishing botanical products, many found in the Daintree Rainforest, guests can experience a renewed sense of wellbeing with each unique treatment. The treatment rooms are open roofed opening up to the rainforest canopy above and the sounds and smells of the wilderness. -
Daintree Catchment
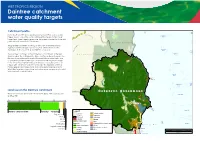
WET TROPICS REGION Daintree catchment water quality targets r e v Catchment profile i Ruby R n Reef a st n Under the Reef 2050 Water Quality Improvement Plan, water quality E a Norm n a A Endeavour nby R Reef i targets have been set for each catchment that drains to the Great v e Barrier Reef. These targets (given over the page) consider land use and r pollutant loads from each catchment. E n d e a v o u r C a t c h m e n t r 2 Rive The Daintree catchment covers 2107 km (10% of the Wet Tropics y b an m region). Rainfall averages 2521 mm a year, which results in river r o N Pickersgill discharges to the coast of about 2887 GL each year. st e Reef Escape W Reef Weary Evening The Daintree catchment is the northernmost catchment in the Wet N o r m a n b y C a t c h m e n t Bay Reef Tropics region. The catchment is divided by two major waterways, the Daintree River in the south and the Bloomfield River in the north, and a number of smaller waterways that flow from the mountain ranges to the coast. The majority of the catchment is covered by mountain Morning Reef ranges with a narrow lowland coastal plain. The highland section is mostly reserved for conservation and is included in the Wet Tropics World Heritage Area. Agriculture and urban areas are primarily located in the lowland coastal section. Mackay Reef Cape Tribulation . -

Cyclone Sadie Flood Plumes in the Great Barrier Reef Lagoon: Composition and Consequences
WORKSHOP SERIES No 22 Cyclone Sadie Flood Plumes in the Great Barrier Reef Lagoon: Composition and Consequences Proceedings of a workshop held in Townsville Queensland, Australia, 10 November 1994, at the Australian Institute of Marine Science. Edited by Andrew Steven GREAT BARRIERREEF MARINEPARKAUTHORMY 0 Great Barrier Reef Marine Park Authority 1997 ISSN 0156 5842 ISBN 0 642 23014 5 Published February 1997 by the Great Barrier Reef Marine Park Authority The opinions expressed in this document are not necessarily those of the Great Barrier Reef Marine Park Authority. National Library of Australia Cataloguing-in-Publication data: Cyclone Sadie flood plumes in the Great Barrier Reef Lagoon : composition and consequences: proceedings of a workshop held in Townsville, Queensland, Australia, 10 November 1994, at the Australian Institute of Marine Science. Bibliography.’ ISBN 0 642 23014 5. 1. Sediment transport - Queensland - Great Barrier Reef - Congresses. 2. Reef ecology - Queensland - Great Barrier Reef - Congresses. 3. Great Barrier Reef (Qld.) - Congresses. I. Steven, A. D. L. (Andrew David Leslie), 1962 - II. Great Barrier Reef Marine Park Authority (Australia). (Series : Workshop series (Great Barrier Reef Marine Park Authority (Australia)) ; no. 22). 574.52636709943 COVER PHOTOGRAPH Maria Creek, Kurramine in flood, 2 February 1994 Photograph by Andrew Elliott Great Barrier Reef Marine Park Authority GREATBARRIERREEF MARmEPARKAuTH0RITY PO Box 1379 Townsville Qld 4810 Telephone (077) 500 700 I Table of Contents Preface Workshop Program Contributed Papers Nutrients and suspended sediment discharge from the Johnstone River catchment during cyclone Sadie HM Hunter .. : . ............................................................. 1 Export of nutrients and suspended sediment from the Herbert River catchment during a flood event associated with cyclone Sadie AW Mitchell and RGV Bramley . -
Flood Risk Management in Australia Building Flood Resilience in a Changing Climate
Flood Risk Management in Australia Building flood resilience in a changing climate December 2020 Flood Risk Management in Australia Building flood resilience in a changing climate Neil Dufty, Molino Stewart Pty Ltd Andrew Dyer, IAG Maryam Golnaraghi (lead investigator of the flood risk management report series and coordinating author), The Geneva Association Flood Risk Management in Australia 1 The Geneva Association The Geneva Association was created in 1973 and is the only global association of insurance companies; our members are insurance and reinsurance Chief Executive Officers (CEOs). Based on rigorous research conducted in collaboration with our members, academic institutions and multilateral organisations, our mission is to identify and investigate key trends that are likely to shape or impact the insurance industry in the future, highlighting what is at stake for the industry; develop recommendations for the industry and for policymakers; provide a platform to our members, policymakers, academics, multilateral and non-governmental organisations to discuss these trends and recommendations; reach out to global opinion leaders and influential organisations to highlight the positive contributions of insurance to better understanding risks and to building resilient and prosperous economies and societies, and thus a more sustainable world. The Geneva Association—International Association for the Study of Insurance Economics Talstrasse 70, CH-8001 Zurich Email: [email protected] | Tel: +41 44 200 49 00 | Fax: +41 44 200 49 99 Photo credits: Cover page—Markus Gebauer / Shutterstock.com December 2020 Flood Risk Management in Australia © The Geneva Association Published by The Geneva Association—International Association for the Study of Insurance Economics, Zurich. 2 www.genevaassociation.org Contents 1. -

Daintreep Daintreepedia
Generously Sponsored by Daintreep June 2019 Daintreepedia Table of Contents Community Facilities.........................................................................................................................................3 Ferry..................................................................................................................................................................5 Distances – driving (approx.)............................................................................................................................7 Dining Out / Groceries / Picnic Areas...............................................................................................................8 Tours & Activities............................................................................................................................................11 Walks...............................................................................................................................................................16 Swimming........................................................................................................................................................17 Arts & Crafts....................................................................................................................................................18 Special Needs.................................................................................................................................................19 Accommodation..............................................................................................................................................22 -

For the Daintree River
BRIDGE OR FERRY FOR THE DAINTREE RIVER Douglas Shire Council received 61 submissions. This document is a compilation of all those submissions in their entirety, with the exception of removing content which identified contributors. The exception being those organisations and community groups who requested their submission be published under the organisation’s banner. For ease of readability, submissions have been grouped under the following headings: ▪ Preference for a two-ferry service Page 2 ▪ Preference for Single Ferry Page 38 ▪ No Clear Preference as to Single or Two Ferries Page 70 ▪ Preference for a bridge Page 74 ▪ No Preference Specified Page 99 Enquiries Gaye Scott [email protected] Published 1 December 2020 Comments Received Preference for a two-ferry service Ferry adds to the specialness and mystery I would like to ask the Council to drop the idea of a bridge across the Daintree River. I believe building a bridge would be killing the goose that laid the golden egg. The whole cache of the Daintree is that it is part of it is pristine rainforest. Reaching this area by ferry adds to the specialness and mystery. Protecting this area has been a hard won fight since the blockade. I think the fact that Douglas is considered one of the world’s top tourist destinations shows that preserving the Daintree was an important step in achieving this accomplishment. If it works - don’t fix it. Visitors love it the way it is. Another ferry is a much better solution to the issue of long waits during peak times. A bridge will destroy what is attracting people in the first place. -

Upper Mitchell Catchment Rehabilitation Plan
Upper Mitchell Catchment Rehabilitation Plan Technical Report on Rehabilitation Needs A report prepared by the NQ Afforestation Association Inc. to facilitate coordinated catchment rehabilitation in the Upper Mitchell Catchment NQ AFFORESTATION Upper Mitchell River Catchment Rehabilitation Plan Technical Report Draft The North Queensland Afforestation Association Inc. is a regional Local Government body made up of 10 member councils - Cook Shire, Douglas Shire, Cairns City, Mareeba Shire, Atherton Shire, Herberton Shire, Eacham Shire, Johnstone Shire, Cardwell Shire and Hinchinbrook Shire. The North Queensland Afforestation Association Inc. is committed to fostering sustainable resource management in the wet tropics region through initiatives such as the Wet Tropics Tree Planting Scheme and the Community Rainforest Reforestation Program. This report is one of a series produced by the North Queensland Afforestation Association Inc. to identify rehabilitation priorities across the wet tropics and provide input to Local Authority planning schemes. Comments and questions regarding the materials in this report should be directed to Kylie Freebody at the North Queensland Afforestation Association Inc. office in Cairns: 28 Scott Street Cairns Q 4870 PO Box 2420, Cairns Q 4870 Phone: (070) 412 593 Fax: (070) 412 598 The North Queensland Afforestation Association Inc. wishes to acknowledge the contributions of the following organisations: Mareeba Shire Council Department of Natural Resources Cattle Creek Landcare Group Department of Environment -

5.8 Daintree River Crossing Round Two Public Consultation Plan
161 of 215 5.8. DAINTREE RIVER CROSSING ROUND TWO PUBLIC CONSULTATION PLAN REPORT AUTHOR Gaye Scott, Community Liaison Officer MANAGER Pieter Kleinhans, Acting Manager Infrastructure DEPARTMENT Infrastructure RECOMMENDATION That Council: endorses the community public consultation plan for the Daintree River Ferry Crossing; and delegates authority under section 257 of the Local Government Act 2009 to the Chief Executive Officer to finalise all matters associated with this plan. EXECUTIVE SUMMARY The Daintree River Crossing Options Assessment Report examines a bridge option and the proposed two-ferry service, includes costs and provides a comparison against the current single ferry arrangement. This report will be released publicly, and the community will be invited to provide feedback on the different options examined, and, if they have one, their preferred Daintree River Crossing option. Attached to this report is the public consultation plan developed for this purpose and it is presented to Council for endorsement. BACKGROUND The current Daintree ferry contract is due to expire 30 June 2021 and following a tender process, in December 2019, Douglas Shire Council resolved to commence contractual negotiations with local company, Sirron Enterprises Pty Ltd which proposed a two-ferry service. In April 2020, via a Mayoral Minute, Council resolved to temporarily suspend the Daintree River Ferry contract negotiations and do a second round of community consultation to include a bridge option. The initial round of consultation was focussed on what the community wanted by way of an enhanced ferry service, and the feedback received was used to prepare tender specifications for a ferry service. It did not include information about the costs involved in either operating a second ferry or building a bridge.