Womb Health = World Health
Total Page:16
File Type:pdf, Size:1020Kb

Load more
Recommended publications
-

The Evidence on Waterbirth What Is Water Birth?
Evidence on the Safety of Water Birth What is Evidence Based Care? Get your 3 free lessons here! Your Name Your Email I want this! We respect your email privacy Evidence on the Safety of Water Birth The Evidence on Waterbirth Popular Recent In April 2014, waterbirth—an alternative method for pain relief in which a mother gives birth Evidence Based in a tub of warm water—made national headlines. The event that pushed water birth safety Birth Class on into the spotlight was a joint Opinion Statement from the American Congress of Obstetricians Suspected Big Babies and Gynecologists (ACOG) and the American Academy of Pediatrics (AAP), denouncing the September 24th, 2013 practice. In their opinion statement, ACOG and the AAP firmly admonished that waterbirth should Group B Strep in be considered an experimental practice that should only occur in the context of a clinical Pregnancy: Evidence research study. Their conclusion, which echoed a previous AAP Opinion Statement from for Antibiotics and 2005, was based on their opinion that water birth does not have any benefits and may pose Alternatives dangers for the newborn. April 9th, 2013 In response, the American College of Nurse Midwives (ACNM),(Midwives 2014) the American What is the Evidence Association of Birth Centers (AABC), and the Royal College of Midwives (RCM) all released for Induction or C- statements endorsing waterbirth as a safe, evidence-based option. Meanwhile, the AABC section for a Big released preliminary data from nearly 4,000 waterbirths that occurred in birth centers all over Baby? the U.S., supporting water birth as safe for mothers and infants. -

Alcohol, Breastfeeding, and Development at 18 Months
Alcohol, Breastfeeding, and Development at 18 Months Ruth E. Little, ScD*; Kate Northstone, MSc‡; Jean Golding, PhD, ScD‡; and the ALSPAC Study Team‡ ABSTRACT. Objective. We aimed to replicate a pre- literature search, we found only 1 systematic study1 vious study of 1-year-olds that reported a deficit in motor that measured drinking during lactation and subse- development associated with moderate alcohol use dur- quent child development. The authors reported a ing lactation, using a different but comparable popula- decrease in the motor development of infants at 1 tion. year of age, as measured by the Bayley Scales,2 when Methodology. The mental development of 915 18- the lactating mother had as little as 1 drink daily in month-old toddlers from a random sample of a longitu- dinal population-based study in the United Kingdom the first 3 months after delivery. This result was was measured using the Griffiths Developmental Scales. independent of drinking during pregnancy. Frequent self-administered questionnaires during and Lactation is the preferred method of early infant after pregnancy provided maternal data. The dose of feeding, and drinking alcohol is a common social alcohol available to the lactating infant was obtained by custom in most of the western world. Knowing the multiplying the alcohol intake of the mother by the pro- effect on the infant when lactation and alcohol drink- portion of breast milk in the infant’s diet. We compared ing are combined is of high importance, especially in this dose with the Griffiths Scales of Mental Develop- view of the previous report of its adverse effects. -

The Polarity Therapy Paradigm Regarding Pre-Conception, Prenatal and Birth Imprinting
The Polarity Therapy Paradigm Regarding Pre-Conception, Prenatal and Birth Imprinting Raymond Castellino, D.C., , R.C.S.T., R.P.P. Winner of the first annual Dr. Randolph Stone Prize for the best research paper on Polarity Therapy. Presented to the American Polarity Therapy Association Ann Arbor, Michigan June, 1995 Castellino Prenatal and Birth Therapy Training Santa Barbara, California ©Copyright August 1995, revised March 1996. Available from Raymond Castellino, D.C., R.P.P., 1105 N. Ontare, Santa 1 Barbara, CA 93105, (805) 687-2897. This document may not be reproduced for any reason. The Polarity Therapy Paradigm1, 2 Regarding Pre-Conception, Prenatal and Birth Imprinting by Raymond Castellino, D.C., R.P.P. Abstract: This article provides an overview of Dr. Randolph Stone’s Polarity paradigm (energy concept) and explores its application to the transition of a baby’s consciousness and experience of pre-conception, conception, gestation and birth. Baby Angelika's case- history is presented to illustrate how application of the Polarity paradigm can support individuals (especially babies) to heal prenatal and birth trauma. The paradigm is presented as a bridge to understanding the effects of trauma on the emerging being and suggests how a new approach to healing trauma in babies is consistent with Dr. Stone's energy concept. Special attention is given to the three gunas and to triad relationships as a conceptual model for healing prenatal and birth trauma. A call for further research is made. The conclusion suggests that: 1. A global paradigm shift from technological and biochemically dominant practices to energy medicine that focuses on human understanding, compassion, contact and love is already in progress; 2. -

A Guide to Obstetrical Coding Production of This Document Is Made Possible by Financial Contributions from Health Canada and Provincial and Territorial Governments
ICD-10-CA | CCI A Guide to Obstetrical Coding Production of this document is made possible by financial contributions from Health Canada and provincial and territorial governments. The views expressed herein do not necessarily represent the views of Health Canada or any provincial or territorial government. Unless otherwise indicated, this product uses data provided by Canada’s provinces and territories. All rights reserved. The contents of this publication may be reproduced unaltered, in whole or in part and by any means, solely for non-commercial purposes, provided that the Canadian Institute for Health Information is properly and fully acknowledged as the copyright owner. Any reproduction or use of this publication or its contents for any commercial purpose requires the prior written authorization of the Canadian Institute for Health Information. Reproduction or use that suggests endorsement by, or affiliation with, the Canadian Institute for Health Information is prohibited. For permission or information, please contact CIHI: Canadian Institute for Health Information 495 Richmond Road, Suite 600 Ottawa, Ontario K2A 4H6 Phone: 613-241-7860 Fax: 613-241-8120 www.cihi.ca [email protected] © 2018 Canadian Institute for Health Information Cette publication est aussi disponible en français sous le titre Guide de codification des données en obstétrique. Table of contents About CIHI ................................................................................................................................. 6 Chapter 1: Introduction .............................................................................................................. -
Turning Your Breech Baby to a Head-Down Position (External Cephalic Version)
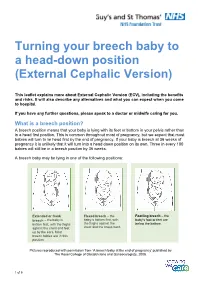
Turning your breech baby to a head-down position (External Cephalic Version) This leaflet explains more about External Cephalic Version (ECV), including the benefits and risks. It will also describe any alternatives and what you can expect when you come to hospital. If you have any further questions, please speak to a doctor or midwife caring for you. What is a breech position? A breech position means that your baby is lying with its feet or bottom in your pelvis rather than in a head first position. This is common throughout most of pregnancy, but we expect that most babies will turn to lie head first by the end of pregnancy. If your baby is breech at 36 weeks of pregnancy it is unlikely that it will turn into a head down position on its own. Three in every 100 babies will still be in a breech position by 36 weeks. A breech baby may be lying in one of the following positions: Extended or frank Flexed breech – the Footling breech – the breech – the baby is baby is bottom first, with baby’s foot or feet are bottom first, with the thighs the thighs against the below the bottom. against the chest and feet chest and the knees bent. up by the ears. Most breech babies are in this position. Pictures reproduced with permission from ‘A breech baby at the end of pregnancy’ published by The Royal College of Obstetricians and Gynaecologists, 2008. 1 of 5 What causes breech? Breech is more common in women who are expecting twins, or in women who have a differently-shaped womb (uterus). -

Dermatology and Pregnancy* Dermatologia E Gestação*
RevistaN2V80.qxd 06.05.05 11:56 Page 179 179 Artigo de Revisão Dermatologia e gestação* Dermatology and pregnancy* Gilvan Ferreira Alves1 Lucas Souza Carmo Nogueira2 Tatiana Cristina Nogueira Varella3 Resumo: Neste estudo conduz-se uma revisão bibliográfica da literatura sobre dermatologia e gravidez abrangendo o período de 1962 a 2003. O banco de dados do Medline foi consul- tado com referência ao mesmo período. Não se incluiu a colestase intra-hepática da gravidez por não ser ela uma dermatose primária; contudo deve ser feito o diagnóstico diferencial entre suas manifestações na pele e as dermatoses específicas da gravidez. Este apanhado engloba as características clínicas e o prognóstico das alterações fisiológicas da pele durante a gravidez, as dermatoses influenciadas pela gravidez e as dermatoses específi- cas da gravidez. Ao final apresenta-se uma discussão sobre drogas e gravidez Palavras-chave: Dermatologia; Gravidez; Patologia. Abstract: This study is a literature review on dermatology and pregnancy from 1962 to 2003, based on Medline database search. Intrahepatic cholestasis of pregnancy was not included because it is not a primary dermatosis; however, its secondary skin lesions must be differentiated from specific dermatoses of pregnancy. This overview comprises clinical features and prognosis of the physiologic skin changes that occur during pregnancy; dermatoses influenced by pregnancy and the specific dermatoses of pregnancy. A discussion on drugs and pregnancy is presented at the end of this review. Keywords: Dermatology; Pregnancy; Pathology. GRAVIDEZ E PELE INTRODUÇÃO A gravidez representa um período de intensas ções do apetite, náuseas e vômitos, refluxo gastroeso- modificações para a mulher. Praticamente todos os fágico, constipação; e alterações imunológicas varia- sistemas do organismo são afetados, entre eles a pele. -

14. Management of Diabetes in Pregnancy: Standards of Medical
Diabetes Care Volume 42, Supplement 1, January 2019 S165 14. Management of Diabetes in American Diabetes Association Pregnancy: Standards of Medical Care in Diabetesd2019 Diabetes Care 2019;42(Suppl. 1):S165–S172 | https://doi.org/10.2337/dc19-S014 14. MANAGEMENT OF DIABETES IN PREGNANCY The American Diabetes Association (ADA) “Standards of Medical Care in Diabetes” includes ADA’s current clinical practice recommendations and is intended to provide the components of diabetes care, general treatment goals and guidelines, and tools to evaluate quality of care. Members of the ADA Professional Practice Committee, a multidisciplinary expert committee, are responsible for updating the Standards of Care annually, or more frequently as warranted. For a detailed description of ADA standards, statements, and reports, as well as the evidence-grading system for ADA’s clinical practice recommendations, please refer to the Standards of Care Introduction. Readers who wish to comment on the Standards of Care are invited to do so at professional.diabetes.org/SOC. DIABETES IN PREGNANCY The prevalence of diabetes in pregnancy has been increasing in the U.S. The majority is gestational diabetes mellitus (GDM) with the remainder primarily preexisting type 1 diabetes and type 2 diabetes. The rise in GDM and type 2 diabetes in parallel with obesity both in the U.S. and worldwide is of particular concern. Both type 1 diabetes and type 2 diabetes in pregnancy confer significantly greater maternal and fetal risk than GDM, with some differences according to type of diabetes. In general, specific risks of uncontrolled diabetes in pregnancy include spontaneous abortion, fetal anomalies, preeclampsia, fetal demise, macrosomia, neonatal hypoglycemia, and neonatal hyperbilirubinemia, among others. -

Vaginal Breech Birth Mary Olusile Lecturer in Practice
1 Vaginal Breech birth Mary Olusile Lecturer in Practice Breech: is where the fetal buttocks is the presenting part. Occurs in 15% of pregnancies at 28wks reducing to 3-4% at term Usually associated with: Uterine & pelvic anomalies - bicornuate uterus, lax uterus, fibroids and cysts Fetal anomalies - anencephaly, hydrocephaly, multiple gestation, oligohydraminous and polyhydraminous Cornually placed placenta (probably the commonest cause). Diagnosis: by abdominal examination or vaginal examination and confirmed by ultrasound scan Vaginal Breech VS. Caesarean Section Trial by Hannah et al (2001) found CS to produce better outcomes than vaginal breech but does acknowledge that may be due to lost skills of operators Therefore recommended mode of delivery is CS Limitations of trial by Hannah et al have since been highlighted questioning results and conclusion (Kotaska 2004) Now some advocates for vaginal breech birth when selection is based on clear prelabour and intrapartum criteria (Alarab et al 2004) Breech birth is u sually not an option except at clients choice Important considerations are size of fetus, presentation, attitude, size of maternal pelvis and parity of the woman NICE recommendation: External cephalic version (ECV) to be considered and offered if appropriate Produced by CETL 2007 2 Vaginal Breech birth Anterior posterior diameter of the pelvic brim is 11 cm Oblique diameter of the pelvic brim is 12 cm Transverse diameter of the pelvic brim is 13 cm Anterior posterior diameter of the outlet is 13 cm Produced by CETL 2007 3 -

WATER BIRTH in a MATERNITY Hospital of the SUPPLEMENTARY HEALTH SECTOR in SANTA CATARINA, BRAZIL: a CROSS-SECTIONAL STUDY
1 Original Article http://dx.doi.org/10.1590/0104-07072016002180015 WATER BIRTH IN A MATERNITY HOSPITAL OF THE SUPPLEMENTARY HEALTH SECTOR IN SANTA CATARINA, BRAZIL: A CROSS-SECTIONAL STUDY Tânia Regina Scheidt1, Odaléa Maria Brüggemann2 1 M.Sc. in Nursing. Obstetric Nurse, Maternidade Carmela Dutra Hospital. Florianópolis, Santa Catarina, Brazil. E-mail: ainatrs@ gmail.com 2 Ph.D in Obstetrics. Professor, Departamento de Enfermagem, Programa de Pós-Graduação em Enfermagem, Universidade Federal de Santa Catarina. Researcher Brazilian National Council for Scientific and Technological Development (CNPq). Florianópolis, Santa Catarina, Brazil. E-mail: [email protected] ABSTRACT: The aim of this cross-sectional study was to identify the prevalence of water births in a maternity hospital of Santa Catarina, Brazil, and to investigate the association between sociodemographic and obstetric variables and water birth. The sample consisted of 973 women who had normal births between June 2007 and May 2013. Data was analyzed through descriptive and bivariate statistics, and estimated prevalence and tested associations through the use of the chi-square test; the unadjusted and adjusted odds ratio were calculated. The prevalence of water births was 13.7%. Of the 153 women who had water birth, most were aged between 20 to 34 years old (122), had a companion (112), a college degree (136), were primiparous (101), had a pregnancy without complications (129) and were admitted in active labor (94). There was no association between sociodemographic characteristics and obstetric outcomes in the bivariate and multivariate analyses and in the adjusted model. Only women with private sources for payment had the opportunity to give birth in water. -

Systematic Review of Hydrotherapy Research Does a Warm Bath in Labor Promote Normal Physiologic Childbirth?
DOI: 10.1097/JPN.0000000000000260 Continuing Education r r J Perinat Neonat Nurs Volume 31 Number 4, 303–316 Copyright C 2017 Wolters Kluwer Health, Inc. All rights reserved. Systematic Review of Hydrotherapy Research Does a Warm Bath in Labor Promote Normal Physiologic Childbirth? Jenna Shaw-Battista, PhD, RN, NP, CNM, FACNM ABSTRACT Key Words: bath, hydrotherapy, immersion, labor, Health sciences research was systematically reviewed to midwives, normal birth, pain, physiology assess randomized controlled trials of standard care versus immersion hydrotherapy in labor before conventional child- birth. Seven studies of 2615 women were included. Six his article describes a systematic review of re- trials examined hydrotherapy in midwifery care and found search on warm water immersion hydrotherapy an effect of pain relief; of these, 2 examined analgesia and Tduring labor, followed by standard care and con- found reduced use among women who bathed in labor. ventional childbirth. Use of nonpharmacologic comfort One study each found that hydrotherapy reduced maternal and pain relief methods remains limited in the United anxiety and fetal malpresentation, increased maternal satis- States where labor analgesia, anesthesia, and multiple faction with movement and privacy, and resulted in cervical obstetric procedures are routine.1 Higher international dilation progress equivalent to standard labor augmenta- utilization rates suggest a potential for increased US tion practices. Studies examined more than 30 fetal and hydrotherapy utilization and benefits that may include neonatal outcomes, and no benefit or harm of hydrother- support for labor physiology.1–3 Hydrotherapy promotes apy was identified. Two trials had anomalous findings of normal childbirth through reduced use of intrapartum increased newborn resuscitation or nursery admission after interventions due to neuroendocrine, circulatory, mus- hydrotherapy, which were not supported by additional re- culoskeletal and psychological effects of immersion.4 sults in the same or other studies. -

3. Physiologic (Spontaneous) Onset of Labor Versus Scheduled Birth
3. Physiologic (Spontaneous) Onset of Labor versus Scheduled Birth A new report, Hormonal Physiology of Childbearing: Evidence and Implications for Women, Babies, and Maternity Care (2015), synthesizes an extensive literature about hormonally-driven processes of parturition and the early postpartum period. The following information is drawn from this report. Many women and babies experience scheduled birth – induced labor and/or prelabor cesarean – annually in the United States.1 This fact sheet highlights key benefits of the spontaneous, physiologic onset of labor at term, including fully experiencing beneficial hormonal actions of late pregnancy and early labor, and identifies practices that support hormonal physiology when scheduled birth is medically necessary. Benefits of hormonal preparations of late pregnancy and of physiologic onset of labor Hormonal processes that lead up to the physiologic onset of labor prepare mother and fetus/newborn for upcoming tasks and phases. For example: Increases in oxytocin2 and prostaglandin3 receptors, at the physiologic onset of labor prime the uterus to promote effective contractions in labor. Increases in brain-based (central) receptors for beta-endorphins prepare endogenous pain-relieving pathways (to date, found in animal studies).4 Elevations in mammary and central oxytocin and prolactin receptors prepare for breastfeeding and maternal-infant biological bonding.5 Rising cortisol supports maturation of the fetal lungs and other organs. Prelabor preparations in oxytocin and catecholamine systems promote fetal protective processes in labor and optimal newborn transition.6 Practices that support beneficial hormonal action when scheduled birth is necessary When scheduled birth and other interventions are medically necessary, childbearing women and newborns can benefit from support of physiologic processes as far as safely possible. -

OB/GYN – Childbirth/Labor/Delivery Protocol 6 - 2
Section SECTION: Obstetrical and Gynecological Emergencies REVISED: 06/2015 6 1. Physiologic Changes with Pregnancy Protocol 6 - 1 2. OB/GYN – Childbirth/Labor/Delivery Protocol 6 - 2 3. Medical – Newborn/Neonatal Protocol 6 - 3 OB / GYN Resuscitation 4. OB/GYN – Pregnancy Related Protocol 6 - 4 Emergencies (Delivery – Shoulder Dystocia) 5. OB/GYN – Pregnancy Related Protocol 6 - 5 Emergencies (Delivery – Breech Presentation) 6. OB/GYN – Pregnancy Related Protocol 6 - 6 Emergencies (Ectopic Pregnancy/Rupture) 7. OB/GYN – Pregnancy Related Protocol 6 - 7 EMERGENCIES Emergencies (Abruptio Placenta) 8. OB/GYN – Pregnancy Related Protocol 6 - 8 Emergencies (Placenta Previa) 9. OB/GYN – Pregnancy Related Protocol 6 - 9 Emergencies (Umbilical Cord Prolapse) 10. OB/GYN - Eclampsia Protocol 6 - 10 (Hypertension/Eclampsia/HELLPS) 11. OB/GYN – Pregnancy Related Protocol 6 - 11 Emergencies (Premature Rupture of Membranes (PROM)) 12. OB/GYN - Pre-term Labor Protocol 6 - 12 (Pre-term Labor) 13. OB/GYN – Post-partum Hemorrhage Protocol 6 - 13 Created, Developed, and Produced by the Old Dominion EMS Alliance Section 6 Continued This page intentionally left blank. OB / GYN EMERGENCIES Created, Developed, and Produced by the Old Dominion EMS Alliance Protocol SECTION: Obstetrical/Gynecological Emergencies PROTOCOL TITLE: Physiologic Changes with Pregnancy 6-1 REVISED: 06/2017 OVERVIEW: Many changes occur in the pregnant woman’s body, starting from the time of conception and throughout the pregnancy. The most obvious body system to undergo change is the reproductive system, but all of the others will change as well. Brief summaries of the physiologic changes that occur during pregnancy have been listed by system. Most of these physiologic changes will resolve during the postpartum period.