Community Medicine & Primary Health Care
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
YELLOW FEVER SITUATION REPORT Serial Number: 001 February 2021 Monthly Sitrep Epi Week: Week 1, 2020 – Week 08, 2021 Reporting Month: February 2021
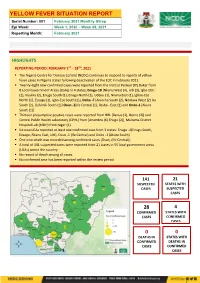
YELLOW FEVER SITUATION REPORT Serial Number: 001 February 2021 Monthly Sitrep Epi Week: Week 1, 2020 – Week 08, 2021 Reporting Month: February 2021 HIGHLIGHTS REPORTING PERIOD: FEBRUARY 1ST – 28TH, 2021 ▪ The Nigeria Centre for Disease Control (NCDC) continues to respond to reports of yellow fever cases in Nigeria states following deactivation of the EOC in February 2021. ▪ Twenty -eight new confirmed cases were reported from the Institut Pasteur (IP) Dakar from 8 Local Government Areas (LGAs) in 4 states; Enugu-18 [Nkanu West (4), Udi (3), Igbo-Etiti (2), Nsukka (2), Enugu South (1), Enugu North (1), Udenu (1), Nkanu East (1), Igboe-Eze North (1), Ezeagu (1), Igbo-Eze South (1)], Delta -7 [Aniocha South (2), Ndokwa West (2) Ika South (2), Oshimili South (1)] Osun -2[Ife Central (1), Ilesha - East (1) and Ondo-1 [Akure South (1)] ▪ Thirteen presumptive positive cases were reported from NRL [Benue (2), Borno (2)] and Central Public Health Laboratory (CPHL) from [Anambra (6) Enugu (2)], Maitama District Hospital Lab (MDH) from Niger (1) ▪ Six new LGAs reported at least one confirmed case from 3 states: Enugu -4(Enugu South, Ezeagu, Nkanu East, Udi), Osun -1 (Ife Central) and Ondo -1 (Akure South) ▪ One new death was recorded among confirmed cases [Osun, (Ife Central)] ▪ A total of 141 suspected cases were reported from 21 states in 55 local government areas (LGAs) across the country ▪ No record of death among all cases. ▪ No confirmed case has been reported within the review period 141 21 SUSPECTED STATES WITH CASES SUSPECTED CASES 28 4 -

The Influence of Vegetation on Microclimate in Hot Humid Tropical Environment: a Case of Enugu Urban
International Journal of Energy and Environmental Research Vol.2,No.4,pp.1-11, December 2014 Published by European Centre for Research Training and Development UK (www.eajournals.org) THE INFLUENCE OF VEGETATION ON MICROCLIMATE IN HOT HUMID TROPICAL ENVIRONMENT: A CASE OF ENUGU URBAN. By Arc. Nich .I. OBI, Assoc. Prof. I.G Chendo Department of Architecture, University of Nigeria, Enugu Campus (UNEC). ABSTRACT: Controlling direct solar radiation and increasing wind velocity to its Optimum capacity are part of planning strategies employed in the design of urban open spaces especially in hot humid tropical environment. Vegetation has the ability to reduce excessive air temperature through sunlight interception. Its geometric configuration influences the amount of solar radiation, air temperature, humidity and wind velocity on microclimate of a given area. Panning strategies aimed at reducing solar heat through application of vegetation were discussed. It also discussed the problem of thermal heat stress affecting the residents of Enugu Urban. The results were analyzed and solutions recommended. KEYWORDS: Open Space; Planning Strategies; Solar Radiation; Tropical Environment; Urban Microclimate. INTRODUCTION According to United Nations (2010), World Bank, (2009), more than half of the world’s population lives in the urban areas. Urbanization trend poses new millennium challenges in both industrialized and developing countries. One of these challenges is thermal heat stress resulting from climate change. The hot humid tropical environment of Enugu is characterized with high intensity of solar radiation and low wind velocity during the hot season. The rapid development activities taking place within the past decade will in no doubt lead to urban heat island effect and plant destruction among other environmental damages. -

Niger Delta Budget Monitoring Group Mapping
CAPACITY BUILDING TRAINING ON COMMUNITY NEEDS ASSESSMENT & SHADOW BUDGETING NIGER DELTA BUDGET MONITORING GROUP MAPPING OF 2016 CAPITAL PROJECTS IN THE 2016 FGN BUDGET FOR ENUGU STATE (Kebetkache Training Group Work on Needs Assessment Working Document) DOCUMENT PREPARED BY NDEBUMOG HEADQUARTERS www.nigerdeltabudget.org ENUGU STATE FEDERAL MINISTRY OF EDUCATION UNIVERSAL BASIC EDUCATION (UBE) COMMISSION S/N PROJECT AMOUNT LGA FED. CONST. SEN. DIST. ZONE STATUS 1 Teaching and Learning 40,000,000 Enugu West South East New Materials in Selected Schools in Enugu West Senatorial District 2 Construction of a Block of 3 15,000,000 Udi Ezeagu/ Udi Enugu West South East New Classroom with VIP Office, Toilets and Furnishing at Community High School, Obioma, Udi LGA, Enugu State Total 55,000,000 FGGC ENUGU S/N PROJECT AMOUNT LGA FED. CONST. SEN. DIST. ZONE STATUS 1 Construction of Road Network 34,264,125 Enugu- North Enugu North/ Enugu East South East New Enugu South 2 Construction of Storey 145,795,243 Enugu-North Enugu North/ Enugu East South East New Building of 18 Classroom, Enugu South Examination Hall, 2 No. Semi Detached Twin Buildings 3 Purchase of 1 Coastal Bus 13,000,000 Enugu-North Enugu North/ Enugu East South East Enugu South 4 Completion of an 8-Room 66,428,132 Enugu-North Enugu North/ Enugu East South East New Storey Building Girls Hostel Enugu South and Construction of a Storey Building of Prep Room and Furnishing 5 Construction of Perimeter 15,002,484 Enugu-North Enugu North/ Enugu East South East New Fencing Enugu South 6 Purchase of one Mercedes 18,656,000 Enugu-North Enugu North/ Enugu East South East New Water Tanker of 11,000 Litres Enugu South Capacity Total 293,145,984 FGGC LEJJA S/N PROJECT AMOUNT LGA FED. -

Evaluation of Groundwater Potential Status in Nkanu-West Local Government Area, Enugu State, Nigeria
IOSR Journal of Applied Geology and Geophysics (IOSR-JAGG) e-ISSN: 2321–0990, p-ISSN: 2321–0982.Volume 4, Issue 6 Ver. I (Nov. - Dec. 2016), PP 79-87 www.iosrjournals.org Evaluation of Groundwater potential status in Nkanu-west Local Government Area, Enugu State, Nigeria. *1Okonkwo A.C, 2Ezeh C.C and 3Amoke A.I 1,2Department of Geology and Mining, Enugu State University of Science and Technology, Enugu, Nigeria. 3Department of Geology, Michael Okpara University of Agriculture, Umudike, Abia State, Nigeria. Abstract: The Evaluation of the groundwater potential status in Nkanu-west Local government area of Enugu State has been undertaken. The project area lies within latitudes 060 25I 00IIN to 060 38I 00IIN and Longitudes 0070 13I 00IIE to 0070 24I 00IIE with an area extent of about 489.4sqkm, over two main geological formations. A total of Seventy-Eight Vertical Electrical Sounding (VES) were acquired, employing the Schlumberger configuration. Resistivity and thickness of aquiferous layers were obtained from the interpreted VES data. Contour variation maps of Apparent resistivity, depth, traverse resistance, Longitudinal conductance, Electrical conductivity, aquifer transmissivity and hydraulic conductivity were constructed. Computed aquifer transmissivity from VES data, indicates medium to low yield aquifer. The latter was used to evaluate the groundwater potential status. Two groundwater potential were mapped; the moderate and low potential zones. The various contour maps and groundwater potential zone map will serve as a useful guide for groundwater exploration in the study area. Keywords: Aquifer yield, Contour maps, Groundwater potential status, Resistivity, Transmissivity, Transverse resistance. I. Introduction Knowledge of groundwater potential status in regions is key useful guide to a successful groundwater exploration and abstraction. -

Enugu State Nigeria Erosion and Watershed
RESETTLEMENT ACTION PLAN (RAP) Public Disclosure Authorized ENUGU STATE NIGERIA EROSION AND WATERSHED MANAGEMENT PROJECT (NEWMAP) Public Disclosure Authorized FOR THE 9TH MILE GULLY EROSION SUB-PROJECT INTERVENTION SITE Public Disclosure Authorized FINAL REPORT Public Disclosure Authorized RESETTLEMENT ACTION PLAN (RAP) ENUGU STATE NIGERIA EROSION AND WATERSHED MANAGEMENT PROJECT (NEWMAP) FOR THE 9TH MILE GULLY EROSION SUB-PROJECT INTERVENTION SITE FINAL REPORT Submitted to: State Project Management Unit Nigeria Erosion and Watershed Management Project (NEWMAP) Enugu State NIGERIA NOVEMBER 2014 Page | ii Resettlement Action Plan for 9th Mile Gully Erosion Site Enugu State- Final Report TABLE OF CONTENTS TABLE OF CONTENTS.................................................................................................................................................................... ii LIST OF FIGURES .................................................................................................................................................................... v LIST OF TABLES...................................................................................................................................................................... v LIST OF PLATES ...................................................................................................................................................................... v DEFINITIONS ....................................................................................................................................................................... -

States and Lcdas Codes.Cdr
PFA CODES 28 UKANEFUN KPK AK 6 CHIBOK CBK BO 8 ETSAKO-EAST AGD ED 20 ONUIMO KWE IM 32 RIMIN-GADO RMG KN KWARA 9 IJEBU-NORTH JGB OG 30 OYO-EAST YYY OY YOBE 1 Stanbic IBTC Pension Managers Limited 0021 29 URU OFFONG ORUKO UFG AK 7 DAMBOA DAM BO 9 ETSAKO-WEST AUC ED 21 ORLU RLU IM 33 ROGO RGG KN S/N LGA NAME LGA STATE 10 IJEBU-NORTH-EAST JNE OG 31 SAKI-EAST GMD OY S/N LGA NAME LGA STATE 2 Premium Pension Limited 0022 30 URUAN DUU AK 8 DIKWA DKW BO 10 IGUEBEN GUE ED 22 ORSU AWT IM 34 SHANONO SNN KN CODE CODE 11 IJEBU-ODE JBD OG 32 SAKI-WEST SHK OY CODE CODE 3 Leadway Pensure PFA Limited 0023 31 UYO UYY AK 9 GUBIO GUB BO 11 IKPOBA-OKHA DGE ED 23 ORU-EAST MMA IM 35 SUMAILA SML KN 1 ASA AFN KW 12 IKENNE KNN OG 33 SURULERE RSD OY 1 BADE GSH YB 4 Sigma Pensions Limited 0024 10 GUZAMALA GZM BO 12 OREDO BEN ED 24 ORU-WEST NGB IM 36 TAKAI TAK KN 2 BARUTEN KSB KW 13 IMEKO-AFON MEK OG 2 BOSARI DPH YB 5 Pensions Alliance Limited 0025 ANAMBRA 11 GWOZA GZA BO 13 ORHIONMWON ABD ED 25 OWERRI-MUNICIPAL WER IM 37 TARAUNI TRN KN 3 EDU LAF KW 14 IPOKIA PKA OG PLATEAU 3 DAMATURU DTR YB 6 ARM Pension Managers Limited 0026 S/N LGA NAME LGA STATE 12 HAWUL HWL BO 14 OVIA-NORTH-EAST AKA ED 26 26 OWERRI-NORTH RRT IM 38 TOFA TEA KN 4 EKITI ARP KW 15 OBAFEMI OWODE WDE OG S/N LGA NAME LGA STATE 4 FIKA FKA YB 7 Trustfund Pensions Plc 0028 CODE CODE 13 JERE JRE BO 15 OVIA-SOUTH-WEST GBZ ED 27 27 OWERRI-WEST UMG IM 39 TSANYAWA TYW KN 5 IFELODUN SHA KW 16 ODEDAH DED OG CODE CODE 5 FUNE FUN YB 8 First Guarantee Pension Limited 0029 1 AGUATA AGU AN 14 KAGA KGG BO 16 OWAN-EAST -

Maternal Reasons for Non-Receipt of Valid Hepatitis B Birth Dose Among
Vaccine 37 (2019) 6894–6899 Contents lists available at ScienceDirect Vaccine journal homepage: www.elsevier.com/locate/vaccine Maternal reasons for non-receipt of valid Hepatitis B birth dose among mother-infant pairs attending routine immunization clinics, South-east, Nigeria ⇑ Uchechukwu Joel Okenwa a,b, , Magbagbeola David Dairo b, Belinda Uba a,c, Olufemi Ajumobi a,c a Nigeria Field Epidemiology and Laboratory Training Program, Abuja, Nigeria b Department of Epidemiology and Medical Statistics, Faculty of Public Health, University of Ibadan, Ibadan, Nigeria c African Field Epidemiology Network, Nigeria Country Office, Abuja, Nigeria article info abstract Article history: Background: Hepatitis B vaccine (HepB) is an effective tool in prevention of hepatitis B virus (HBV) infec- Received 23 April 2019 tion. When administered at birth, it prevents mother-to-child transmission of acute and chronic HBV Received in revised form 16 September infection. However, despite a decade and half of implementation of HepB birth dose (HepB-BD), uptake 2019 has remained persistently low in Enugu State, Nigeria. We assessed the uptake of valid HepB-BD and the Accepted 17 September 2019 reasons given by mothers of infants for not receiving the HepB-BD in Enugu State, South-east Nigeria. Available online 24 September 2019 Methods: An hospital-based cross-sectional survey was conducted among mother-infant pairs attending immunization clinics at randomly selected health facilities in Enugu State, Nigeria. Overall, 344 mothers Keywords: and their infant children in this study were interviewed using structured questionnaire. Data on maternal Hepatitis B valid-birth-dose Immunization reasons for non-receipt of valid HepB-BD by their infants and their recommendations on ways to improve Maternal valid HepB-BD uptake, were collected. -

Volume 9 Number 3 September 2010 Pp
215 Agro-Science Journal of Tropical Agriculture, Food, Environment and Extension Volume 9 Number 3 September 2010 pp. 215 -222 ISSN 1119-7455 WOMEN MARKETERS’ PERCEIVED CONSTRAINTS ON SELECTED AGRICULTURAL PRODUCE MARKETING IN ENUGU SOUTH AREA: CHALLENGES OF EXTENSION TRAINING FOR WOMEN GROUPS IN ENUGU STATE, NIGERIA Eze 1 S.O., Onwubuya 2 E.A and Ezeh 3 A.N 1Dept of Agricultural Economics, Management and Extension Ebonyi State University, P.M.B 053 Abakaliki , Nigeria. 2Department of Agricultural Extension University of Nigeria, Nsukka, Nigeria. ABSTRACT Women constitute great apostles in agricultural production, processing, utilization and marketing as well as national economic growth. Given the increasing demands for basic crop products such as garri and milled rice in the diets of most households in Enugu south area, Nigeria, the marketing situation seems to be low relative to distribution. In this regard, this study investigated women marketers’ perceived constraints on marketing of milled rice and garri in Enugu south area and highlighted challenges of extension training for women groups in Enugu State, Nigeria. One hundred and sixty randomly selected women marketers in Enugu South area constituted the sample size for the study. Structured interview schedule was employed in data collection.Frequency counts, percentage and factor analysis technique were the analytical tools adopted. The findings revealed that majority (63.8%) of the women were within the ages of 31-50 years, while majority (75.5%) have 6-20 years of marketing experience and 69.4 % of them have equity capital of N5,001.00- N45,000.00. The major constraints perceived by the women included inadequate processing skill, produce deterioration and lack of storage facilities. -

Observed Urban Heat Island Characteristics in Enugu Urban During the Dry Season by Enete, Ifeanyi
Global Journal of HUMAN SOCIAL SCIENCE Geography & Environmental GeoSciences Volume 12 Issue 10 Version 1.0 Year 2012 Type: Double Blind Peer Reviewed International Research Journal Publisher: Global Journals Inc. (USA) Online ISSN: 2249-460x & Print ISSN: 0975-587X Observed Urban Heat Island Characteristics in Enugu Urban During the Dry Season By Enete, Ifeanyi. C & Alabi, M.O Nnamdi Azikiwe University, Awka Abstract - Aim : The dry season microclimate variation at several sites in Enugu was assessed with the sole aim of determining the UHI characteristics during dry season periods. Study Design: The study design employed in the study was survey design. Place and Duration of the study: Enugu urban was the study area and the study occurred between the months of Feb – Mar 2006 and 2007. Methodology : During the study, transect and fixed point measurements were taken hourly and averaged over a month. All temperature difference was calculated as site temperature minus reference temperature. Thus, a negative (-) temperature difference indicates that the site was cooler than the reference station. The reference station is the rural environment. Results : Dry season months showed strong variability in temperature. The downtown site was the warmest (2.0 0c) during the day. The heavily vegetated urban residential site (LVR) and suburban site (LOR) with fully developed vegetation canopy were the coolest (-3.8 and -2.68). Keywords : Urban heat island, rural, intraurban. GJHSS-C Classification : FOR Code: 120504, 120507 Observed Urban Heat Island Characteristics in Enugu Urban During the Dry Season Strictly as per the compliance and regulations of: © 2012. Enete, Ifeanyi. C & Alabi, M.O. -

Enugu State, Nigeria) Urban Growth and Development
Quest Journals Journal of Research in Environmental and Earth Sciences Volume 1 ~ Issue 3 (2014) pp: 44-51 ISSN(Online) : 2348-2532 www.questjournals.org Research Paper A Review of Enugu (Enugu State, Nigeria) Urban Growth and Development Edmund Amuezuoke Iyi Received 14 November, 2014; Accepted 06 December, 2014 © The author(s) 2014. Published with open access at www.questjournals.org ABSTRACT:- Enugu Urban of Enugu State of Nigeria came into being as a result of the discovery of coal in the area in 1917 by the European explorers. This paper presents a study carried out to appraise the growth and development of the area over the past five years. Survey research design was adopted in the study. Multiple regression analysis was used in analyzing the data collected during the study. The use of the model was to ascertain the magnitude and significance of relationship among the identified development indicators. The test was performed at 5% level of significance. The analysis revealed that there is only a weak relationship among the identified indicators. The trend of development from the initial points to other areas was rapid initially but slowed down in the later years. The slow pace in development was identified to have resulted from inadequate attention to newer innovations to cater for ever increasing population of both people and vehicles. It is suggested that vigorous efforts be made to anticipate workable new innovations in urban design and management chief, of which is the Environmental Planning and Management (EPM) approach. Keywords:- Development indicator, Survey research, innovations, Environmental Planning and Management. -

Solid Mineral Resources of ENUGU State: a Review
International Journal of Science and Research (IJSR) ISSN (Online): 2319-7064 Index Copernicus Value (2013): 6.14 | Impact Factor (2014): 5.611 Solid Mineral Resources of ENUGU State: A Review Onyeabor Chinenye Florence Department of Geology and Mining, Enugu State University of Science and Technology Abstract: Enugu state, southeastern Nigeria is endowed with many natural resources which include coal, oil shale, gas, glass sands, ironstone, clay minerals, limestone, gypsum and alum. They occur in various formations of the state which includes Enugu Shale, Mamu Formation, Ajali Formation, Nsukka Formation and Imo shale. The minerals presently under exploitation are clay, sand, ironstone with others being under exploited or found in an uneconomic reserve. Mining of coal ceased since the 1990’s hence reducing drastically the economic hub of the state. The return to coal exploitation and other solid minerals will enhance the economic output of the state. Keywords: Glass sands; coal; ironstone; limestone; mineral 1. Introduction Enugu state is one of the key states in Southeastern Nigeria. Enugu has served as capital of various defunct geopolitical regions known as Eastern Region, East Central State and Anambra State. The state is situated within longitudes 60501E and long.70521E and latitudes 60001N and lat.70101N. The entire areal extent is 7,161 sq. kilometers and the estimated population is 4,267,837 people (Census 2006). Presently Enugu State consists of 17 local government areas (fig.1). It is bordered to the north by Benue state and to the west by Anambra state, to the east by Ebonyi state, and Abia State to the south. -

Perceived Influence of Non-Formal Educational Programmes on Basic Academic Attainment of Teenage Mothers in Enugu State Nigeria
Perceived Influence of Non-Formal Educational Programmes on Basic Academic Attainment of Teenage Mothers in Enugu State Nigeria Eddiefloyd M. Igbo Ibrahim Badamasi Babangida University, Lapai, Nigeria Rosemary O. Igbo James C. Ayaogu Enugu State University of Science & Technology, Enugu State, Nigeria Abstract: The study examined perceived influence of non-formal education programmes on the basic academic attainment of teenage mothers in Enugu state Nigeria. The total population for the study was 8,143 teenage mothers from which a study sample of 814 was raised. Four research questions were raised and four hypotheses were tested. Twenty-three items were used to elicit information from the teenage mothers. A four point scale was used to rate the responses. The research questions were answered using mean statistic(x), while t- test analysis was done to test the hypotheses at .05 significant levels. The findings showed that teenage mothers in Enugu state perceived a low influence of radio lessons on their ability to participate in practical subjects, cover subject topics and sit mainstream examinations. They however, perceived high influence of correspondence courses and evening lessons on their ability to study school subjects and sit mainstream examinations. Recommendations were made, which include the adoption of modern technology in the facilitation of learning for this group of learners especially one that guarantees personal relationship between the trainer(s) and trainees(s). INTRODUCTION Equal opportunity in all aspects of education is an injunction of the government of the Federal Republic of Nigeria that is spelt out in section 1 of the National Policy on education (FGN, 2004), to ensure that various groups in society access educational provision irrespective of their age and ability.