Equity and the Cuban National Health System's Response to COVID-19*
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Cuba by Sea Cienfuegos to Havana Aboard Variety Voyager
MUSEUM TRAVEL ALLIANCE Cuba by Sea Cienfuegos to Havana Aboard Variety Voyager January 24–February 1, 2019 MUSEUM TRAVEL ALLIANCE Dear Members and Friends of the National Building Museum, Please join us next January for a cultural cruise along Cuba’s Caribbean coast. From Cienfuegos to Havana, we will journey aboard a privately chartered yacht, discovering well-preserved colonial architecture and fascinating small museums, visiting talented artists in their studios, and enjoying private concerts and other exclusive events. The Museum Travel Alliance (MTA) provides museums with the opportunity to offer their members and patrons high-end educational travel programming. Trips are available exclusively through MTA members and co-sponsoring non- profit institutions. This voyage is co-sponsored by The Metropolitan Museum of Art and the Association of Yale Alumni. Traveling with us on this cultural cruise are a Cuban-American architect and a partner in an award-winning design firm, a curator from The Metropolitan Museum of Art, and a Professor in the Music Department and African American Studies and American Studies at Yale University. In Cienfuegos, view the city’s French-accented buildings on an architectural tour before boarding the sleek Variety Voyager to travel to picturesque Trinidad. Admire the exquisite antiques and furniture displayed in the Romantic Museum and tour the studios of prominent local artists. Continue to Cayo Largo to meet local naturalists, and to remote Isla de la Juventud to see the Panopticon prison (now a museum) that once held Fidel Castro. We will also visit with marine ecologists on María la Gorda, a UNESCO Biosphere Reserve, before continuing to Havana for our two-day finale. -
Overview Print Page Close Window
World Directory of Minorities Americas MRG Directory –> Cuba –> Cuba Overview Print Page Close Window Cuba Overview Environment Peoples History Governance Current state of minorities and indigenous peoples Environment Cuba is the largest island in the Caribbean. It is located 150 kilometres south of the tip of the US state of Florida and east of the Yucatán Peninsula. On the east, Cuba is separated by the Windward Passage from Hispaniola, the island shared by Haiti and Dominican Republic. The total land area is 114,524 sq km, which includes the Isla de la Juventud (formerly called Isle of Pines) and other small adjacent islands. Peoples Main languages: Spanish Main religions: Christianity (Roman Catholic, Protestant), syncretic African religions The majority of the population of Cuba is 51% mulatto (mixed white and black), 37% white, 11% black and 1% Chinese (CIA, 2001). However, according to the Official 2002 Cuba Census, 65% of the population is white, 10% black and 25% mulatto. Although there are no distinct indigenous communities still in existence, some mixed but recognizably indigenous Ciboney-Taino-Arawak-descended populations are still considered to have survived in parts of rural Cuba. Furthermore the indigenous element is still in evidence, interwoven as part of the overall population's cultural and genetic heritage. There is no expatriate immigrant population. More than 75 per cent of the population is classified as urban. The revolutionary government, installed in 1959, has generally destroyed the rigid social stratification inherited from Spanish colonial rule. During Spanish colonial rule (and later under US influence) Cuba was a major sugar-producing territory. -

How to Cite Complete Issue More Information About This Article Journal's Webpage in Redalyc.Org Scientific Information System Re
Cultivos Tropicales ISSN: 1819-4087 Ediciones INCA Benítez-Fernández, Bárbara; Crespo-Morales, Anaisa; Casanova, Caridad; Méndez-Bordón, Aliek; Hernández-Beltrán, Yaima; Ortiz- Pérez, Rodobaldo; Acosta-Roca, Rosa; Romero-Sarduy, María Isabel Impactos de la estrategia de género en el sector agropecuario, a través del Proyecto de Innovación Agropecuaria Local (PIAL) Cultivos Tropicales, vol. 42, no. 1, e04, 2021, January-March Ediciones INCA DOI: https://doi.org/10.1234/ct.v42i1.1578 Available in: https://www.redalyc.org/articulo.oa?id=193266707004 How to cite Complete issue Scientific Information System Redalyc More information about this article Network of Scientific Journals from Latin America and the Caribbean, Spain and Journal's webpage in redalyc.org Portugal Project academic non-profit, developed under the open access initiative Cultivos Tropicales, 2021, vol. 42, no. 1, e04 enero-marzo ISSN impreso: 0258-5936 Ministerio de Educación Superior. Cuba ISSN digital: 1819-4087 Instituto Nacional de Ciencias Agrícolas http://ediciones.inca.edu.cu Original article Impacts of the gender strategy in the agricultural sector, through the Local Agricultural Innovation Project (PIAL) Bárbara Benítez-Fernández1* Anaisa Crespo-Morales2 Caridad Casanova3 Aliek Méndez-Bordón4 Yaima Hernández-Beltrán5 Rodobaldo Ortiz-Pérez1 Rosa Acosta-Roca1 María Isabel Romero-Sarduy6 1Instituto Nacional de Ciencias Agrícolas (INCA), carretera San José-Tapaste, km 3½, Gaveta Postal 1, San José de las Lajas, Mayabeque, Cuba. CP 32 700 2Policlínico Docente “Pedro Borrás Astorga”, Calle Comandante Cruz # 70, La Palma, Pinar del Río, Cuba 3Universidad de Cienfuegos “Carlos Rafael Rodríguez”, carretera a Rodas, km 3 ½, Cuatro Caminos, Cienfuegos, Cuba 4Universidad Las Tunas, Centro Universitario Municipal “Jesús Menéndez”, calle 28 # 33, El Cenicero, El batey, Jesús Menéndez, Las Tunas, Cuba 5Universidad de Sancti Spíritus “José Martí Pérez”. -
Highlights Situation Overview
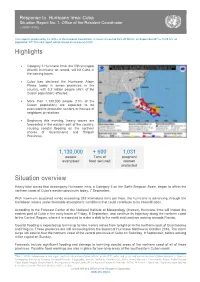
Response to Hurricane Irma: Cuba Situation Report No. 1. Office of the Resident Coordinator ( 07/09/ 20176) This report is produced by the Office of the Resident Coordinator. It covers the period from 20:00 hrs. on September 06th to 14:00 hrs. on September 07th.The next report will be issued on or around 08/09. Highlights Category 5 Hurricane Irma, the fifth strongest Atlantic hurricane on record, will hit Cuba in the coming hours. Cuba has declared the Hurricane Alarm Phase today in seven provinces in the country, with 5.2 million people (46% of the Cuban population) affected. More than 1,130,000 people (10% of the Cuban population) are expected to be evacuated to protection centers or houses of neighbors or relatives. Beginning this evening, heavy waves are forecasted in the eastern part of the country, causing coastal flooding on the northern shores of Guantánamo and Holguín Provinces. 1,130,000 + 600 1,031 people Tons of pregnant evacuated food secured women protected Situation overview Heavy tidal waves that accompany Hurricane Irma, a Category 5 on the Saffir-Simpson Scale, began to affect the northern coast of Cuba’s eastern provinces today, 7 September. With maximum sustained winds exceeding 252 kilometers (km) per hour, the hurricane is advancing through the Caribbean waters under favorable atmospheric conditions that could contribute to its intensification. According to the Forecast Center of the National Institute of Meteorology (Insmet), Hurricane Irma will impact the eastern part of Cuba in the early hours of Friday, 8 September, and continue its trajectory along the northern coast to the Central Region, where it is expected to make a shift to the north and continue moving towards Florida. -

Federal Register/Vol. 85, No. 188/Monday, September 28, 2020
Federal Register / Vol. 85, No. 188 / Monday, September 28, 2020 / Notices 60855 comment letters on the Proposed Rule Proposed Rule Change and to take that the Secretary of State has identified Change.4 action on the Proposed Rule Change. as a property that is owned or controlled On May 21, 2020, pursuant to Section Accordingly, pursuant to Section by the Cuban government, a prohibited 19(b)(2) of the Act,5 the Commission 19(b)(2)(B)(ii)(II) of the Act,12 the official of the Government of Cuba as designated a longer period within which Commission designates November 26, defined in § 515.337, a prohibited to approve, disapprove, or institute 2020, as the date by which the member of the Cuban Communist Party proceedings to determine whether to Commission should either approve or as defined in § 515.338, a close relative, approve or disapprove the Proposed disapprove the Proposed Rule Change as defined in § 515.339, of a prohibited Rule Change.6 On June 24, 2020, the SR–NSCC–2020–003. official of the Government of Cuba, or a Commission instituted proceedings For the Commission, by the Division of close relative of a prohibited member of pursuant to Section 19(b)(2)(B) of the Trading and Markets, pursuant to delegated the Cuban Communist Party when the 7 Act, to determine whether to approve authority.13 terms of the general or specific license or disapprove the Proposed Rule J. Matthew DeLesDernier, expressly exclude such a transaction. 8 Change. The Commission received Assistant Secretary. Such properties are identified on the additional comment letters on the State Department’s Cuba Prohibited [FR Doc. -

Abrir En Una Nueva Pestaña
Nombre Apellidos Profesión Lugar donde fue visto por última vez Provincia Hora de detención Fecha de detención Último reporte Si tienes una denuncia o actualización sobre las personas detenidas o desparecidas en las protestas de julio, envía un mensaje a Cubalex +1 901 7080230, publica en el grupo de Facebook DESAPARECIDOS #SOSCuba (https://www.facebook.com/groups/243016724042825), o etiqueta en Twitter a @CubalexDDHH, @onceagainsalome o @cantera89. Comparte esta lista para mayor difusión. Abdiel Cedeño Martínez Desconocida Parque el Caney Santiago de Cuba Abel Lescay Desconocida Bejucal Mayabeque 12.07 7am 12/07/2021 Adonis Abilleira Desconocida Cruces Cienfuegos Adrian Portieles Desconocida Desaparecido! No se sabe donde lo tienen. TrinidadSancti Spiritus 11/07/2021 Alejandro Mejías Guerra Desconocida San Antonio de los Baños Artemisa Alejandro Rodríguez Gelin Desconocida Detenido en Jovellanos Matanzas Alejandro Naranjo Desconocida Con su esposa Yenny Santiago de Cuba 11/07/2021 Alejandro Criado González Desconocida Detenido en Zanja La Habana 3pm 12/07/2021 Liberado 13/07/2021 Alejandro Rojas Calzadilla Desconocida Frente al hotel Saratoga La Habana 11/07/2021 Alejandro Núñez Maldonado Informatico Detenido en el Cotorro La Habana 11/07/2021 Alexander Fabregas Desconocida Sancti Spiritus Alvaro Otero Rodríguez Desconocida Trinidad Sancti Spiritus Amalia Portieles Desconocida ICRT La Habana 12/07/2021 Amanda Hernández Desconocida Infanta y San Lázaro La Habana 11/07/2021 Amaury Pacheco Artista P11 La Habana 11/07/2021 Liberado y sitiado -

Alexander Sánchez-Ruiz
ARTÍCULO: CURRENT TAXONOMIC STATUS OF THE FAMILY CAPONIIDAE (ARACHNIDA, ARANEAE) IN CUBA WITH THE DESCRIPTION OF TWO NEW SPECIES Alexander Sánchez-Ruiz Abstract: All information known about the spider species of the family Caponiidae recorded from Cuba is compiled. Two new species of the genus Nops MacLeay, 1839 (Araneae, Caponiidae) are described from eastern Cuba, raising to seven the number of species in the Caponiidae fauna of this archipelago. Key words: Araneae, Caponiidae, taxonomy, West Indies, Cuba. Taxonomy: Nops enae sp. n. Nops siboney sp. n. ARTÍCULO: Current taxonomic status of the Estado taxonómico actual de la familia Caponiidae (Arachnida, Araneae) en family Caponiidae (Arachnida, Cuba y descripción de dos especies nuevas Araneae) in Cuba with the description of two new species Resumen: Se recopila toda la información conocida acerca de las especies de arañas de la familia Alexander Sánchez-Ruiz Caponiidae registradas para Cuba. Se describen dos nuevas especies del género Nops Centro Oriental de Ecosistemas y MacLeay, 1839 (Araneae, Caponiidae) procedentes del oriente de Cuba, alcanzando las Biodiversidad, Museo de Historia siete especies la fauna de Caponiidae de este archipiélago. Natural “Tomás Romay”, José A. Palabras clave: Araneae, Caponiidae, taxonomía, Antillas, Cuba. Saco # 601, Santiago de Cuba Taxonomía: 90100, Cuba. Nops enae sp. n. [email protected] Nops siboney sp. n. Revista Ibérica de Aracnología ISSN: 1576 - 9518. Dep. Legal: Z-2656-2000. Introduction Vol. 9, 30-VI-2004 Sección: Artículos y Notas. The family Caponiidae in the New World is represented by nine genera: Calponia Pp: 95–102. Platnick 1993, Caponina Simon, 1891, Nops MacLeay, 1839, Nopsides Chamberlin, 1924, Notnops Platnick, 1994, Orthonops Chamberlin, 1924, Taintnops Platnick, Edita: 1994, Tarsonops Chamberlin, 1924 and Tisentnops Platnick, 1994. -

Country Portfolio Evaluation Report: Cuba (1992-2011)
GEF/ME/C.44/Inf. 05 May 23, 2013 GEF Council June 18-20, 2013 Washington, D.C. COUNTRY PORTFOLIO EVALUATION REPORT: CUBA (1992-2011) (Prepared by the GEF Evaluation Office) TABLE OF CONTENTS Introduction ................................................................................................................................................. 1 Evaluation Scope and Methodology ............................................................................................... 2 Conclusions .................................................................................................................................................. 4 Effectiveness, Results and Sustainability ....................................................................................... 4 Relevance ....................................................................................................................................... 14 Efficiency ....................................................................................................................................... 17 Recommendations ...................................................................................................................................... 21 ii INTRODUCTION 1. At the request of the Global Environment Facility (GEF) Council, the GEF Evaluation Office conducts a number of CPEs every year. In fiscal year 12,1 in addition to the CPE in Cuba, the GEF Evaluation Office has been conducting CPEs in Brazil, India and Sri Lanka. Furthermore, a Country Portfolio Study (CPSs) has -

Introduced Amphibians and Reptiles in the Cuban Archipelago
Herpetological Conservation and Biology 10(3):985–1012. Submitted: 3 December 2014; Accepted: 14 October 2015; Published: 16 December 2015. INTRODUCED AMPHIBIANS AND REPTILES IN THE CUBAN ARCHIPELAGO 1,5 2 3 RAFAEL BORROTO-PÁEZ , ROBERTO ALONSO BOSCH , BORIS A. FABRES , AND OSMANY 4 ALVAREZ GARCÍA 1Sociedad Cubana de Zoología, Carretera de Varona km 3.5, Boyeros, La Habana, Cuba 2Museo de Historia Natural ”Felipe Poey.” Facultad de Biología, Universidad de La Habana, La Habana, Cuba 3Environmental Protection in the Caribbean (EPIC), Green Cove Springs, Florida, USA 4Centro de Investigaciones de Mejoramiento Animal de la Ganadería Tropical, MINAGRI, Cotorro, La Habana, Cuba 5Corresponding author, email: [email protected] Abstract.—The number of introductions and resulting established populations of amphibians and reptiles in Caribbean islands is alarming. Through an extensive review of information on Cuban herpetofauna, including protected area management plans, we present the first comprehensive inventory of introduced amphibians and reptiles in the Cuban archipelago. We classify species as Invasive, Established Non-invasive, Not Established, and Transported. We document the arrival of 26 species, five amphibians and 21 reptiles, in more than 35 different introduction events. Of the 26 species, we identify 11 species (42.3%), one amphibian and 10 reptiles, as established, with nine of them being invasive: Lithobates catesbeianus, Caiman crocodilus, Hemidactylus mabouia, H. angulatus, H. frenatus, Gonatodes albogularis, Sphaerodactylus argus, Gymnophthalmus underwoodi, and Indotyphlops braminus. We present the introduced range of each of the 26 species in the Cuban archipelago as well as the other Caribbean islands and document historical records, the population sources, dispersal pathways, introduction events, current status of distribution, and impacts. -

Cuba Ñ a Jewel of the Caribbean by Alvanir “Jornada” S
DEPARTMENTS DIVING WORLD Cuba Ñ A Jewel of the Caribbean By Alvanir “Jornada” S. Oliveira, NAUI 19845 Cuba, officially the Republic of Cuba, Between 1953 and 1959, the Cuban on the island are Cayo Largo, Maria is an island country located in the Revolution took place, removing the la Gorda and Isla de la Juventud, northern Caribbean. It is bounded by dictatorship of Fulgencio Batista and among others. Some portions of the the Caribbean Sea (or Mar Caribe) to installing the communist regime Underwater Photography World the south, the Gulf of Mexico to the under Fidel Castro. Since then, Cuba Championship took place in Cuba, the northwest and the Atlantic Ocean to seems in many ways to have stopped most recent occurring in 2013. All of the northeast. The Cuban archipelago in time. It is still possible to see the island’s dive centers are owned by consists of the main island of Cuba, hundreds of well-maintained cars government companies. the Isla de la Juventud (Isle of Youth) from the 1950s driving through the The photos accompanying this and several smaller islands. Havana streets of the country. article were taken on Isla de la is the largest city in Cuba and the Cuba is home to more than 11 Juventud at the Punta Frances Marine capital of the country, with Santiago million people and is the Caribbean’s National Park, which has more than de Cuba being the second-largest city. most populous island nation. 50 different dive sites. There are Cuba’s geographic neighbors include Politically, Cuba is the only socialist excellent dives for beginner divers as the United States and Bahamas to the country in the Americas today. -

Ever Faithful
Ever Faithful Ever Faithful Race, Loyalty, and the Ends of Empire in Spanish Cuba David Sartorius Duke University Press • Durham and London • 2013 © 2013 Duke University Press. All rights reserved Printed in the United States of America on acid-free paper ∞ Tyeset in Minion Pro by Westchester Publishing Services. Library of Congress Cataloging- in- Publication Data Sartorius, David A. Ever faithful : race, loyalty, and the ends of empire in Spanish Cuba / David Sartorius. pages cm Includes bibliographical references and index. ISBN 978- 0- 8223- 5579- 3 (cloth : alk. paper) ISBN 978- 0- 8223- 5593- 9 (pbk. : alk. paper) 1. Blacks— Race identity— Cuba—History—19th century. 2. Cuba— Race relations— History—19th century. 3. Spain— Colonies—America— Administration—History—19th century. I. Title. F1789.N3S27 2013 305.80097291—dc23 2013025534 contents Preface • vii A c k n o w l e d g m e n t s • xv Introduction A Faithful Account of Colonial Racial Politics • 1 one Belonging to an Empire • 21 Race and Rights two Suspicious Affi nities • 52 Loyal Subjectivity and the Paternalist Public three Th e Will to Freedom • 94 Spanish Allegiances in the Ten Years’ War four Publicizing Loyalty • 128 Race and the Post- Zanjón Public Sphere five “Long Live Spain! Death to Autonomy!” • 158 Liberalism and Slave Emancipation six Th e Price of Integrity • 187 Limited Loyalties in Revolution Conclusion Subject Citizens and the Tragedy of Loyalty • 217 Notes • 227 Bibliography • 271 Index • 305 preface To visit the Palace of the Captain General on Havana’s Plaza de Armas today is to witness the most prominent stone- and mortar monument to the endur- ing history of Spanish colonial rule in Cuba. -

The Second Wave of the COVID-19 Epidemic in Cuba: the Sixth- and Seventh-Month Flare-Ups
EDITORIAL The second wave of the COVID-19 epidemic in Cuba: the sixth- and seventh-month flare-ups Enrique Beldarraín-Chaple, MD PhD; Ileana R. Alfonso-Sánchez, PhD; María Vidal-Ledo PhD Introduction The remaining 44,067 confirmed cases (6,703 on COVID-19 is a respiratory disease caused that day) and 1,440 deaths (310 of them new) were by the SARS-CoV-2 virus. It was first diagnosed distributed among the 118 countries reporting in December 2019 in the Chinese city of Wuhan, cases of the disease.[4] Hubei province, and was found to generate In the Cuban epidemic, cases increased pneumonia different from that produced by other during March, and on April 24th, the curve reached viruses. [1] The disease was very aggressive and its acme with 849 active cases. From May contagious and spread rapidly to other Asian onwards, the number of positive cases decreased countries and the rest of the world, causing a and, although 244 cases were reported on June 7th, pandemic. On January 30th, 2020, the WHO the curve continued to decrease until mid-July, [5] declared it a global emergency. [2] which indicates an effective control of the disease The first three cases of COVID-19 in Cuba in the country. were reported on March 11th of the same year.[3] When the first cases were diagnosed, the That same day, the WHO declared 125,048 Province and Municipality Defense Councils were confirmed cases worldwide (6,729 on that day) activated. These councils are made up of decision- and 4,613 deaths (321 of them new).