In This Chapter, We Will Examine
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Sensory Receptors A17 (1)
SENSORY RECEPTORS A17 (1) Sensory Receptors Last updated: April 20, 2019 Sensory receptors - transducers that convert various forms of energy in environment into action potentials in neurons. sensory receptors may be: a) neurons (distal tip of peripheral axon of sensory neuron) – e.g. in skin receptors. b) specialized cells (that release neurotransmitter and generate action potentials in neurons) – e.g. in complex sense organs (vision, hearing, equilibrium, taste). sensory receptor is often associated with nonneural cells that surround it, forming SENSE ORGAN. to stimulate receptor, stimulus must first pass through intervening tissues (stimulus accession). each receptor is adapted to respond to one particular form of energy at much lower threshold than other receptors respond to this form of energy. adequate (s. appropriate) stimulus - form of energy to which receptor is most sensitive; receptors also can respond to other energy forms, but at much higher thresholds (e.g. adequate stimulus for eye is light; eyeball rubbing will stimulate rods and cones to produce light sensation, but threshold is much higher than in skin pressure receptors). when information about stimulus reaches CNS, it produces: a) reflex response b) conscious sensation c) behavior alteration SENSORY MODALITIES Sensory Modality Receptor Sense Organ CONSCIOUS SENSATIONS Vision Rods & cones Eye Hearing Hair cells Ear (organ of Corti) Smell Olfactory neurons Olfactory mucous membrane Taste Taste receptor cells Taste bud Rotational acceleration Hair cells Ear (semicircular -

Somatotopic Organization of Perioral Musculature Innervation Within the Pig Facial Motor Nucleus
Original Paper Brain Behav Evol 2005;66:22–34 Received: September 20, 2004 Returned for revision: November 10, 2004 DOI: 10.1159/000085045 Accepted after revision: December 7, 2004 Published online: April 8, 2005 Somatotopic Organization of Perioral Musculature Innervation within the Pig Facial Motor Nucleus Christopher D. Marshall a Ron H. Hsu b Susan W. Herring c aTexas A&M University at Galveston, Galveston, Tex., bDepartment of Pediatric Dentistry, University of North Carolina, Chapel Hill, N.C., and cDepartment of Orthodontics, University of Washington, Seattle, Wash., USA Key Words pools of the lateral 4 of the 7 subnuclei of the facial motor Somatotopy W Innervation W Facial nucleus W Perioral nucleus. The motor neuron pools of the perioral muscles muscles W Orbicularis oris W Buccinator W Mammals were generally segregated from motoneurons innervat- ing other facial muscles of the rostrum. However, motor neuron pools were not confined to single nuclei but Abstract instead spanned across 3–4 subnuclei. Perioral muscle The orbicularis oris and buccinator muscles of mammals motor neuron pools overlapped but were organized so- form an important subset of the facial musculature, the matotopically. Motor neuron pools of portions of the perioral muscles. In many taxa, these muscles form a SOO overlapped greatly with each other but exhibited a robust muscular hydrostat capable of highly manipula- crude somatotopy within the SOO motor neuron pool. tive fine motor movements, likely accompanied by a spe- The large and somatotopically organized SOO motor cialized pattern of innervation. We conducted a retro- neuron pool in pigs suggests that the upper lip might be grade nerve-tracing study of cranial nerve (CN) VII in pigs more richly innervated than the other perioral muscles (Sus scrofa) to: (1) map the motor neuron pool distribu- and functionally divided. -

Neurolosical Manifestations of Diabetes Mellitus
1954] MANIFESTATIONS OF DIABETES MELLITUS : VAISHNAVA 463 is the commonest lesion in diabetic neuropathy inal Articles but nerve trunks, spinal ganglia, posterior nerve Orig roots, posterior and lateral columns and ante- rior horn cells of the spinal cord or the motor nuclei of the brain stem, the autonomic ner- Neurological manifestations of vous system and the brain may also be affected. DIABETES MELLITUS The lower extremities appear to bear the greatest brunt of the disease. % HARI P. VAISHNAVA, m.b., b.s. (Lucknow), exact mechanism of these M.R.C.P. (Ed.) The neurological manifestations is not known. As this condi- Medical Registrar and Resident Medical Officer, tion is more common in elderly people, arterio- Victoria Hospital, Blackpool, England sclerosis is considered the most likely cause Neurological complications of diabetes though this theory does not account for its ^ellitug have baffled many physicians. There occurrence in younger people without signs of ]s an extensive American literature on this sub- arterio-sclerosis; moreover, so many elderly ject which is being increasingly recognised in subjects with arterio-sclerosis do not suffer ?ther countries. The incidence of diabetic neu- from neuropathy. r?Pathy varies with different authors, Jordan Martin (1953).states that the condition is a (1936) mentioning 67 per cent; Collens at al degenerative one in which non-myelinated (1952) 93 per cent ; Bonkalo (1950) 49.3 per small calibre fibres degenerate more extensively contrasting with Rundles (1945) 5 per cent. ^eilt, than the larger myelinated ones. The primary *he difference in these figures is mainly due to lesion, according to Martin, is a degeneration lriterpretation of the symptoms; if objective of axis cylinders and sheaths are re- ^gns must be taken into account with the myelin duced as a secondary effect. -

A Systematic Review of Structural and Functional MRI Stud
Yin et al. The Journal of Headache and Pain (2020) 21:78 The Journal of Headache https://doi.org/10.1186/s10194-020-01131-4 and Pain REVIEW ARTICLE Open Access The neuro-pathophysiology of temporomandibular disorders-related pain: a systematic review of structural and functional MRI studies Yuanyuan Yin1,2†, Shushu He2†, Jingchen Xu2, Wanfang You1,3, Qian Li1,3, Jingyi Long1,3, Lekai Luo1,3, Graham J. Kemp4, John A. Sweeney1,5, Fei Li1,3*, Song Chen2* and Qiyong Gong1,3 Abstract Chronic pain surrounding the temporomandibular joints and masticatory muscles is often the primary chief complaint of patients with temporomandibular disorders (TMD) seeking treatment. Yet, the neuro-pathophysiological basis underlying it remains to be clarified. Neuroimaging techniques have provided a deeper understanding of what happens to brain structure and function in TMD patients with chronic pain. Therefore, we performed a systematic review of magnetic resonance imaging (MRI) studies investigating structural and functional brain alterations in TMD patients to further unravel the neurobiological underpinnings of TMD-related pain. Online databases (PubMed, EMBASE, and Web of Science) were searched up to August 3, 2019, as complemented by a hand search in reference lists. A total of 622 papers were initially identified after duplicates removed and 25 studies met inclusion criteria for this review. Notably, the variations of MRI techniques used and study design among included studies preclude a meta-analysis and we discussed the findings qualitatively according to the specific neural system or network the brain regions were involved in. Brain changes were found in pathways responsible for abnormal pain perception, including the classic trigemino-thalamo-cortical system and the lateral and medial pain systems. -

Case Report Endometrial Carcinoma Presenting As Vasculitic Sensorimotor Polyneuropathy
CORE Metadata, citation and similar papers at core.ac.uk Provided by PubMed Central Hindawi Publishing Corporation Case Reports in Obstetrics and Gynecology Volume 2011, Article ID 968756, 3 pages doi:10.1155/2011/968756 Case Report Endometrial Carcinoma Presenting as Vasculitic Sensorimotor Polyneuropathy Marketa Vasku, Thomas Papathemelis, Nicolai Maass, Ivo Meinhold-Heerlein, and Dirk Bauerschlag Department of Gynecology and Obstetrics, University Medical Center Aachen, Pauwelsstraße 30, 52074 Aachen, Germany Correspondence should be addressed to Marketa Vasku, [email protected] Received 10 May 2011; Accepted 15 June 2011 Academic Editors: S. Z. A. Badawy and S.-Y. Ku Copyright © 2011 Marketa Vasku et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. Paraneoplastic syndromes (PNS) are a heterogeneous group of symptoms which are indirectly caused by primary or metastatic tumor. Paraneoplastic polyneuropathy (PNP) is mostly related to small cell lung cancer (5%), prostate, gastric, and breast cancer. Only sporadic cases have been reported to be associated with endometrial cancer. We present a case of a premenopausal woman with severe vasculitic, asymmetric sensorimotor polyneuropathy that developed in conjunction with an endometrial carcinoma responding to surgical therapy of primary tumor combined to steroid therapy. Neurological symptoms such as asymmetrical sensorimotor deficits and painful paresthesias are suspicious when they occur in otherwise healthy women with no medical history. The phenomenon of a paraneoplastic syndrome can point to an underlying malignancy and can be used as marker of progression or regression of the tumor. -

MR Imaging of Wallerian Degeneration in the Brainstem: Temporal Relationships
897 MR Imaging of Wallerian Degeneration in the Brainstem: Temporal Relationships Yuichi Inoue 1 Degeneration of the myelin sheath and axon distal to the most proximal site of axonal Yasumasa Matsumura2 interruption secondary to axonal disease has been called wallerian degeneration. On Teruo Fukuda1 MR imaging, wallerian degeneration of the pyramidal tract can be observed as an Yutaka Nemoto1 abnormal signal intensity, showing prolonged T1 and T2 relaxation times that correspond to the corticospinal tract, with or without shrinkage of the ipsilateral cerebral peduncle Nobuyuki Shirahata3 and pons. Review of MR studies in 150 cases of supratentorial cerebrovascular accidents Tosihisa Suzuki4 1 showed abnormal signal alterations in the ipsilateral brainstem in 33 of the cases. Miyuki Shakudo Abnormal intensity in the ipsilateral brainstem was seen as early as 5 weeks after the 1 Satoshi Yawata supratentorial ictus and was fully evident after 10 weeks in all 33 cases. Signal 2 Shigeko Tanaka alterations were strongest at about 3-6 months when compared with alterations seen Kazumasa Takemoto5 at 10 weeks or even 10 months after the ictus. Shrinkage of the ipsilateral brainstem Yasuto Onoyama 1 appeared as early as 8 months and was demonstrated in all cases 13 months after the ictus. MR seems to be the most effective technique for early detection of wallerian degen eration and may provide insight into its pathophysiological and chemical changes. AJNR 11:897-902, September/October 1990 Wallerian degeneration is the process of disintegration that affects an axon and its myelin sheath after its connection with the cell body has been interrupted [1 ). -

A Current Overview of Diabetic Neuropathy – Mechanisms, Symptoms, Diagnosis, and Treatment
Chapter 5 A Current Overview of Diabetic Neuropathy – Mechanisms, Symptoms, Diagnosis, and Treatment Takashi Kawano Additional information is available at the end of the chapter http://dx.doi.org/10.5772/58308 1. Introduction Diabetic neuropathies are nerve disorders associated with diabetes, which affect approxi‐ mately half of all diabetes patients [1]. The most common complication of diabetes is caused by hyperglycemia which can damage nerve fibers throughout the body [2]. Depending on the types of nerves involved, diabetic neuropathies can be categorized as peripheral, autonomic, proximal, focal neuropathies [3]. Because the pathogenesis mechanisms of diabetic neuropathy remain unknown, numerous studies try to elucidate the underlying mechanisms of this disease. Several reports have demonstrated that a variety of molecules are likely involved in the development of diabetic neuropathy, such as protein kinase C, polyol, aldose reductase, advanced glycation end- products, reactive oxygen species, cytokines [1-10]. Moreover, some risk factors including metabolite, autoimmune, inherited traits and lifestyle, may contribute to the development of diabetic neuropathy. These multiple factors mentioned above might correlate with various symptoms of diabetic neuropathy. These symptoms vary in different organ systems, such as the extremities, digestive system, urinary tract, blood vessels, heart, and sex organs, depending on the nerves affected [9, 10]. The symptoms usually include pain, foot ulcer, dysesthesia, numbness and tingling of extremities, indigestion, nausea, vomiting, diarrhea, facial and eyelid drooping, eyesight change, dizziness, muscle weakness, dysphagia, urinary incontinence, sexual dysfunction, and speech impairment [2, 4, 9-11] The symptoms remain minor initially and develop gradually over years. As a result, the majority of patients do not even realize they are affected until the complications become noticeable or severe. -

The Size and Distribution of Midbrain Dopaminergic Populations Are Permanently Altered by Perinatal Glucocorticoid Exposure in a Sex- Region- and Time-Specific Manner
Neuropsychopharmacology (2007) 32, 1462–1476 & 2007 Nature Publishing Group All rights reserved 0893-133X/07 $30.00 www.neuropsychopharmacology.org The Size and Distribution of Midbrain Dopaminergic Populations are Permanently Altered by Perinatal Glucocorticoid Exposure in a Sex- Region- and Time-Specific Manner Simon McArthur1, Emily McHale1 and Glenda E Gillies*,1 1 Department of Cellular and Molecular Neuroscience, Division of Neuroscience and Mental Health, Imperial College, London, UK Central dopaminergic (DA) systems appear to be particularly vulnerable to disruption by exposure to stressors in early life, but the underlying mechanisms are poorly understood. As endogenous glucocorticoids (GCs) are implicated in other aspects of neurobiological programming, this study aimed to characterize the effects of perinatal GC exposure on the cytoarchitecture of DA populations in the substantia nigra pars compacta (SNc) and the ventral tegmental area (VTA). Dexamethasone was administered non-invasively to rat pups via the mothers’ drinking water during embryonic days 16–19 or postnatal days 1–7, with a total oral intake circa 0.075 or 0.15 mg/ kg/day, respectively; controls received normal drinking water. Analysis of tyrosine hydroxylase-immunoreactive cell counts and regional volumes in adult offspring identified notable sex differences in the shape and volume of the SNc and VTA, as well as the topographical organization and size of the DA populations. Perinatal GC treatments increased the DA population size and altered the shape of the SNc and VTA as well as the organization of the DA neurons by expanding and/or shifting them in a caudal direction. This response was sexually dimorphic and included a feminization or demasculinization of the three-dimensional cytoarchitecture in males, and subtle differences that were dependent on the window of exposure. -

Pilot Longitudinal Study on Post-Stroke Subjects
brain sciences Article Brain Plasticity Mechanisms Underlying Motor Control Reorganization: Pilot Longitudinal Study on Post-Stroke Subjects Marta Gandolla 1,2,* , Lorenzo Niero 1, Franco Molteni 3, Elenora Guanziroli 3 , Nick S. Ward 4,5 and Alessandra Pedrocchi 1,6 1 NearLab@Lecco, Polo Territoriale di Lecco, Politecnico di Milano, Via Gaetano Previati, 1/c, 23900 Lecco, Italy; [email protected] (L.N.); [email protected] (A.P.) 2 Department of Mechanical Engineering, Politecnico di Milano, Via Privata Giuseppe La Masa, 1, 20156 Milano, Italy 3 Villa Beretta Rehabilitation Center, Valduce Hospital, Via N. Sauro, 17, 23845 Costa Masnaga, Italy; [email protected] (F.M.); [email protected] (E.G.) 4 Department of Movement and Clinical Neuroscience, UCL Queen Square Institute of Neurology, London WC1N 3BG, UK; [email protected] 5 The National Hospital for Neurology and Neurosurgery, Queen Square, London WC1N 3BG, UK 6 NearLab, Department of Electronic Information and Bioengineering, Politecnico di Milano, Via Giuseppe Ponzio, 34/5, 20133 Milano, Italy * Correspondence: [email protected] Citation: Gandolla, M.; Niero, L.; Abstract: Functional Electrical Stimulation (FES) has demonstrated to improve walking ability Molteni, F.; Guanziroli, E.; Ward, N.S.; and to induce the carryover effect, long-lasting persisting improvement. Functional magnetic Pedrocchi, A. Brain Plasticity resonance imaging has been used to investigate effective connectivity differences and longitudinal Mechanisms Underlying Motor changes in a group of chronic stroke patients that attended a FES-based rehabilitation program Control Reorganization: Pilot for foot-drop correction, distinguishing between carryover effect responders and non-responders, Longitudinal Study on Post-Stroke and in comparison with a healthy control group. -
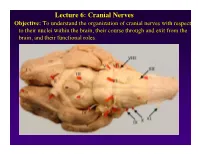
Lecture 6: Cranial Nerves
Lecture 6: Cranial Nerves Objective: To understand the organization of cranial nerves with respect to their nuclei within the brain, their course through and exit from the brain, and their functional roles. Olfactory Eye Muscles 3, 4 &6 Cranial Nerves 1-7 I overview Table, Page 49 II Lecture notes Cranial Nerves and their Functions V Trigeminal VII Facial VIII IX X XII XI Cranial Nerves 8-12 Overview sternocephalic I. Factors Responsible for the Complex Internal Organization of the Brain Stem-> leads to altered location of cranial nerve nuclei in adult brain stem 1. Development of the Fourth Ventricle a. Medulla and Pons develop ventral to the 4th ventricle cerebellum b. Alar plate is displaced lateral to basal plate 4 Medulla Developing Neural Tube 2. Cranial nerve nuclei form discontinuous columns Rostral 12 SE Page 48 Notes 3. Some cranial nerve nuclei migrate from their primitive embryonic positions (e.g., nuclei of V and VII) Facial N. Factors responsible for the complex internal organization of the brainstem: 4) Special senses develop in association with the brain stem. Nuclei of special senses 5) Development of the cerebellum and its connections Cerebellum II. Cranial Nerve Nuclei: Nucleus = column of neuron cell bodies. Efferent nuclei are composed of cell bodies of alpha or gamma motor neurons (SE) or preganglionic parasympathetic neurons (VE). III. Motor Efferent Nuclei (Basal Plate Derivatives): 1. SE (Somatic Efferent) Nuclei: SE neurons form two longitudinally oriented but discontinuous columns of cell bodies in the brain stem. Neurons that comprise these columns are responsible for innervating all of the skeletal musculature of the head. -

The High Yield Neurologic Examination Sadly, I Still Have Nothing New to Disclose Since Tuesday John Engstrom, M.D
Disclosures The High Yield Neurologic Examination Sadly, I still have nothing new to disclose since Tuesday John Engstrom, M.D. August 2018 Medical Chart Quotes Medical Chart Quotes “Exam of the genitalia reveals that he is circus sized.” “While in the ER, She was examined, X- rated and sent home.” 1 Overview – The Neurologic Medical Chart Quotes Examination • Mental status-brief review “Both breasts are equal and reactive • Cranial nerves – common/urgent patterns • Motor exam – common patterns to light and accommodation” • Sensory exam – common patterns • What is wrong with my walking? • Demonstrate the 15 minute exam • Other questions/demonstrations? Screening Mental Status Screening for Visual Field Deficits • Orientation-time, place, person • Visual field screen if you suspect a brain problem • Attention-Digit span forward (nl > 6-7) • Allows you to test function of broad areas of brain – Lobes-occipital, temporal, parietal • Language-repetition, naming, comprehen – Optic nerves, chiasm, optic tracts, and thalamus • Memory-Recall of 3 common objects at 5 • Clinical Importance minutes; if misses an answer give a prompt – “An anatomic sedimentation rate of the brain” • Abstractions-Similarities and differences – Detect abnormalities that require brain imaging (e.g.-apple vs. orange; lake vs. river) – Localize the deficit (right vs. left brain) 2 Screening for Visual Field Deficits- Ambulatory, Cooperative Patient • Imagine visual field cut in four equal pieces • Move examiner finger in the center of each quadrant with patient gaze fixed -

Trigeminal Neuropathy Accompanied by a Pontine Lesion on MRI
□ CASE REPORT □ Trigeminal Neuropathy Accompanied by a Pontine Lesion on MRI Yoichi Ohnuki, Atsushi Mizuma, Tsuyoshi Uesugi and Shunya Takizawa Abstract A 63-year-old man presented with the loss of the sensations of pain and temperature sensation in the right facial region innervated by the trigeminal nerve (V1 to 3). He showed abnormal lesions in the pons and the trigeminal nerve on magnetic resonance imaging (MRI). He had recurrent herpes in the nasal cavity, and a history of left facial palsy. We herein present the unique MRI findings and suggest that herpes simplex infec- tion may cause trigeminal neuropathy. This is the first reported case of dissociated trigeminal neuropathy with herpes simplex infection which was accompanied by a pontine lesion on MRI. Key words: dissociated trigeminal neuropathy, herpes simplex virus, MRI, pontine lesion (Intern Med 55: 1187-1189, 2016) (DOI: 10.2169/internalmedicine.55.5730) port of a patient with dissociated trigeminal sensory neuro- Introduction pathy, which was accompanied by a pontine lesion on MRI. The trigeminal nerve is the largest of the 12 cranial Case Report nerves. It carries the sensory input from the supratentorial dura mater, face, cornea, and the nasal, oral, and sinus mu- A 63-year-old man noticed right palatine numbness after cosa (1). The trigeminal nerve has three main branches dis- the appearance of herpes in his nasal cavity. It spread to his tal to the trigeminal ganglion: the ophthalmic (V1), maxil- right chin, temple and forehead over several days. He was lary (V2), and mandibular (V3) nerves, of which the latter admitted to our hospital on the 14th day after the onset of also carries efferent motor signals to the muscles of mastica- symptoms.