Msk Services Pathway - Low Back Pain Pathology for Patients Aged Over 16 Years
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Universitätsspital Balgrist, Zürich Chiropraktische Medizin Kommissarischer Leiter: Prof
Universitätsspital Balgrist, Zürich Chiropraktische Medizin Kommissarischer Leiter: Prof. Dr. Armin Curt, MD, FRCPC Betreuung der Masterarbeit: Dr. Brigitte Wirth, PT, PhD Leitung der Masterarbeit: Prof. em. Dr. Barry Kim Humphreys, BSc, DC, PhD A SYSTEMATIC REVIEW ON QUANTIFIABLE PHYSICAL RISK FACTORS FOR NON-SPECIFIC ADOLESCENT LOW BACK PAIN MASTERARBEIT zur Erlangung des akademischen Grades Master in Chiropraktischer Medizin (M Chiro Med) der Medizinischen Fakultät der Universität Zürich vorgelegt von Tobias Potthoff (09-712-712) 2017 Table of Content 1. Scientific Accompanying Text .......................................................................................................... 3 2. Abstract ......................................................................................................................................... 13 3. Introduction ................................................................................................................................... 14 4. Methods ........................................................................................................................................ 15 a. Search strategy .......................................................................................................................... 15 b. Inclusion criteria ........................................................................................................................ 15 c. Study selection ......................................................................................................................... -

Injuries and Affections of the Spine ศ.นพ.พิบูลย์ อิทธิระวิวงศ์ ภาควิชาออร์โธปิดิกส์ I
Injuries and Affections of the Spine ศ.นพ.พิบูลย์ อิทธิระวิวงศ์ ภาควิชาออร์โธปิดิกส์ I. Injuries of the spine and thorax :- Classification 1. Major fractures and displacements of the cervical spine - Wedge compression fracture of vertebral body - Burst fracture of vertebral body - Extension subluxation - Flexion subluxation - Dislocation and fracture-dislocation - Fracture of the aieas - Fracture-dislocation of atlanto-axial joint - Intra-spinal displacements of soft tissue 2. Major fractures and displacements of the thoracic and lumbar vertebrae - Wedge compression fracture of vertebral body - Burst fracture of vertebral body - Dislocation and fracture-dislocation 3. Paraplegia from spinal injuries 4. Minor fractures of the spinal column - Fracture of transverse processes - Fracture of spinous processes - Fracture of the sacrum - Fracture of the coccyx 5. Fractures of the thoracic case - Fracture of the ribs - Fracture of the sternum II. Orthopaedic disorders of the spine Disorders Neck and cervical spine Trunk and spine (T,L,S) Congenital - Lumbar and sacral variations, abnormalities Hemivertebra. Spina bifida. Deformities Infantile torticollis Scoliosis. Congenital short neck Kyphosis. Congenital high spcapula Lordosis. Infections of bone Tuberculosis of C-spine Tuberculosis of T or L-spine Pyogenic infection of C- Pyogenic infection of T of L-spine. spine Arthritis of the spinal Ankylosing spondylitis Rheumatoid arthritis Osteoarthritis joints Cervical spondylosis Ankylosing spondylitis Osteochondritis - Scheuermann’s disease Calve’s -
Evicore Spine Imaging Guidelines
CLINICAL GUIDELINES Spine Imaging Policy Version 1.0 Effective February 14, 2020 eviCore healthcare Clinical Decision Support Tool Diagnostic Strategies: This tool addresses common symptoms and symptom complexes. Imaging requests for individuals with atypical symptoms or clinical presentations that are not specifically addressed will require physician review. Consultation with the referring physician, specialist and/or individual’s Primary Care Physician (PCP) may provide additional insight. CPT® (Current Procedural Terminology) is a registered trademark of the American Medical Association (AMA). CPT® five digit codes, nomenclature and other data are copyright 2017 American Medical Association. All Rights Reserved. No fee schedules, basic units, relative values or related listings are included in the CPT® book. AMA does not directly or indirectly practice medicine or dispense medical services. AMA assumes no liability for the data contained herein or not contained herein. © 2019 eviCore healthcare. All rights reserved. Spine Imaging Guidelines V1.0 Spine Imaging Guidelines Procedure Codes Associated with Spine Imaging 3 SP-1: General Guidelines 5 SP-2: Imaging Techniques 14 SP-3: Neck (Cervical Spine) Pain Without/With Neurological Features (Including Stenosis) and Trauma 22 SP-4: Upper Back (Thoracic Spine) Pain Without/With Neurological Features (Including Stenosis) and Trauma 26 SP-5: Low Back (Lumbar Spine) Pain/Coccydynia without Neurological Features 28 SP-6: Lower Extremity Pain with Neurological Features (Radiculopathy, Radiculitis, or Plexopathy and Neuropathy) With or Without Low Back (Lumbar Spine) Pain 32 SP-7: Myelopathy 36 SP-8: Lumbar Spine Spondylolysis/Spondylolisthesis 39 SP-9: Lumbar Spinal Stenosis 42 SP-10: Sacro-Iliac (SI) Joint Pain, Inflammatory Spondylitis/Sacroiliitis and Fibromyalgia 44 SP-11: Pathological Spinal Compression Fractures 47 SP-12: Spinal Pain in Cancer Patients 49 SP-13: Spinal Canal/Cord Disorders (e.g. -

The Effectiveness and Harms of Spinal Manipulative
Effectiveness and Harms of Spinal Manipulative Therapy Evidence-based Synthesis Program for the Treatment of Acute Neck and Lower Back Pain APPENDIX A. SEARCH STRATEGIES 1. SYSTEMATIC REVIEW SEARCH STRATEGIES SEARCH STRATEGY FOR “CHIROPRACTIC” SYSTEMATIC REVIEWS DATABASE SEARCHED: Cochrane Database of Systematic Reviews and Other Reviews NO DATE OR LANGUAGE LIMITATIONS SEARCH STRATEGY: 'chiroprac* in Title, Abstract, Keywords Cochrane Reviews (17) Other Reviews (44) SEARCH STRATEGY: "Manipulation, Spinal" Cochrane Database Search Strategy #2: spine or spinal or neck or back or cervi* and (smt or manipulat* or chiropract*):ti,ab,kw Dates: 2011-present, Limit to the Cochrane Systematic Reviews, Other Reviews (DARE), Technology Assessments, and Economic Evaluations databases. Forward search on: Hurwitz EL, Aker PD, Adams AH, Meeker WC, Shekelle PG. Manipulation and mobilization of the cervical spine. A systematic review of the literature. Spine (Phila Pa 1976). Aug 1 1996;21(15):1746-1759; discussion 1759-1760. 2. UPDATE SEARCH STRATEGIES SPINAL MANIPULATION THERAPY – 2015 UPDATE SEARCH METHODOLOGY DATABASE SEARCHED & TIME PERIOD COVERED: COCHRANE CENTRAL – 1/1/2011-2/06/2017 SEARCH STRATEGY: #1 MeSH descriptor: [Back] explode all trees #2 MeSH descriptor: [Buttocks] this term only #3 MeSH descriptor: [Leg] this term only 54 Effectiveness and Harms of Spinal Manipulative Therapy Evidence-based Synthesis Program for the Treatment of Acute Neck and Lower Back Pain #4 MeSH descriptor: [Back Pain] explode all trees #5 MeSH descriptor: [Back Pain] -

National Imaging Associates, Inc. Clinical Guidelines FACET JOINT
National Imaging Associates, Inc. Clinical guidelines Original Date: July 1, 2015 FACET JOINT INJECTIONS OR BLOCKS Page 1 of 4 “FOR FLORIDA BLUE MEMBERS ONLY” CPT Codes: Last Review Date: May 28, 2015 Cervical/Thoracic Region: 64490 (+ 64491, +64492) Lumbar/Sacral Region: 64493 (+64494, +64495) Medical Coverage Guideline Number: Last Revised Date: 02-61000-30 Responsible Department: Implementation Date: July 2015 Clinical Operations “FOR FLORIDA BLUE MEMBERS ONLY” INTRODUCTION Facet joints (also called zygapophysial joints or z-joints), are posterior to the vertebral bodies in the spinal column and connect the vertebral bodies to each other. They are located at the junction of the inferior articular process of a more cephalad vertebra, and the superior articular process of a more caudal vertebra. These joints provide stability and enable movement, allowing the spine to bend, twist, and extend in different directions. They also restrict hyperextension and hyperflexion. Facet joints are clinically important spinal pain generators in those with chronic spinal pain. Facet joints may refer pain to adjacent structures, making the underlying diagnosis difficult, as referred pain may assume a pseudoradicular pattern. Lumbar facet joints may refer pain to the back, buttocks, and lower extremities while cervical facet joints may refer pain to the head, neck and shoulders. Imaging findings are of little value in determining the source and location of ‘facet joint syndrome’, a term referring to back pain caused by pathology at the facet joints. Imaging studies may detect changes in facet joint architecture, but correlation between radiologic findings and symptoms is unreliable. Although clinical signs are also unsuitable for diagnosing facet joint-mediated pain, they may be of value in selecting candidates for controlled local anesthetic blocks of either the medial branches or the facet joint itself. -

The Erector Spinae Plane Block a Novel Analgesic Technique in Thoracic Neuropathic Pain
CHRONIC AND INTERVENTIONAL PAIN BRIEF TECHNICAL REPORT The Erector Spinae Plane Block A Novel Analgesic Technique in Thoracic Neuropathic Pain Mauricio Forero, MD, FIPP,*Sanjib D. Adhikary, MD,† Hector Lopez, MD,‡ Calvin Tsui, BMSc,§ and Ki Jinn Chin, MBBS (Hons), MMed, FRCPC|| Case 1 Abstract: Thoracic neuropathic pain is a debilitating condition that is often poorly responsive to oral and topical pharmacotherapy. The benefit A 67-year-old man, weight 116 kg and height 188 cm [body of interventional nerve block procedures is unclear due to a paucity of ev- mass index (BMI), 32.8 kg/m2] with a history of heavy smoking idence and the invasiveness of the described techniques. In this report, we and paroxysmal supraventricular tachycardia controlled on ateno- describe a novel interfascial plane block, the erector spinae plane (ESP) lol, was referred to the chronic pain clinic with a 4-month history block, and its successful application in 2 cases of severe neuropathic pain of severe left-sided chest pain. A magnetic resonance imaging (the first resulting from metastatic disease of the ribs, and the second from scan of his thorax at initial presentation had been reported as nor- malunion of multiple rib fractures). In both cases, the ESP block also pro- mal, and the working diagnosis at the time of referral was post- duced an extensive multidermatomal sensory block. Anatomical and radio- herpetic neuralgia. He reported constant burning and stabbing logical investigation in fresh cadavers indicates that its likely site of action neuropathic pain of 10/10 severity on the numerical rating score is at the dorsal and ventral rami of the thoracic spinal nerves. -

Coccydynia: a Story Retold
Open Access Austin Journal of Surgery Special Article - Brain Tumor Surgery Coccydynia: A Story Retold Sarmast AH*, Kirmani AR and Bhat AR Department of Neurosurgery, Sher I Kashmir Institute of Abstract Medical Sciences, India Coccydynia refers to a pathological condition in which pain occurs in the *Corresponding author: Arif Hussain Sarmast, coccyx or its immediate vicinity. The pain is usually provoked by sitting or rising Department of Neurosurgery, Sher I Kashmir Institute of from sitting. Most cases are associated with abnormal mobility of the coccyx, Medical Sciences, Dalipora Kawadara Srinagar Kashmir, which may trigger a chronic inflammatory process leading to degeneration of this India structure. The exact incidence of coccydynia has not been reported; however, factors associated with increased risk of developing coccydynia include obesity Received: May 06, 2016; Accepted: October 20, 2016; and female gender. Several non operative interventions are currently used Published: October 26, 2016 for the management of coccydynia including Non-Steroidal Anti-Inflammatory Drugs (NSAIDs), hot baths, ring-shaped cushions, intrarectal massage and manipulation (manual therapy), steroid injection, dextrose prolotherapy, ganglion impar blocks, pulsed Radio Frequency Thermocoagulation (RFT) and psychotherapy. Several studies have reported good or excellent results after coccygectomy especially in patients who are refractory to conservative treatment. Keywords: Coccydynia; Coccygectomy; Sacrococcygeal joint Introduction those with type I [10]. Anterior subluxation is a rare lesion and tends to occur in type III and type IV patterns. Posterior subluxation is The word ‘coccyx’ has its ancestry from the Greek word used the more common in the straighter type I configuration [11]. beak of the cuckoo bird due to remarkable resemblance in appearance when viewed from the side [1-3]. -

Skeletal System? Skeletal System Chapters 6 & 7 Skeletal System = Bones, Joints, Cartilages, Ligaments
Warm-Up Activity • Fill in the names of the bones in the skeleton diagram. Warm-Up 1. What are the 4 types of bones? Give an example of each. 2. Give 3 ways you can tell a female skeleton from a male skeleton. 3. What hormones are involved in the skeletal system? Skeletal System Chapters 6 & 7 Skeletal System = bones, joints, cartilages, ligaments • Axial skeleton: long axis (skull, vertebral column, rib cage) • Appendicular skeleton: limbs and girdles Appendicular Axial Skeleton Skeleton • Cranium (skull) • Clavicle (collarbone) • Mandible (jaw) • Scapula (shoulder blade) • Vertebral column (spine) • Coxal (pelvic girdle) ▫ Cervical vertebrae • Humerus (arm) ▫ Thoracic vertebrae • Radius, ulna (forearm) ▫ Lumbar vertebrae • Carpals (wrist) • Metacarpals (hand) ▫ Sacrum • Phalanges (fingers, toes) ▫ Coccyx • Femur (thigh) • Sternum (breastbone) • Tibia, fibula (leg) • Ribs • Tarsal, metatarsals (foot) • Calcaneus (heel) • Patella (knee) Functions of the Bones • Support body and cradle soft organs • Protect vital organs • Movement: muscles move bones • Storage of minerals (calcium, phosphorus) & growth factors • Blood cell formation in bone marrow • Triglyceride (fat) storage Classification of Bones 1. Long bones ▫ Longer than they are wide (eg. femur, metacarpels) 2. Short bones ▫ Cube-shaped bones (eg. wrist and ankle) ▫ Sesamoid bones (within tendons – eg. patella) 3. Flat bones ▫ Thin, flat, slightly curved (eg. sternum, skull) 4. Irregular bones ▫ Complicated shapes (eg. vertebrae, hips) Figure 6.2 • Adult = 206 bones • Types of bone -

Pain Pattern Explanation Forms
Pain Pattern Explanation Forms 1. Cervical Facet Pain Pattern 2. Cervical Radicular/Dynatome Pain Pattern 3. Costotransverse Joint Pain Pattern 4. Fibromyalgia Points 5. Hip Joint Pain Pattern 6. Lumbar Dermatomes: Chemical Radiculitis 7. Lumbar Dermatomes: Disc Pathology 8. Lumbar Disc Pathology Healed 9. Lumbar Epidural Fibrosis 10. Lumbar Facet Pain Pattern 11. Lumbar Stenosis 12. Sacroiliac Joint Pain Pattern 13. Thoracic Facet Pain Pattern 14. Upper Cervical Joint Pain Pattern The OEA pain pattern handouts are PDF files that can be used for patient education and marketing. They help you explain your diagnosis with original illustrations that the patients can take home with them. There is limited text so you can tell your explanation of the treatment plan. The pain patterns can be printed in color or black and white. Once purchased, our business card will be replaced with yours to personalize each handout. Each illustration is based on the pain patterns that have been established in books or research articles when available. Normal anatomy and pathoanatomy illustrations are shown for the clinician to explain the diagnosis to the patient and how their treatment can influence the pain generator. These can also be utilized as marketing tools. The following pages are some guidelines that can be utilized to explain the handouts to patients. Cervical Facet Pain Pattern The cervical facet joints are the joints of the neck. Neurophysiologic studies have shown that cervical facet‐joint capsules are sources of neck pain.1 Dwyer et al.2 established pain patterns of the cervical facet joints. o Parasagittal cervical and cervicothoracic pain. -
Digital Motion X-Ray Cervical Spine
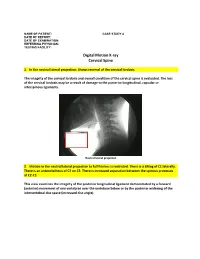
NAME OF PATIENT: CASE STUDY 4 DATE OF REPORT: DATE OF EXAMINATION: REFERRING PHYSICIAN: TESTING FACILITY: Digital Motion X-ray Cervical Spine 1. In the neutral lateral projection: Shows reversal of the cervical lordosis. The integrity of the cervical lordosis and overall condition of the cervical spine is evaluated. The loss of the cervical lordosis may be a result of damage to the posterior longitudinal, capsular or interspinous ligaments. Neutral lateral projection 2. Motion in the neutral lateral projection to full flexion: Is restricted. There is a tilting of C1 laterally. There is an anterolisthesis of C2 on C3. There is increased separation between the spinous processes at C2-C3. This view examines the integrity of the posterior longitudinal ligament demonstrated by a forward (anterior) movement of one vertebrae over the vertebrae below or by the posterior widening of the intervertebral disc space (increased disc angle). Widening of posterior disc space Anterolisthesis The integrity of the interspinous ligament is evaluated in the lateral flexion view. Damage to this ligament results in increased separation of the spinous processes in flexion. Damaged Interspinous Ligament Full flexion projection 3. Motion in the neutral lateral projection to full extension: Is restricted. There is a retrolisthesis of C4 on C5. This view examines the integrity of the anterior longitudinal ligament demonstrated by a backward (posterior) movement of one vertebrae over the vertebrae below or by the anterior widening of the intervertebral disc space (increased disc angle). Retrolisthesis Widening of the anterior disc Full Extension 4. Motion in the oblique flexion projection: Is restricted. There is gapping of the facet joints at C6-C7 bilaterally and C7-T1 bilaterally. -

Relationship Between Endplate Defects, Modic Change, Facet Joint Degeneration, and Disc Degeneration of Cervical Spine
Neurospine 2020;17(2):443-452. Neurospine https://doi.org/10.14245/ns.2040076.038 pISSN 2586-6583 eISSN 2586-6591 Original Article Relationship Between Endplate Corresponding Author Defects, Modic Change, Facet Joint Dong Wuk Son https://orcid.org/0000-0002-9154-1923 Degeneration, and Disc Degeneration Department of Neurosurgery, Pusan of Cervical Spine National University Yangsan Hospital, 20 Geumo-ro, Mulgeum-eup, Yangsan 50612, Su-Hun Lee1,2, Dong Wuk Son1,2, Jun-Seok Lee1,2, Soon-Ki Sung1,2, Sang Weon Lee1,2, Korea Geun Sung Song1,2 E-mail: [email protected] 1Department of Neurosurgery, Pusan National University Yangsan Hospital, Pusan National University School of Medicine, Yangsan, Korea Received: February 11, 2020 2Research Institute for Convergence of Biomedical Science and Technology, Pusan National University Yangsan Revised: February 26, 2020 Hospital, Yangsan, Korea Accepted: February 27, 2020 Objective: The ‘‘disc degeneration precedes facet joint osteoarthritis’’ hypothesis and multi- dimensional analysis were actively discussed in lumbar spine. However, in cervical spine degeneration, the multifactorial analyzes of disc degeneration (DD), Modic changes (Mcs), facet degeneration, and endplate degeneration (ED) is still limited. In this cross-sectional study, we aimed to analyze the prevalence and interrelationship of cervical DD parameters. Methods: We retrospectively recruited 62 patients aged between 60 and 70 years. The disc height, segmental angle, ossified posterior longitudinal ligament (OPLL), ED, facet joint degeneration -

Ossification of the Posterior Longitudinal Ligament: Pathogenesis, Management, and Current Surgical Approaches
Neurosurg Focus 30 (3):E10, 2011 Ossification of the posterior longitudinal ligament: pathogenesis, management, and current surgical approaches A review ZACHARY A. SMITH, M.D.,1 COLIN C. BUCHANAN, M.D.,2 DAN RAPHAEL, P.A.-C.,1 AND LARRY T. KHOO, M.D.1 1Division of Neurosurgery, The Spine Clinic of Los Angeles, Good Samaritan Hospital, An Affiliate Hospital of the University of Southern California Medical School; and 2Department of Neurosurgery, Ronald Reagan–UCLA Medical Center, David Geffen School of Medicine at UCLA, Los Angeles, California Ossification of the posterior longitudinal ligament (OPLL) is an important cause of cervical myelopathy that results from bony ossification of the cervical or thoracic posterior longitudinal ligament (PLL). It has been estimated that nearly 25% of patients with cervical myelopathy will have features of OPLL. Patients commonly present in their mid-40s or 50s with clinical evidence of myelopathy. On MR and CT imaging, this can be seen as areas of ossification that commonly coalesce behind the cervical vertebral bodies, leading to direct ventral compression of the cord. While MR imaging will commonly demonstrate associated changes in the soft tissue, CT scanning will better define areas of ossification. This can also provide the clinician with evidence of possible dural ossification. The surgical management of OPLL remains a challenge to spine surgeons. Surgical alternatives include anterior, posterior, or circumferential decompression and/or stabilization. Anterior cervical stabilization options include cervical corpectomy or multilevel anterior cervical corpectomy and fusion, while posterior stabilization approaches include instrumented or noninstru- mented fusion or laminoplasty. Each of these approaches has distinct advantages and disadvantages.