Norwich University Health Services Operated by Central Vermont
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Applications by College
College Acceptances 2021 The University of Alabama University of New Hampshire-Main Campus American University New Jersey Institute of Technology Bard College The College of New Jersey Belmont University New York Film Academy - New York City Bentley University New York University Binghamton University University of North Carolina Boston Conservatory at Berklee North Carolina State University at Raleigh Boston University Northeastern University California Polytechnic State University Norwich University Carnegie Mellon University Pace University Case Western Reserve University Pennsylvania State University College of Charleston University of Pittsburgh Clark University Plymouth State University Clarkson University Providence College Clemson University SUNY at Purchase College University of Colorado Boulder SUNY at Purchase College University of Colorado Denver Quinnipiac University Colorado School of Mines University of Rhode Island Colorado State University-Fort Collins University of Richmond Columbia University in the City of NY Ringling College of Art and Design Connecticut College Roanoke College University of Connecticut Rochester Institute of Technology Cornell University University of Rochester University of Delaware Roger Williams University Dickinson College Sacred Heart University Drexel University Saint Joseph's University Duquesne University Saint Michael's College East Carolina University School of Visual Arts Elon University Siena College Emerson College University of South Carolina Endicott College University of South Florida-Main -

WHS Profile 2018-19
School Profile Windsor 2018-2019 High School Community Administrative Staff Windsor High School is located in historic Windsor, the Tiffany Cassano Principal birthplace of Vermont. Marked by picturesque Ascutney Colleen DeSchamp Assistant Principal Mountain, WHS welcomes students from Windsor, West Matthew Meagher Dean of Students Windsor, Weathersfield, Hartland, and Cornish, New Hampshire. These Windsor Yellowjackets live and learn in a Terri Hage Administrative Assistant community with a rich history alongside the Connecticut River, Paradise Park - our Town Forest, and unique shopping and dining opportunities downtown and at Artisan’s Park. Guidance Services Terri Herzog School Counselor Greg Pickering School Counselor Colleges Accepted Laurie Brown Registrar by Recent Graduates Admin. Office 802-674-6344 Guidance Services 802-674-8304 Albany College of Pharmacy San Diego State University Fax 802-674-9802 California Polytechnic Inst. Simmons College Castleton University Smith College Champlain College Saint Michael’s College School Dartmouth College Stony Brook University Comprehensive high school for grades 9 –12. Courses not Endicott College Temple University weighted. Fairfield University United States Naval Academy Gordon College Student Enrollment: 234 University of Massachusetts Johnson State College Faculty: 25 Keene State College University of New Hampshire Accreditation: Vermont Agency of Education. Lyndon State College University of Rhode Island Merrimack College University of Southern New York University California Northeastern -

Norwich University Internships Jim Graves, Internship Coordinator (802) 485-2269 [email protected] Career Development Center [email protected]
NORWICH UNIVERSITY™ Expect Challenge. Achieve Distinction. "~ .~F°"' +""".,..,·i}. 2 a~ .. .. i' """'' s..• .,.,..._, +Lt. ~+·', JA .·k) .t ' .,,.t 6 ,1~. ,o·~ ,lll!!i"""' ""~ p0,,,11 ~ , ~ k:rr\ s.1~,1f ...".. ,r S, -4-lr, t ,0\,..., , , ~".) ·; covlJ f'"·; ~ ·, ,~+ tiv-, +L. e··~e,,1e,,.....co· , IP'\, Jl..~e: erc.1.f..°" ... ,..... C.t t c1 ,,.{. f:'!o IL _ L . 1 ' "') cl....... .... ,~~o,,"~.,,......I ttc.... "'"" .·.,, ,_ 1. Will you pay the intern? If so, how much? Wages vary widely from field to field, so be sure yours are competitive or offer competitive incentives. 2. Where will you put the intern? Do you have adequate workspace for them? Will you help make parking arrangements, living arrangements, etc.? 3. What sort of academic background and experience do you want in an intern? Decide on standards for quality beforehand — it’ll help you narrow down the choices and find the best candidates. 4. Who will have the primary responsibility for the intern? Will that person be a mentor or merely a supervisor? 5. What will the intern be doing? Be as specific as possible. Interns, like others in the process of learning, need structure so they don’t become lost, confused or bored. 6. Do you want to plan a program beyond the work you give your interns? Field of study Average hourly wage Business $15.93 Communications $16.00 Computer Sciences $17.20 Engineering $18.26 Sciences $16.60 33 majors total 15 majors=internship courses • Accounting • Biology • Criminal Justice • Political Science • Communications • Psychology • History • Sports -

2011-Summer.Pdf
BOWDOIN MAGAZINE VOL. 82 NO. 2 SUMMER 2011 BV O L . 8 2 N Oow . 2 S UMMER 2 0 1 1 doin STANDP U WITH ASOCIAL FOR THECLASSOF1961, BOWDOINISFOREVER CONSCIENCE JILLSHAWRUDDOCK’77 HARI KONDABOLU ’04 SLICINGTHEPIEFOR THE POWER OF COMEDY AS AN STUDENTACTIVITIES INSTRUMENT FOR CHANGE SUMMER 2011 CONTENTS BowdoinMAGAZINE 24 AGreatSecondHalf PHOTOGRAPHS BY FELICE BOUCHER In an interview that coincided with the opening of an exhibition of the Victoria and Albert’s English alabaster reliefs at the Bowdoin College Museum of Art last semester, Jill Shaw Ruddock ’77 talks about the goal of her new book, The Second Half of Your Life—to make the second half the best half. 30 FortheClassof1961,BowdoinisForever BY LISA WESEL • PHOTOGRAHS BY BOB HANDELMAN AND BRIAN WEDGE ’97 After 50 years as Bowdoin alumni, the Class of 1961 is a particularly close-knit group. Lisa Wesel spent time with a group of them talking about friendship, formative experi- ences, and the privilege of traveling a long road together. 36 StandUpWithaSocialConscience BY EDGAR ALLEN BEEM • PHOTOGRAPHS BY KARSTEN MORAN ’05 The Seattle Times has called Hari Kondabolu ’04 “a young man reaching for the hand-scalding torch of confrontational comics like Lenny Bruce and Richard Pryor.” Ed Beem talks to Hari about his journey from Queens to Brunswick and the power of comedy as an instrument of social change. 44 SlicingthePie BY EDGAR ALLEN BEEM • PHOTOGRAPHS BY DEAN ABRAMSON The Student Activity Fund Committee distributes funding of nearly $700,000 a year in support of clubs, entertainment, and community service. -

Vermont Genetics Network 2018 INSIDE
Vermont Genetics Network 2018 INSIDE: VGN Researcher Awarded NIH AREA Grant Northeast Regional IDeA Conference Highlights VGN Graduate Creates Opportunities For New Students New STEM Course Engages Students VGN Student Gains Coveted Research Position VGN Students Present Research Abroad The Vermont Genetics Network (VGN) is in its third phase of funding About the with a five-year $17.8 million award from the IDeA Networks of Biomedical Research Excellence program of the National Institute of General Medical Vermont Sciences at the National Institutes of Health. The mission of VGN is to build human and physical infrastructure in Vermont for biomedical research. At the lead institution, the University of Vermont, we have developed Genetics state-of-the-art facilities for Proteomics and Bioinformatics to provide to researchers across Vermont the resources they need to carry out world Network class research and compete for federal funding. To address workforce development and its diversity, we build cultures of research by supporting faculty and student research at our Baccalaureate Partner Institutions: Castleton University, Johnson and Lyndon State Colleges, Middlebury College, Norwich University, Saint Michael’s College and Green Mountain College. We also work with students in college lab classes throughout Vermont in order to bring state-of-the-art research resources into their education, including at the Community College of Vermont and Landmark College. JOHNSON STATE COLLEGE LYNDON STATE COLLEGE SAINT MICHAEL’S COLLEGE UNIVERSITY OF VERMONT NORWICH UNIVERSITY MIDDLEBURY COLLEGE CASTLETON UNIVERSITY GREEN MOUNTAIN COLLEGE VGN is funded by the National Institute of General Medical Sciences as part of the National Institutes of Health initiative IDeA Networks of Biomedical Research Excellence (INBRE) under award number P20-GM103449. -

Faculty Faculty Faculty JACQUES N
Faculty Faculty Faculty JACQUES N. BENEAT (2002) Professor of Electrical and Computer Engineering (2015); DEA 1990, Universite Faculty de Brest; Ph.D. 1993 Worcester Polytechnic Institute; Doctorate 1994, Universite de Bordeaux. The year after a name indicates the year hired at Norwich University; the date after the academic title COREY BENNETT (2019) Lecturer of Nursing (2019); indicates the year of that title; the year after each A.S.N. 2011, Castleton State College; B.S.N. 2018, degree indicates the year the degree was earned. University of Vermont; M.S.N. 2019, Norwich University; Registered Nurse. JONATHAN C. ADKINS (2021) Assistant Professor of Cybersecurity (2021); B.S., University of Central KYLIE BLODGETT (2016) Senior Lecturer Physical Florida; M.S., University of Central Florida; Ph.D., Nova Education (2021); B.S. 2010, Norwich University; M.S. Southeastern Univeristy in Ft. Lauderdale, FL. 2011, University of Michigan. M.S. 2015, University of New Hampshire; PhD. 2020, Walden University. MARIE AGAN (2018) Lecturer in Chemistry (2018); B.S. 2011, Saint Michael's College. DAVID J. BLYTHE (1991) Director of the School of Business (2016); Associate Professor of Management DEBORAH AHLERS (1991) Head of Cataloging and (2010); B.S. 1981, Rutgers University; J.D. 1986, Vermont Interlibrary Loan; Assistant Professor (1991); B.A., 1989, Law School. SUNY Binghamton; M.L.S., 1991, SUNY Albany. MATTHEW W. BOVEE (2010) Associate Professor of DANIEL P. ALCORN (2010) Assistant Professor (2020): Computer Science (2019); B.S. 1981, Arizona State A.A. 2008, Kent State University; B.A. 2009, Kent State University; M.A. 1986, The University of Kansas; MSISA University; Program Manager, Bachelor of Science in 2018, Norwich University; Ph.D. -
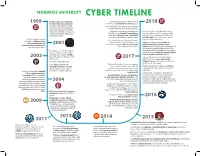
Norwich University Cyber Timeline Nu Pi
NORWICH UNIVERSITY CYBER TIMELINE Bachelor of Science in Computer $3.58 million grant from the NSF for student 1999 Security & Information Assurance scholarships in Scholarship for Service program. 2018 (BSCSIA) program launches. Based Tokyo’s Allied Telesis K.K. partners exclusively with on theory and hands-on experience, Norwich University on cybersecurity services. the program utilizes state-of-the-art forensic tools, offering concentrations Norwich receives two grants totaling over For the third year in a row, Norwich receives a in Advanced Information Assurance $170,549 from the National Security Agency grant from the National Security Agency (NSA) and Digital Forensics. (NSA) and the National Science Foundation and National Science Foundation (NSF) to host (NSF) to host two GenCyber summer camps. GenCyber@NU, a free cybersecurity camp for The NSA designates Norwich At its annual Residency Conference, Norwich’s high school juniors and seniors. University as a National Center College of Graduate and Continuing Studies Norwich University is named a Center of of Academic Excellence in 2001 hosts the second annual Cybersecurity Summit Academic Excellence in Cyber Defense Information Assurance Education featuring international experts. Education (CAE-CDE) by the NSA and Department (CAE-IAE) for the first time. of Homeland Security (DHS) through 2022. The The National Center for the Study of Department of Defense (DoD) Cyber Crime Center Counter-Terrorism and CyberCrime certifies Norwich as a National Center for Digital at Norwich University (later NUARI) is Forensic Academic Excellence (CDFAE). 2002 funded through a U.S. Department of 2017 College of Graduate and Continuing Studies Justice grant. (CGCS) holds the inaugural Cybersecurity NU enters the NSF Cyber Corps. -

Private Higher Education Update During COVID-19 Date: April 10, 2020
To: House Education Committee From: Susan Stitely, President Re: Private Higher Education Update During COVID-19 Date: April 10, 2020 Students Remaining on Campus Although most students are no longer on campus, many international students cannot go home and some U.S-based students without homes are living on campuses. Essential staffs are reporting to work to provide services in dining, buildings and grounds, and campus safety. The colleges are requiring students to observe state restrictions. The total number of students on AVIC member campuses is 609: Champlain College: 130 St. Michael’s College: 126 Bennington College: 116 Norwich University: 100 Middlebury College: 85 Landmark College: 25 VCFA: 10 Sterling College: 9 Marlboro College: 8 Challenges & Success with Remote Learning Technologically, the colleges are doing well with remote learning. Many faculty and students have pivoted to remote learning with resiliency and creativity. The online structure that many colleges already had in place helped facilitate that process. This is particularly true for institutions like Champlain College and Norwich that had strong online studies. However, Vermont’s lack of internet infrastructure is a problem for some of our colleges and is a problem that needs to be addressed by government. For students, broadband access in rural areas is a challenge and can be isolating. Many students at home have weak wifi signals and need printers and other resources. Students have been through a lot this semester including relocating, the cancellation of commencements, and the unexpected transfer to online learning which can be difficult for some students. In addition, focusing on schoolwork from home or far away from campus can be difficult for a variety of reasons. -

College AcceptancesHaverhill High School Students2007Present
College AcceptancesHaverhill High School Students2007Present Acadia University George Mason University Oberlin College The University of Alabama Georgetown University Ohio Northern University Alma College Gordon College University of Ottawa American International College Hampshire College Pace University, New York City American University University of Hartford Pace University, Pleasantville-Briarcliff Anna Maria College Hartwick College Pennsylvania State University, University Arcadia University University of Hawaii at Manoa Park Arizona State University Hawaii Pacific University Philadelphia Biblical University The Art Institute of Boston at Lesley Hesser College University of Pittsburgh University Hiram College Plattsburgh State University Assumption College Hobart and William Smith Colleges Plymouth State University Babson College Hofstra University Point Park University Bard College College of the Holy Cross Prince Edward Island, Univ of Bates College Husson College Providence College Bay State College Iona College Quinnipiac University Becker College Ithaca College Quinsigamond Community College Bentley University Johns Hopkins University Regis College Berklee College of Music Johnson & Wales University Rensselaer Polytechnic Institute Binghamton University Johnson & Wales University University of Rhode Island Boston College Keene State College Rivier College Boston Conservatory La Salle University Rochester Institute of Technology Boston University Lasell College University of Rochester Bowdoin College Lawrence Technological -

Be All That You Can Be: Targeting Library Orientations to Military Cadets
Be All That You Can Be: Targeting Library Orientations to Military Cadets Sarah LeMire First Year Programs Coordinator/Assistant Professor Texas A&M University Libraries [email protected] Stephanie J. Graves Director of Learning and Outreach/Associate Professor Texas A&M University Libraries [email protected] Zackary Chance Medlin Program Assistant Texas A&M University Libraries [email protected] Introduction At Texas A&M University, the Corps of Cadets is the largest and oldest student organization on campus. Each summer, nearly 1,000 freshman recruits participate in the Corps’ Freshman Orientation Week (FOW), a military-style orientation. Buzz cuts, white T-shirts, physical training, and academic success seminars introduce new cadets to life in the Corps and at the university. Due to their participation in FOW, cadets miss out on many other traditional freshman orientation opportunities. In order to reach this large and highly visible freshman cohort, the University Libraries adopted a military-inspired orientation approach that built upon the unique nature of FOW. Librarians strategically used the bonds formed by cadets over the grueling week of FOW by gamifying the presentation, incorporating competition, and relying on the cadets’ sense of camaraderie to create a fun and meaningful experience. This chapter presents a case study on how to target particular audiences in first-year orientations, specifically student cadets. Literature Review Many academic libraries provide orientations and outreach to students on their campuses. However, little has been written about targeted outreach to military-affiliated populations. Recently, librarians have begun developing outreach strategies to serve student veterans, including such efforts as military-themed events and exhibits, partnerships with campus veterans offices, oral history projects, and participation in campus orientations for veterans (Hudson, 2016; LeMire, 2015; LeMire and Mulvihill, 2017; Mills, Paladino, and Klentzin 2015; Samson, 2016; Sojdehei, 2013). -

Master of Business Administration
ONLINE Master of Business Administration LOG IN TO A DISTINGUISHED TRADITION. SINCE 1819. Pictured: Mai Nguyen Khac, Master of Business Administration, 2018 Program Overview PROGRAM MISSION The mission of the Master of Business Administration program is to contribute to Norwich University’s goals by providing high-quality outcomes for graduates in the areas of experiential learning, leadership, creativity, and critical thinking. More than how to succeed in business At Norwich, we believe that people of integrity with a strong moral foundation and personal ethics are needed in business today more than ever. With the complexity of the financial markets, the interconnectedness of our global system and the speed with which modern enterprises adapt to technology, the knowledge and skills acquired in a graduate-level business program are critical. Couple that with the courage to lead and you’ve arrived at something in short supply: the qualities that typify the Norwich MBA. PROGRAM OUTCOMES Students will: The MBA program is structured ■ Have a working knowledge of the key concepts of as follows: strategic resource management, managerial finance, ■ Four start dates per year: March, June, marketing management, operations management, September, and December. and strategic management. ■ Six, eleven-week courses of six credits each. ■ Understand and be able to apply the key concepts used in the primary functional areas of business management. ■ Concentrations of specialized study in: Finance ■ Acquire the critical and creative thinking skills to identify Organizational Leadership business problems and recommend implementable Project Management solutions that meet business objectives. Supply Chain Management ■ Demonstrate an understanding of the process for solving Construction Management business problems and making sound business decisions. -

The Commencement of NORWICH UNIVERSITY
COMMENCEMENT Two Thousand Twenty The Commencement of NORWICH UNIVERSITY Two Thousand Twenty COMMENCEMENT Welcome Provost and Dean of Faculty Sandra G. Affenito National Anthem Regimental Band Invocation Reverend William S. Wick, University Chaplain Greetings President Mark C. Anarumo Conferring of Honorary Degrees President Emeritus Richard W. Schneider President Mark C. Anarumo Commencement Address President Emeritus Richard W. Schneider Response to Address President Mark C. Anarumo Conferring of Degrees President Emeritus Richard W. Schneider Provost and Dean of Faculty Sandra G. Affenito Norwich Forever Norwich forever, queen of the hills When far from thee, still mem’ry thrills recalling Scenes and old friendships, songs, and old cheers Mem’ries that fade not through the changing years Benediction Reverend William S. Wick Closing Remarks President Mark C. Anarumo A Norwich Graduate A university’s legacy can be measured by the impact of its graduates. Norwich University graduates helped to build our In coming to Norwich, today’s graduates nation. From the chief engineer of the first US encountered great challenges. By overcoming transcontinental railroad, to leaders in decisive them, they confirmed in themselves the battles, to the individuals who developed the confidence to persevere in the face of adversity. nation’s banking system, the legacy of Norwich While studying in a rigorous and disciplined reaches back to the most formative decades of academic environment, they acquired invaluable our nation’s History. time management skills as well as practical knowledge and expertise in their chosen fields. More recent graduates have included a president They have been encouraged to think deeply about of NBC and the Chief of Staff of the Army.