Anomalous Origin and Vulnerable Course of Left Colic Artery in Relation to the Pancreas—A Case Report
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

PERIPHERAL VASCULATURE Average Vessel Diameter
PERIPHERAL VASCULATURE Average Vessel Diameter A Trio of Technologies. Peripheral Embolization Solutions A Single Solution. Fathom™ Steerable Guidewires Total Hypotube Tip Proximal/ UPN Length (cm) Length (cm) Length (cm) Distal O.D. Hepatic, Gastro-Intestinal and Splenic Vasculature 24 8-10 mm Common Iliac Artery 39 2-4 mm Internal Pudendal Artery M00150 900 0 140 10 10 cm .016 in 25 6-8 mm External Iliac Artery 40 2-4 mm Middle Rectal M00150 901 0 140 20 20 cm .016 in 26 4-6 mm Internal Iliac Artery 41 2-4 mm Obturator Artery M00150 910 0 180 10 10 cm .016 in 27 5-8 mm Renal Vein 42 2-4 mm Inferior Vesical Artery 28 43 M00150 911 0 180 20 20 cm .016 in 15-25 mm Vena Cava 2-4 mm Superficial Epigastric Artery 29 44 M00150 811 0 200 10 10 cm pre-shaped .014 in 6-8 mm Superior Mesenteric Artery 5-8 mm Femoral Artery 30 3-5 mm Inferior Mesenteric Artery 45 2-4 mm External Pudendal Artery M00150 810 0 200 10 10 cm .014 in 31 1-3 mm Intestinal Arteries M00150 814 0 300 10 10 cm .014 in 32 Male 2-4 mm Superior Rectal Artery A M00150 815 0 300 10 10 cm .014 in 33 1-3 mm Testicular Arteries 1-3 mm Middle Sacral Artery B 1-3 mm Testicular Veins 34 2-4 mm Inferior Epigastric Artery Direxion™ Torqueable Microcatheters 35 2-4 mm Iliolumbar Artery Female 36 2-4 mm Lateral Sacral Artery C 1-3 mm Ovarian Arteries Usable 37 D UPN Tip Shape RO Markers 3-5 mm Superior Gluteal Artery 1-3 mm Ovarian Veins Length (cm) 38 2-4 mm Inferior Gluteal Artery E 2-4 mm Uterine Artery M001195200 105 Straight 1 M001195210 130 Straight 1 M001195220 155 Straight 1 Pelvic -

Redalyc.Accessory Hepatic Artery: Incidence and Distribution
Jornal Vascular Brasileiro ISSN: 1677-5449 [email protected] Sociedade Brasileira de Angiologia e de Cirurgia Vascular Brasil Dutta, Sukhendu; Mukerjee, Bimalendu Accessory hepatic artery: incidence and distribution Jornal Vascular Brasileiro, vol. 9, núm. 1, 2010, pp. 25-27 Sociedade Brasileira de Angiologia e de Cirurgia Vascular São Paulo, Brasil Available in: http://www.redalyc.org/articulo.oa?id=245016483014 How to cite Complete issue Scientific Information System More information about this article Network of Scientific Journals from Latin America, the Caribbean, Spain and Portugal Journal's homepage in redalyc.org Non-profit academic project, developed under the open access initiative ORIGINAL ARTICLE Accessory hepatic artery: incidence and distribution Artéria hepática acessória: incidência e distribuição Sukhendu Dutta,1 Bimalendu Mukerjee2 Abstract Resumo Background: Anatomic variations of the hepatic arteries are com- Contexto: As variações anatômicas das artérias hepáticas são co- mon. Preoperative identification of these variations is important to pre- muns. A identificação pré-operatória dessas variações é importante para vent inadvertent injury and potentially lethal complications during open prevenir lesão inadvertida e complicações potencialmente letais durante and endovascular procedures. procedimentos abertos e endovasculares. Objective: To evaluate the incidence, extra-hepatic course, and Objetivo: Avaliar a incidência, o trajeto extra-hepático e a presen- presence of side branches of accessory hepatic arteries, defined as an ad- ça de ramos laterais das artérias hepáticas acessórias definidas como um ditional arterial supply to the liver in the presence of normal hepatic ar- suprimento arterial adicional para o fígado na presença de artéria hepática tery. normal. Métodos: Oitenta e quatro cadáveres humanos masculinos foram Methods: Eighty-four human male cadavers were dissected using dissecados através de laparotomia mediana transperitoneal. -

Arterial Arcades of Pancreas and Their Variations Chavan NN*, Wabale RN**
International J. of Healthcare and Biomedical Research, Volume: 03, Issue: 02, January 2015, Pages 23-33 Original article: Arterial arcades of Pancreas and their variations Chavan NN*, Wabale RN** [*Assistant Professor, ** Professor and Head] Department of Anatomy, Rural Medical College, PIMS, Loni , Tal. Rahata, Dist. Ahmednagar, Maharashtra, Pin - 413736. Corresponding author: Dr Chavan NM Abstract: Introduction : Pancreas is a highly vascular organ supplied by number of arteries and arterial arcades which provide blood supply to the organ. Arteries contributing to the arterial arcades are celiac and superior mesenteric arteries forming anterior and posterior arcades. These vascular arcades lie upon the surface of the pancreas but also supply the duodenal wall and are the chief obstacles to complete pancreatectomy without duodenectomy. Knowledge of variations of upper abdominal arteries is important while dealing with gastric and duodenal ulcers, biliary tract surgeries and mobilization of the head of the pancreas, as bleeding is one of the complications of these surgeries. During pancreaticoduodenectomies or lymph node resection procedures, these arcades are liable to injuries. Material and methods : Study was conducted on 50 specimens of pancreas removed enbloc from cadavers to study variations in the arcade. Observation and result : Anterior arterial arcade was present in 98% specimens and absent in 2%. It was formed by anterior superior pancreaticoduodenal artery(ASPDA) and anterior inferior pancreaticoduodenal artery(AIPDA) in 92%, Anterior superior pancreaticoduodenal artery (ASPDA), Anterior inferior pancreaticoduodenal artery (AIPDA) and Right dorsal pancreatic artery (Rt.DPA) in 2%, Anterior superior pancreaticoduodenal artery (ASPDA) only in 2%, Anterior superior pancreaticoduodenal artery (ASPDA) and Posterior inferior pancreaticoduodenal artery (PIPDA) in 2%, Arcade was absent and Anterior superior pancreaticoduodenal artery (ASPDA) gave branches in 2%. -

Colon Operative Standards
282 SECTION IV | COLON F G E F FIGURE 16-7 (Continued). patients with hereditary nonpolyposis colon cancer, as they have a higher incidence of synchronous and metachronous colonic tumors than do patients with sporadic colorectal cancer. As calculated by life table analysis, the risk for metachronous cancer among patients with hereditary nonpolyposis is as high as 40% at 10 years. Simi- larly, for colon cancer patients with familial adenomatous polyposis, surgical resec- tion should consist of either total abdominal colectomy or total proctocolectomy. The choice between these two operations depends on the burden of polypoid disease in the rectum and the patient’s preference for close surveillance. 7,8,9 Finally, individuals who develop colon cancer in the setting of long-standing ulcerative colitis require a total proctocolectomy. The oncologic principles of colon cancer surgery as outlined in this chapter, including the attention to surgical margins and the need for proximal vascular ligation, should be adhered to bilaterally, not just for the portion of colon in which the tumor has been identifi ed.10,11 3. PROXIMAL VASCULAR LIGATION AND REGIONAL LYMPHADENECTOMY Recommendation: Resection of the tumor-bearing bowel segment and radical lymphadenectomy should be performed en bloc with proximal vascular ligation at the origin of the primary feeding vessel(s). Copyright © 2015 Wolters Kluwer Health, Inc. Unauthorized reproduction of the article is prohibited. 226_ACS_Ch16.indd6_ACS_Ch16.indd 228282 44/3/15/3/15 22:58:58 AAMM CHAPTER 16 | Colon Resection 283 Type of Data: Prospective and retrospective observational studies. Strength of Recommendation: Moderate. Rationale The standard of practice for the treatment of stage I to III (nonmetastatic) colon can- cer is complete margin-negative resection (R0 resection) of the tumor-bearing bowel combined with en bloc resection of the intact node-bearing mesentery (i.e., regional lymphadenectomy). -

Parts of the Body 1) Head – Caput, Capitus 2) Skull- Cranium Cephalic- Toward the Skull Caudal- Toward the Tail Rostral- Toward the Nose 3) Collum (Pl
BIO 3330 Advanced Human Cadaver Anatomy Instructor: Dr. Jeff Simpson Department of Biology Metropolitan State College of Denver 1 PARTS OF THE BODY 1) HEAD – CAPUT, CAPITUS 2) SKULL- CRANIUM CEPHALIC- TOWARD THE SKULL CAUDAL- TOWARD THE TAIL ROSTRAL- TOWARD THE NOSE 3) COLLUM (PL. COLLI), CERVIX 4) TRUNK- THORAX, CHEST 5) ABDOMEN- AREA BETWEEN THE DIAPHRAGM AND THE HIP BONES 6) PELVIS- AREA BETWEEN OS COXAS EXTREMITIES -UPPER 1) SHOULDER GIRDLE - SCAPULA, CLAVICLE 2) BRACHIUM - ARM 3) ANTEBRACHIUM -FOREARM 4) CUBITAL FOSSA 6) METACARPALS 7) PHALANGES 2 Lower Extremities Pelvis Os Coxae (2) Inominant Bones Sacrum Coccyx Terms of Position and Direction Anatomical Position Body Erect, head, eyes and toes facing forward. Limbs at side, palms facing forward Anterior-ventral Posterior-dorsal Superficial Deep Internal/external Vertical & horizontal- refer to the body in the standing position Lateral/ medial Superior/inferior Ipsilateral Contralateral Planes of the Body Median-cuts the body into left and right halves Sagittal- parallel to median Frontal (Coronal)- divides the body into front and back halves 3 Horizontal(transverse)- cuts the body into upper and lower portions Positions of the Body Proximal Distal Limbs Radial Ulnar Tibial Fibular Foot Dorsum Plantar Hallicus HAND Dorsum- back of hand Palmar (volar)- palm side Pollicus Index finger Middle finger Ring finger Pinky finger TERMS OF MOVEMENT 1) FLEXION: DECREASE ANGLE BETWEEN TWO BONES OF A JOINT 2) EXTENSION: INCREASE ANGLE BETWEEN TWO BONES OF A JOINT 3) ADDUCTION: TOWARDS MIDLINE -
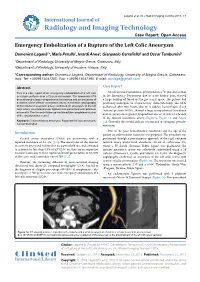
Emergency Embolization of a Rupture of the Left Colic Aneurysm
Laganà et al. Int J Radiol Imaging Technol 2015, 1:1 International Journal of Radiology and Imaging Technology Case Report: Open Access Emergency Embolization of a Rupture of the Left Colic Aneurysm Domenico Laganà1*, Maria Petullà1, Ierardi Anna2, Gianpaolo Carrafiello2 and Oscar Tamburrini1 1Department of Radiology, University of Magna Grecia, Catanzaro, Italy 2Department of Radiology, University of Insubria, Varese, Italy *Corresponding author: Domenico Laganà, Department of Radiology, University of Magna Grecia, Catanzaro, Italy, Tel: +3909613647285, Fax: +3909613647395, E-mail: [email protected] Abstract Case Report This is a case report of an emergency embolization of a left colic An ultrasound examination, performed on a 72-year-old woman aneurysm performed on a 72-year-old woman. The abdominal CTA in the Emergency Department due to acute lumbar pain, showed scan showed a large retroperitoneal hematoma and an aneurysm of a large buildup of blood in the pre-sacral space. The patient had a branch of the inferior mesenteric artery. A selective angiography previously undergone to a laparoscopic cholecystectomy. The CTA, of the inferior mesenteric artery confirmed an aneurysm of the left performed after two hours, due to a sudden hemorrhagic shock colic artery. An endovascular ligation was performed with platinum (arterial pressure 90/50), showed a large retroperitoneal hematoma microcoils. The 3-month follow-up confirmed the complete exclusion of the aneurysmatic vessel. and an aneurysm at greater longitudinal axis of 18 mm of a branch of the inferior mesenteric artery (Figure1a, Figure 1b and Figure Keywords: Visceral artery aneurysm, Ruptured left colic aneurysm, 1c). Generally this would indicate a traumatic or iatrogenic pseudo- Coil embolization aneurysm. -

Concurrent Origin of Right Gastroepiploic and Left Colic Arteries from Inferior Pancreaticoduodenal Artery: Rare Variation of Splanchnic Anastomosis
DOI: 10.5958/2319-5886.2015.00142.3 International Journal of Medical Research & Health Sciences www.ijmrhs.com Volume 4 Issue 3 Coden: IJMRHS Copyright @2015 ISSN: 2319-5886 Received: 27th Apr 2015 Revised: 10th May 2015 Accepted: 25th May 2015 Case report CONCURRENT ORIGIN OF RIGHT GASTROEPIPLOIC AND LEFT COLIC ARTERIES FROM INFERIOR PANCREATICODUODENAL ARTERY: RARE VARIATION OF SPLANCHNIC ANASTOMOSIS *Mutalik Maitreyee M Assistant Professor, Department of Anatomy, MIMER Medical College, Talegaon Dabhade, Pune, India *Corresponding author email: [email protected] ABSTRACT In the present case, inferior pancreaticoduodenal artery, the first branch of superior mesenteric artery, was exceptionally giving rise to right gastroepiploic artery and left colic artery simultaneously. Right gastroepiploic artery is a branch of foregut artery, while left colic artery is a branch of hindgut artery. Concurrent origin of branches of foregut as well as hindgut arteries from a midgut artery i.e. superior mesenteric artery is very rare. Usual left colic artery from inferior mesenteric artery was also present but was supplying smaller area than usual. It can be explained as persistence of unusual channels and obliteration of usual ones along the dorsal splanchnic anastomosis during the embryonic development. The field of vascularization of superior mesenteric artery was extended beyond its usual boundaries both proximally as well as distally, which is clinically important as unawareness of the variations may lead to significant morbidity and mortality. Keywords: Bypass graft, Colic artery, Gastroepiploic artery, Pancreaticoduodenal artery, Splanchnic anastomosis, Mesenteric artery INTRODUCTION Fields of vascularization of celiac trunk (CT), gastroduodenal artery (GDA), arising from hepatic superior mesenteric artery (SMA), and inferior branch of CT (foregut artery). -

Dorsal Pancreatic Artery—A Study of Its Detailed Anatomy for Safe Pancreaticoduodenectomy
Indian Journal of Surgery (February 2021) 83(1):144–149 https://doi.org/10.1007/s12262-020-02255-2 ORIGINAL ARTICLE Dorsal Pancreatic Artery—a Study of Its Detailed Anatomy for Safe Pancreaticoduodenectomy T Tatsuoka1 & TNoie2 & TNoro1 & M Nakata3 & HYamada4 & Y Harihara2 Received: 29 October 2019 /Accepted: 24 April 2020 /Published online: 155 May 2020 # The Author(s) 2020 Abstract Early division of the dorsal pancreatic artery (DPA) or its branches to the uncinate process during pancreaticoduodenectomy (PD) in addition to early division of the gastroduodenal artery and inferior pancreaticoduodenal artery should be performed to reduce blood loss by completely avoiding venous congestion. However, the significance of early division of DPA or its branches to the uncinate process has not been reported. The aim of this study was to investigate the anatomy of DPA and its branches to the uncinate process using the currently available high-resolution dynamic computed tomography (CT) as the first step to investigate the significance of DPA in the artery-first approach during PD. Preoperative dynamic thin-slice CT data of 160 consecutive patients who underwent hepato–pancreato–biliary surgery were examined focusing on the anatomy of DPA and its branches to the uncinate process. DPAwas recognized in 103 patients (64%); it originated from the celiac axis or its branches in 70 patients and from the superior mesenteric artery or its branches in 34 patients. The branches to the uncinate process were visualized in 82 patients (80% of those with DPA), with diameters of 0.5–1.5 mm in approximately 80% of the 82 patients irrespective of DPA origin. -

SŁOWNIK ANATOMICZNY (ANGIELSKO–Łacinsłownik Anatomiczny (Angielsko-Łacińsko-Polski)´ SKO–POLSKI)
ANATOMY WORDS (ENGLISH–LATIN–POLISH) SŁOWNIK ANATOMICZNY (ANGIELSKO–ŁACINSłownik anatomiczny (angielsko-łacińsko-polski)´ SKO–POLSKI) English – Je˛zyk angielski Latin – Łacina Polish – Je˛zyk polski Arteries – Te˛tnice accessory obturator artery arteria obturatoria accessoria tętnica zasłonowa dodatkowa acetabular branch ramus acetabularis gałąź panewkowa anterior basal segmental artery arteria segmentalis basalis anterior pulmonis tętnica segmentowa podstawna przednia (dextri et sinistri) płuca (prawego i lewego) anterior cecal artery arteria caecalis anterior tętnica kątnicza przednia anterior cerebral artery arteria cerebri anterior tętnica przednia mózgu anterior choroidal artery arteria choroidea anterior tętnica naczyniówkowa przednia anterior ciliary arteries arteriae ciliares anteriores tętnice rzęskowe przednie anterior circumflex humeral artery arteria circumflexa humeri anterior tętnica okalająca ramię przednia anterior communicating artery arteria communicans anterior tętnica łącząca przednia anterior conjunctival artery arteria conjunctivalis anterior tętnica spojówkowa przednia anterior ethmoidal artery arteria ethmoidalis anterior tętnica sitowa przednia anterior inferior cerebellar artery arteria anterior inferior cerebelli tętnica dolna przednia móżdżku anterior interosseous artery arteria interossea anterior tętnica międzykostna przednia anterior labial branches of deep external rami labiales anteriores arteriae pudendae gałęzie wargowe przednie tętnicy sromowej pudendal artery externae profundae zewnętrznej głębokiej -
Variations in the Origin and Colic Branches of the Superior Mesenteric Artery
VARIATIONS IN THE ORIGIN AND COLIC BRANCHES OF THE SUPERIOR MESENTERIC ARTERY Dissertation Submitted to THE TAMIL NADU DR. M.G.R. MEDICAL UNIVERSITY CHENNAI in partial fulfillment of the regulations for the award of the degree of M.S. (Anatomy) BRANCH - V THE TAMILNADU DR. M.G.R. MEDICAL UNIVERSITY CHENNAI, INDIA. MARCH 2008 Certificate This is to certify that the dissertation title, ‘Variations in the Origin and Colic branches of the Superior Mesenteric Artery’ is an original work done by Dr. M. Nirmaladevi, PG Student, Stanley Medical College, Chennai-1, under my supervision and guidance. Dr. Mythili Bhaskaran, M.D., Dr. Sudha Seshayyan, M.S., Dean Professor and HOD Stanley Medical College Department of Anatomy Chennai-1 Stanley Medical College Chennai-1 Place: Chennai-1 Date: DECLARATION I solemnly declare that this dissertation "Variations in the Origin and Colic branches of the Superior Mesenteric Artery" was written by me in the Department of Anatomy, Govt. Stanley Medical College and Hospital, Chennai, under the guidance and supervision of Prof. Dr. Sudha Seshayyan, M.S., Professor and Head of the Department of Anatomy, Govt. Stanley Medical College, Chennai - 600 001. This dissertation is submitted to The Tamil Nadu Dr. M.G.R. Medical University, Chennai in partial fulfillment of the University regulations for the award of degree of M.S. Anatomy - Branch V examinations to be held in March 2008. Place : Chennai. Date : (Dr.M.Nirmala Devi) ACKNOWLEDGEMENT I have been overwhelmed by the support and guidance that I have received from a large number of people in completing this study and I would like to take this opportunity to thank each one of them. -

Nodal Drainage Pathways in Primary Rectal Cancer: Anatomy of Regional and Distant Nodal Spread
Abdominal Radiology (2019) 44:3527–3535 https://doi.org/10.1007/s00261-019-02094-0 SPECIAL SECTION: RECTAL CANCER Nodal drainage pathways in primary rectal cancer: anatomy of regional and distant nodal spread Harmeet Kaur1 · Randy D. Ernst1 · Gaiane M. Rauch1 · Mukesh Harisinghani2 Published online: 18 October 2019 © Springer Science+Business Media, LLC, part of Springer Nature 2019 Abstract Nodal involvement is a signifcant prognostic factor in rectal cancer and difcult to assess preoperatively. An understanding of the patterns of nodal spread from diferent regions of the rectum can assist in this process and is essential for the purposes of surgical planning. In this article we defne patterns of spread to mesenteric and pelvic sidewall nodal subgroups and discuss the importance of accurate anatomic localization of nodes for the purposes of staging and surgical planning. Keywords Rectal cancer · Rectal adenocarcinoma · Lymph node · MRI · CT Introduction The anatomic defnition of the rectum specifes its supe- rior or upper extent as the point of coalescence of the taenia Lymph node spread is an important prognostic factor in rec- to form a continuous outer longitudinal muscle layer in the tal cancer. An understanding of lymphatic drainage path- rectum. Inferiorly the anatomic rectum ends at the dentate ways from diferent regions of the rectum, the most common line, which also is the point of transition between columnar nodal groups’ involved and accurate localization of these epithelium lining the rectum and the squamous epithelium nodes to mesenteric, pelvic sidewall and retroperitoneal lining the anatomic anal canal, which extends down from the compartments is important in the accurate staging and sur- dentate line to the anal verge [1]. -

Unusual Pancreatico-Mesenteric Vasculature: a Clinical Insight
Clinical Group Archives of Anatomy and Physiology DOI http://dx.doi.org/10.17352/aap.000001 ISSN: 2640-7957 CC By Shikha Singh, Jasbir Kaur, Jyoti Arora*, Renu Baliyan Jeph, Vandana Research Article Mehta and Rajesh Kumar Suri Unusual Pancreatico-Mesenteric Department of Anatomy, Vardhman Mahavir Medical College and Safdarjung Hospital, Ansari Nagar West, Delhi 110029, India Vasculature: A Clinical Insight Dates: Received: 09 November, 2016; Accepted: 03 December, 2016; Published: 06 December, 2016 *Corresponding author: Jyoti Arora, MBBS, MS, Abstract Professor, Department of Anatomy, Vardhman Mahavir Medical College and Safdarjung Hospital, Background: Awareness about the variable vascular anatomy of superior mesenteric artery is Ansari Nagar West, New Delhi, Delhi 110029, India, imperative for appropriate clinical management. Present study not only augments anatomical literature Tel: +91-99-99077775; Fax: +91-11-2375365; E-mail: pertaining to mesenteric vasculature but also adds to the clinical acumen of medical practitioners in their clinical endeavors. Keywords: Superior mesenteric artery; Anomalous Case summary: The present study reports the occurrence of anomalous branch, termed as branch; Inferior pancreatic artery; Inferior accessory inferior pancreatic artery stemming from superior mesenteric artery. Additionally inferior pancreaticoduodenal artery; Ventral splanchnic pancreaticoduodenal artery was seen to be dividing into right and left branches instead of usual anterior arteries and posterior branches. Right branch terminated