Cardiovascular Disease Recurrence and Long-Term Mortality in a Tri
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Michael Marmot Secretary in Your Lifetime? I Have a Dog in This Fight
BMJ CONFIDENTIAL Bevan or Lansley? Who was the best and the worst health Michael Marmot secretary in your lifetime? I have a dog in this fight. The best was Alan Johnson: Evidence based optimist we share a passion for reducing health inequalities. He commissioned me to do the Marmot Review, which we published as Fair Society, Healthy Lives . It has proved to be a great way to work with local authorities, Public Health England, and many others on social determinants of health. Stephen Dorrell used his experience as health secretary to be an independent minded and analytical chair of the Health Select Committee. The worst? A crowded field. Who is the person you would most like to thank and why? I believe, and evidence supports it, that good work requires a good home life and vice versa. I most want to MICHAEL MARMOT , 70, is the doyen of thank my wife and three children. health inequalities, both in research and To whom would you most like to apologise? policy. He led a groundbreaking study of When I toddled off to Buckingham Palace to receive Whitehall civil servants that showed, contra- an award, I kept thinking that it should have been Jerry ry to traditional thinking, that the lower their Morris [Scottish epidemiologist] and Geoffrey Rose. Jerry status, the worse their health—the “social rang me and said, “ We have come in from the cold.” gradient.” His conviction that evidence should If you were given £1m what would you spend it on? form the basis of policy and that people can I was given a lot of money once and established the make a diff erence led to his chairing two WHO commissions and the English review on Balzan Fellowships—bringing young scholars to UCL from social determinants of health. -
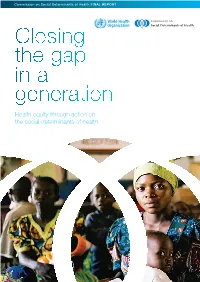
Closing the Gap in a Generation Health Equity Through Action on the Social Determinants of Health Closing the Gap in a Generation Contents
Commission on Social Determinants of Health FINAL REPORT Closing the gap in a generation Health equity through action on the social determinants of health CLOSING THE GAP IN A GENERATION CONTENTS WHO Library Cataloguing-in- © World Health Organization 2008 whatsoever on the part of the World Health All reasonable precautions have been taken Publication Data Organization concerning the legal status of by the World Health Organization to verify All rights reserved. Publications of the World any country, territory, city or area or of its the information contained in this publication. Closing the gap in a generation : health equity Health Organization can be obtained from authorities, or concerning the delimitation of its However, the published material is being through action on the social determinants WHO Press, World Health Organization, 20 frontiers or boundaries. Dotted lines on maps distributed without warranty of any kind, either of health : final report of the commission on Avenue Appia, 1211 Geneva 27, Switzerland represent approximate border lines for which expressed or implied. The responsibility for social determinants of health. (tel.: +41 22 791 3264; fax: +41 22 791 there may not yet be full agreement. the interpretation and use of the material lies 4857; e-mail: [email protected]). Requests with the reader. In no event shall the World 1.Socioeconomic factors. 2.Health care for permission to reproduce or translate The mention of specific companies or of Health Organization be liable for damages rationing. 3.Health services accessibility. WHO publications – whether for sale or for certain manufacturers’ products does not arising from its use. 4.Patient advocacy. -

1/11/2006 Health in an Unequal World Michael Marmot This Is a Lightly
1/11/2006 Health in an Unequal World Michael Marmot This is a lightly edited version of the (October) 2006 Harveian Oration at the Royal College of Physicians. It will be published in Clinical Medicine and the Lancet. In poor countries, tragically, people die unnecessarily. In rich countries, too, the higher death rate of those in less fortunate social positions is unnecessary. Can there be a link between these two phenomena: inequalities in health among countries and inequalities within? Surely, it might be argued, the depredations of grinding poverty – lack of food, shelter, clean water, and basic medical care or public health – that ravage the lives of the poor in developing countries are different in kind from the way that social disadvantage leads to poor health in modern Britain, for example. The diseases of the slums of Nairobi are, to be sure, different in kind from the diseases that affect the disadvantaged in east London or Harlem, and have different proximate causes. There is, however, a link. The unnecessary disease and suffering of the disadvantaged, whether in poor countries or rich, is a result of the way we organise our affairs in society. I shall argue, in this oration, that failing to meet the fundamental human need of autonomy, empowerment, or human freedom is a potent cause of ill-health. In making this case, I shall bring together two rather disparate streams of work. The first is a report of my own research endeavour. I have sought explanations for the social gradient in health, as observed in the Whitehall studies, pointing to the fundamental importance of the circumstances in which people live and work. -

To Govern the Health Or to Make the Bills of Mortality - This Is the Question for Public Health in Poland
PRZEGL EPIDEMIOL 2013; 67: 651 - 660 Public health Dorota Cianciara TO GOVERN THE HEALTH OR TO MAKE THE BILLS OF MORTALITY - THIS IS THE QUESTION FOR PUBLIC HEALTH IN POLAND School of Public Health, The Centre of Postgraduate Medical Education, Warsaw National Institute of Public Health – National Institute of Hygiene, Warsaw ABSTRACT In the article important moments in the development of public health at the global scale were presented, as- suming that postwar evolution proceeded in two fundamental phases: the first – events which occurred to the proclamation of the Ottawa Charter and introduction of ‘new public health’ and the second – situations reported after Ottawa to the present time. The current challenges for public health in Poland were also discussed. It was proposed to differentiate two dimensions of public health capacity: internal (ad intra), which is with regard to the power centre, condition within the environment and external (ad extra), which refers to the relation with surroundings and population and enables to deliver sustain services and programmes. The possible strategies aiming at increasing ad intra capacity were also indicated. Key words: public health, health promotion, history, forecasting, capacity building In Poland, the theoretic, demonstrative and dis- INTRODUCTION cursive papers are hardly present. Furthermore, some papers which are available are of questionable quality. Health is of too high priority to be left for physi- The forums concerning ideas exchange, confronting the cians and public’s health is too crucial to be in charge of opinions, correcting the mistakes are also lacking. Not public health officers only. In Poland, the public health enough studies are conducted and the ones which are lesson has not been studied so scrupulously as it was carried out are the exemplification of biomedical and done in more developed countries. -

Professor Sir Michael Marmot
Professor Sir Michael Marmot The degree of Doctor of Medicine (honoris causa) was conferred upon Professor Sir Michael Marmot at the Faculty of Medicine's 150th birthday celebrations held on 13 June 2006. Chancellor the Hon Justice Kim Santow conferring the honorary degree upon Professor Marmot, photo, courtesy Faculty of Medicine. Citation Chancellor, I have the honour to present Professor Sir Michael Marmot for admission to the degree of Doctor of Medicine, honoris causa. Sir Michael Marmot is a social epidemiologist of rare repute - indeed a founding father of that discipline. He has pioneered the academic study of how society influences health, particularly cardiovascular health, and of health inequalities both within and between countries. He chairs The World Health Organization Commission on Social Determinants of Health, which will report this year. The social and biological factors which Sir Michael has already identified as causes of disease and mortality have been as unexpected as they are preventable. The famous ‘Whitehall studies’ which he led showed that the higher people progressed in the hierarchy of the British civil service, the better their cardiac health and life expectancy - much better. The studies turned conventional wisdom about ‘executive stress’ upside down. He argues that limited personal autonomy and poor social participation are killers, acting via endocrine and metabolic pathways. This has major implications for political and corporate management policies, not to mention ‘participation policies’ for an aging population. Our leaders would do well to read his book called ‘Status Syndrome’. He is a distinguished graduate of this University. But the Medical Faculty’s 1968 Senior Year Book records, curiously, that Michael Marmot was born in 1945 and ‘became educated in 1966’. -

Social Determinants of Health Inequalities
Social Determinants of Health Inequalities Michael Marmot Professor of Epidemiology and Public Health, International Centre for Health and Society, University College London, 1-19 Torrington Place London WC1E 6BT UK e-mail: [email protected] Michael Marmot is chairman of the Commission on Social Determinants of Health Acknowledgements: Grateful thanks to Ruth Bell, Hilary Brown, Tim Evans, Alec Irwin, Rene Loewenson, Nicole Valentine, Jeanette Vega, and members of the WHO Equity team who have worked to develop the Commission and the concepts in this paper. Abstract: The gross inequalities in health that we see within and between countries present a challenge to the world. That there should be a spread of life expectancy of 48 years among countries and 20 years or more within countries is not inevitable. A burgeoning volume of research identifies social factors at the root of much of these inequalities in health. Social determinants are relevant to communicable and non- communicable disease alike. Health status, therefore, should be of concern to policy makers in every sector, not solely those involved in health policy. As a response to this global change, WHO is launching a Commission on Social Determinants of Health, which will review the evidence, raise societal debate, and recommend policies with the goal of improving health of the word’s most vulnerable people. A major thrust of the Commission is turning public-health knowledge into political action. 1 There are gross inequalities in health between countries. Life expectancy at birth, to take one measure, ranges from 34 in Sierra Leone to 81.9 in Japan. -

Review of Social Determinants and the Health Divide in the WHO European Region: Final Report
reprintUpdated 2014 Review of social determinants social of Review The World Health Organization World Health Organization (WHO) is a specialized agency Regional Office for Europe of the United Nations created in UN City 1948 with the primary responsibility Marmorvej 51 for international health matters and DK-2100 Copenhagen Ø public health. The WHO Regional Denmark Office for Europe is one of six regional offices throughout the Tel.: +45 45 33 70 00 world, each with its own programme Fax: +45 45 33 70 01 geared to the particular health E-mail: [email protected] conditions of the countries it serves. Web site: www.euro.who.int Review of social determinants Member States Albania Andorra and the health divide in Armenia Austria Azerbaijan Belarus and the health divide in the WHO European Region: WHO the European in divide health the and the WHO European Region: Belgium Bosnia and Herzegovina Bulgaria Croatia Cyprus final report Czech Republic Denmark Estonia Finland France Georgia Germany Greece Hungary Iceland Ireland Israel Italy Kazakhstan Kyrgyzstan Latvia Lithuania Luxembourg Malta Monaco Montenegro Netherlands Norway Poland Portugal Republic of Moldova Romania Russian Federation San Marino Serbia Slovakia Slovenia Spain Sweden final report final Switzerland Tajikistan The former Yugoslav Republic of Macedonia Turkey Turkmenistan Ukraine United Kingdom Uzbekistan panos pictures | cover photo: bjoern steinz WHO-UCL SDH 2014 final full cover PRESS 260514.indd 1 26/05/2014 09:48 WHO-UCL SDH 2014 final full cover PRESS 260514.indd 2 26/05/2014 09:48 Review of social determinants and the health divide in the WHO European Region: final report Review chair Michael Marmot Report prepared by UCL Institute of Health Equity Abstract The WHO European Region has seen Keywords remarkable health gains in populations that Health inequities have experienced progressive improvements Health management and planning in the conditions in which people are born, Health status disparities grow, live and work. -
Sir Michael Marmot
International Balzan Foundation Sir Michael Marmot 2004 Balzan Prize for Epidemiology Excerpt from Premi Balzan 2004. Laudationes, discorsi, saggi, Milan, 2005 (revised and enlarged edition, 2012) This publication has been re-issued on the occasion of the Annual Balzan Lecture 2012 at the University of Zurich, 29 August 2012, an initiative derived from the Agreements on Collaboration between the International Balzan Foundation “Prize”, the Swiss Academies of Arts and Sciences, and the Accademia Nazionale dei Lincei. © 2012, Fondazione Internazionale Balzan, Milano [www.balzan.org] Printed in Italy CONTENTS Michael Marmot, 2004 Balzan Prize for Epidemiology Prize Citation and Laudatio 5 Prizewinner’s Acceptance Speech at the Awards Ceremony 18 November 2004 at the Accademia Nazionale dei Lincei, Rome 7 Social Determinants of Health: A Panoramic View A panoramic synthesis of his career, drawn up by Michael Marmot, on the occasion of the 2004 Awards Ceremony 9 Research Project – Abstract 19 Biographical and bibliographical data 23 International Balzan Foundation 25 Michael Marmot 2004 Balzan Prize for Epidemiology Prize Citation and Laudatio Sir Michael Marmot has made seminal contributions to epidemiology by establishing hitherto unsuspected links between social status and differences in health and life expectancy. He has initiated the era of social epidemiology and paved the way for the development of a wholly new concept of preventive medicine. Sir Michael Marmot has revolutionized epidemiology by establishing hith- erto unsuspected links between differences in health and life expectancy on the one hand, and social status on the other. In comparative studies of Japanese migrants in Hawaii and in California and of migrants from the Indian subcontinent to Great Britain, Sir Michael Marmot discovered the importance of a change in sociocultural environment relative to that of the associated change in habits – dietary, alcohol, smoking – in bringing about biological changes associated with an increase in cardiovascular morbid- ity and mortality. -

Health Equity in England : the Marmot Review 10 Years On
HEALTH EQUITY IN ENGLAND: THE MARMOT REVIEW 10 YEARS ON HEALTH EQUITY IN ENGLAND: THE MARMOT REVIEW 10 YEARS ON HEALTH EQUITY IN ENGLAND: THE MARMOT REVIEW 10 YEARS ON 1 Note from the Chair AUTHORS Report writing team: Michael Marmot, Jessica Allen, Tammy Boyce, Peter Goldblatt, Joana Morrison. The Marmot Review team was led by Michael Marmot and Jessica Allen and consisted of Jessica Allen, Matilda Allen, Peter Goldblatt, Tammy Boyce, Antiopi Ntouva, Joana Morrison, Felicity Porritt. Peter Goldblatt, Tammy Boyce and Joana Morrison coordinated production and analysis of tables and charts. Team support: Luke Beswick, Darryl Bourke, Kit Codling, Patricia Hallam, Alice Munro. The work of the Review was informed and guided by the Advisory Group and the Health Foundation. Suggested citation: Michael Marmot, Jessica Allen, Tammy Boyce, Peter Goldblatt, Joana Morrison (2020) Health equity in England: The Marmot Review 10 years on. London: Institute of Health Equity HEALTH FOUNDATION The Health Foundation supported this work and provided insight and advice. IHE would like to thank in particular: Jennifer Dixon, Jo Bibby, Jenny Cockin, Tim Elwell Sutton, Grace Everest, David Finch Adam Tinson, Rita Ranmal. AUTHORS’ ACKNOWLEDGEMENTS We are indebted to the Advisory Group that informed the review: Torsten Bell, David Buck, Sally Burlington, Jabeer Butt, Jo Casebourne, Adam Coutts, Naomi Eisenstadt, Joanne Roney, Frank Soodeen, Alice Wiseman. We are also grateful for advice and insight from the Collaboration for Health and Wellbeing. We are grateful for advice and input from Nicky Hawkins, Frameworks Institute; Angela Donkin, NFER; and Tom McBride, Early Intervention Foundation for comments on drafts. -

The Cost of Greed
Book Two The Cost of Greed Originally published in Greed and Good: Understanding and Overcoming the Inequality That Limits Our Lives by Sam Pizzigati (Apex Press/Rowman & Littlefield, 2004). For more, see Inequality.org. THE PRICE WE PAY FOR INEQUALITY IF THOSE WHO FAWN OVER FORTUNES were right, if letting wealth accu- mulate were indeed the prime prescription for a healthy, vigorous soci- ety, we ought today to be enjoying a new American golden age. Never before, after all, have grand fortunes accumulated as prodigiously as they have over recent decades, at least not in modern times. Our econ- omy, given this awesome accumulation, ought to be vibrant, full of opportunity at every turn. Our enterprises should be generating wealth at extraordinary rates. We ourselves ought to be feeling stoked and energetic, confident that our hard work will be duly rewarded. Compassion ought to be flowing for the unfortunate, the arts ought to be blooming. We should be feeling absolutely terrific about ourselves and our country. But we aren’t. So what went wrong? What really happens when societies stand back and let great wealth accumulate in the pockets of a few? What has inequality cost us? The pages ahead will search for answers to these questions, in places both self-evident and somewhat surprising. We’ll explore the worksites where we labor and the neighborhoods where we live. We’ll look at our families and our friendships. We’ll examine what makes us happy and what makes us sick. We’ll probe why our professions no longer leave us proud, why our pastimes no longer bring us pleasure. -

0001Hrs Wednesday 30Th June, 2021 All Media Enquiries: Felicity Porritt [email protected] 07739 419219
EMBARGO: 0001hrs Wednesday 30th June, 2021 All media enquiries: Felicity Porritt [email protected] 07739 419219 New bold & ambitious framework to reduce inequities & build back fairer for future generations “If Government is serious about levelling up, here’s how to do it”, says Marmot The leading global institute on health inequalities – the UCL Institute of Health Equity (IHE) – has published a new framework, which includes new bold and ambitious recommendations on how to reduce health inequities and build back fairer from the COVID-19 pandemic for future generations. The Framework is part of a new Marmot Review and comes as life expectancy falls for everyone across the UK, and health inequities widen, at a cost of £39 billion every year. The new Review, published today 30th June, was commissioned by the Greater Manchester Health and Social Care Partnership. The City Region had a 25% higher COVID-19 death rate than England as a whole in the 13 months to March 2021. This high death rate contributed to a decline in life expectancy in the North West region, which was larger than the average in England. Life expectancy fell in 2020 by 1.6 years for men and 1.2 years for women in the North West compared 1.3 years and 0.9 years, respectively, across England. Commenting, the IHE’s Director, Professor Sir Michael Marmot, said if the government is serious about levelling up health inequities, equity of health and wellbeing must be at the heart of government and business strategy rather narrow economic goals: “Greater Manchester has high levels of avoidable health inequalities as a result of longstanding economic and social inequities, and as across the country, ethnic disadvantage. -

Public Health Classics Economic And
Public Health Classics This section looks back to some ground-breaking contributions to public health, reproducing them in their original form and adding a commentary on their significance from a modern-day perspective. To complement the theme of this month’s Bulletin, Michael Marmot comments on the 1985 paper by Geoffrey Rose on the study of the determinants of disease in individuals and in populations. The original paper is reproduced by permission of The International Journal of Epidemiology. Economic and social determinants of disease Michael Marmot1 Blessed, or burdened, with a traditional medical Armed with an individual difference approach education, doctors are taught that the individual to disease one might argue that a population patient has priority. The ethical and just action is that characterized by a high rate of disease must have a which benefits the individual patient. What is, high prevalence of high-risk individuals; and con- undoubtedly, a blessing for patients may be a burden versely for a low-risk population. Someone arguing the for public health. Expanding the clinical role to environmental case might cite the high rate of embrace prevention commonly means focusing on childhood illness in an area without a clean water the individual. This may include advice to pregnant supply as evidence against this individual focus. Such women and young mothers, detection of risk factors, loose thinking would not convince the scientist with and counselling on behaviour change in middle age, the individual focus who could point out that infected or detection of early disease and decrements in water would not be a cause of illness if individuals did functioning at older ages.