UNICEF Cameroon Situation Report Reporting Period: August 28–September 27, 2012
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
PCD LAGDO.Pdf
REPUBLIQUE DU CAMEROUN REPUBLIC OF CAMEROON Paix – Travail – Patrie Peace-Work-Fatherland ********* *********** MINISTERE DE L’ADMINISTRATION MINISTRY OF TERRITORIAL TERRITORIALE ET DE LA ADMINISTRATION DECENTRALISATION AND DECENTRALISATION *********** *********** REGION DU NORD NORTH REGION *********** *********** DEPARTEMENT DE LA BENOUE BENUE DIVISION *********** *********** COMMUNE DE LAGDO LADGO COUNCIL *********** *********** PLAN COMMUNAL DE DEVELOPPEMENT D E L A G D O PLANIFICATION COMMUNALE AVEC L’APPUI DU PNDP juin 2015 Programme National de Développement Participatif (PNDP)-Cellule Régionale de Coordination du Nord -Tél : 22 27 10 70 / 98 49 89 91 – E Mail : [email protected]– Site Web : www.pndp.org g i SOMMAIRE SOMMAIRE ......................................................................................................................................................... ii RESUME DU PCD ................................................................................................................................................ vi LISTE DES ABBREVIATIONS ............................................................................................................................... vii LISTE DES TABLEAUX ......................................................................................................................................... xii LISTE DES PHOTOS ........................................................................................................................................... xiii LISTE DES CARTES -
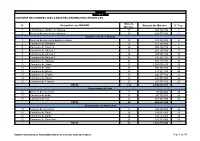
De 40 MINMAP Région Du Nord SYNTHESE DES DONNEES SUR LA BASE DES INFORMATIONS RECUEILLIES
MINMAP Région du Nord SYNTHESE DES DONNEES SUR LA BASE DES INFORMATIONS RECUEILLIES Nbre de N° Désignation des MO/MOD Montant des Marchés N° Page Marchés 1 Communauté Urbaine de Garoua 11 847 894 350 3 2 Services déconcentrés régionaux 20 528 977 000 4 Département de la Bénoué 3 Services déconcentrés départementaux 10 283 500 000 6 4 Commune de Barndaké 13 376 238 000 7 5 Commune de Bascheo 16 305 482 770 8 6 Commune de Garoua 1 11 201 187 000 9 7 Commune de Garoua 2 26 498 592 344 10 8 Commune de Garoua 3 22 735 201 727 12 9 Commune de Gashiga 21 353 419 404 14 10 Commune de Lagdo 21 2 026 560 930 16 11 Commune de Pitoa 18 360 777 700 18 12 Commune de Bibémi 18 371 277 700 20 13 Commune de Dembo 11 300 277 700 21 14 Commune de Ngong 12 235 778 000 22 15 Commune de Touroua 15 187 777 700 23 TOTAL 214 6 236 070 975 Département du Faro 16 Services déconcentrés 5 96 500 000 25 17 Commune de Beka 15 230 778 000 25 18 Commune de Poli 22 481 554 000 26 TOTAL 42 808 832 000 Département du Mayo-Louti 19 Services déconcentrés 6 196 000 000 28 20 Commune de Figuil 16 328 512 000 28 21 Commune de Guider 28 534 529 000 30 22 Commune de Mayo Oulo 24 331 278 000 32 TOTAL 74 1 390 319 000 MINMAP / DIVISION DE LA PROGRAMMATION ET DU SUIVI DES MARCHES PUBLICS Page 1 de 40 MINMAP Région du Nord SYNTHESE DES DONNEES SUR LA BASE DES INFORMATIONS RECUEILLIES Nbre de N° Désignation des MO/MOD Montant des Marchés N° Page Marchés Département du Mayo-Rey 23 Services déconcentrés 7 152 900 000 35 24 Commune de Madingring 14 163 778 000 35 24 Commune de Rey Bouba -

Cameroon : Adamawa, East and North Rgeions
CAMEROON : ADAMAWA, EAST AND NORTH RGEIONS 11° E 12° E 13° E 14° E N 1125° E 16° E Hossere Gaval Mayo Kewe Palpal Dew atan Hossere Mayo Kelvoun Hossere HDossere OuIro M aArday MARE Go mbe Trabahohoy Mayo Bokwa Melendem Vinjegel Kelvoun Pandoual Ourlang Mayo Palia Dam assay Birdif Hossere Hosere Hossere Madama CHARI-BAGUIRMI Mbirdif Zaga Taldam Mubi Hosere Ndoudjem Hossere Mordoy Madama Matalao Hosere Gordom BORNO Matalao Goboum Mou Mayo Mou Baday Korehel Hossere Tongom Ndujem Hossere Seleguere Paha Goboum Hossere Mokoy Diam Ibbi Moukoy Melem lem Doubouvoum Mayo Alouki Mayo Palia Loum as Marma MAYO KANI Mayo Nelma Mayo Zevene Njefi Nelma Dja-Lingo Birdi Harma Mayo Djifi Hosere Galao Hossere Birdi Beli Bili Mandama Galao Bokong Babarkin Deba Madama DabaGalaou Hossere Goudak Hosere Geling Dirtehe Biri Massabey Geling Hosere Hossere Banam Mokorvong Gueleng Goudak Far-North Makirve Dirtcha Hwoli Ts adaksok Gueling Boko Bourwoy Tawan Tawan N 1 Talak Matafal Kouodja Mouga Goudjougoudjou MasabayMassabay Boko Irguilang Bedeve Gimoulounga Bili Douroum Irngileng Mayo Kapta Hakirvia Mougoulounga Hosere Talak Komboum Sobre Bourhoy Mayo Malwey Matafat Hossere Hwoli Hossere Woli Barkao Gande Watchama Guimoulounga Vinde Yola Bourwoy Mokorvong Kapta Hosere Mouga Mouena Mayo Oulo Hossere Bangay Dirbass Dirbas Kousm adouma Malwei Boulou Gandarma Boutouza Mouna Goungourga Mayo Douroum Ouro Saday Djouvoure MAYO DANAY Dum o Bougouma Bangai Houloum Mayo Gottokoun Galbanki Houmbal Moda Goude Tarnbaga Madara Mayo Bozki Bokzi Bangei Holoum Pri TiraHosere Tira -

Emergency Appeal Operation Update Cameroon: Floods
Emergency appeal operation update Cameroon: Floods Emergency appeal n° MDRCM014 GLIDE n° FL-2012-000157-CMR Operation update n°1 19 November, 2012 Period covered by this Ops Update: 6 September to 31 October, 2012. Appeal target (current): CHF 1,637,316. Appeal coverage: 18%; not including DREF allocation and yet-to-be-confirmed pledges. <Click here to go directly to the updated donor response report; here for interim financial here to link to contact details > Appeal history: This Emergency Appeal was initially launched on 28 September, 2012 for CHF 1,637,314 for 12 months to assist about 25,000 beneficiaries. Disaster Relief Emergency Fund (DREF): CHF 299,707 was initially allocated from the Federation’s DREF to Cameroon Red Cross volunteers constructing emergency latrines in support the national society to respond. Northern Cameroon with assistance from members of the floods affected community / Photo by Cameroon Red Cross Summary: Beginning the second half of August 2012, widespread heavy rain in Cameroon caused severe flooding, especially in North, and Far North regions. IFRC helped the Cameroon Red Cross to obtain DREF funds in order to assist the affected populations in the North and Far North Regions. Considering the magnitude of the situation, this DREF was transformed into an emergency appeal. Funds raised through this emergency appeal, in addition to those of the DREF, have so far enabled the Cameroon Red Cross to build 170 emergency shelters for internally displaced persons (IDPs), build 26 emergency latrines, distribute non-food items to 921 families, treat 198 wells and provide first aid to flood victims in the two regions. -

Cameroon: Cholera 21 April, 2010
DREF operation n° DRMDRCM007 GLIDE n° EP-2009-000021-CM Cameroon: Cholera 21 April, 2010 The International Federation of Red Cross and Red Crescent (IFRC) Disaster Relief Emergency Fund (DREF) is a source of un-earmarked money created by the Federation in 1985 to ensure that immediate financial support is available for Red Cross Red Crescent response to emergencies. The DREF is a vital part of the International Federation’s disaster response system and increases the ability of National Societies to respond to disasters. Summary: CHF 203,419 was allocated from the IFRC’s Disaster Relief Emergency Fund (DREF) on 26 October, 2009 to support the Cameroon Red Cross national society in delivering assistance to some 800,000 beneficiaries. Twenty health districts were hit by a cholera outbreak in the North and Far North regions of Cameroon in October 2009. The funds allocated from DREF enabled the Cameroon Red Cross National Society to train 495 volunteers who in turn conducted health education in the various neighbourhoods affected. In addition, the identified cholera cases were referred to the nearest health centres. The trained volunteers also distributed sanitation materials which were used to disinfect latrines, treat water Cameroon Red Cross volunteers covered water wells with metal roofing sheets to prevent them from being contaminated/ Viviane points, clean gutters and organise Nzeusseu/IFRC cleanliness days in the market places of the affected localities. In addition, buckets with covers and taps were distributed to restaurants in the affected localities for clients to wash their hands. Red Cross volunteers also distributed metal roofing sheets to cover latrines and water wells, and chemicals for disinfecting water. -

Cameroon Humanitarian Situation Report
Cameroon Humanitarian Situation Report ©UNICEF Cameroon/2019 SITUATION IN NUMBERS Highlights August 2019 2,300,000 • More than 118,000 people have benefited from UNICEF’s # of children in need of humanitarian assistance humanitarian assistance in the North-West and South-West 4,300,000 regions since January including 15,800 in August. # of people in need (Cameroon Humanitarian Needs Overview 2019) • The Rapid Response Mechanism (RRM) strategy, Displacement established in the South-West region in June, was extended 530,000 into the North-West region in which 1,640 people received # of Internally Displaced Persons (IDPs) in the North- WASH kits and Long-Lasting Insecticidal Nets (LLINs) in West and South-West regions (OCHA Displacement Monitoring, July 2019) August. 372,854 # of IDPs and Returnees in the Far-North region • In August, 265,694 children in the Far-North region were (IOM Displacement Tracking Matrix 18, April 2019) vaccinated against poliomyelitis during the final round of 105,923 the vaccination campaign launched following the polio # of Nigerian Refugees in rural areas (UNHCR Fact Sheet, July 2019) outbreak in May. UNICEF Appeal 2019 • During the month of August, 3,087 children received US$ 39.3 million psychosocial support in the Far-North region. UNICEF’s Response with Partners Total funding Funds requirement received Sector Total UNICEF Total available 20% $ 4.5M Target Results* Target Results* Carry-over WASH: People provided with 374,758 33,152 75,000 20,181 $ 3.2 M access to appropriate sanitation 2019 funding Education: Number of boys and requirement: girls (3 to 17 years) affected by 363,300 2,415 217,980 0 $39.3 M crisis receiving learning materials Nutrition**: Number of children Funding gap aged 6-59 months with SAM 60,255 39,727 65,064 40,626 $ 31.6M admitted for treatment Child Protection: Children reached with psychosocial support 563,265 160,423 289,789 87,110 through child friendly/safe spaces C4D: Persons reached with key life- saving & behaviour change 385,000 431,034 messages *Total results are cumulative. -

Cameroon Page 1 of 19
Cameroon Page 1 of 19 Cameroon Country Reports on Human Rights Practices - 2004 Released by the Bureau of Democracy, Human Rights, and Labor February 28, 2005 Cameroon is a republic dominated by a strong presidency. Despite the country's multiparty system of government, the Cameroon People's Democratic Movement (CPDM) has remained in power since the early years of independence. In October, CPDM leader Paul Biya won re-election as President. The primary opposition parties fielded candidates; however, the election was flawed by irregularities, particularly in the voter registration process. The President retains the power to control legislation or to rule by decree. He has used his legislative control to change the Constitution and extend the term lengths of the presidency. The judiciary was subject to significant executive influence and suffered from corruption and inefficiency. The national police (DGSN), the National Intelligence Service (DGRE), the Gendarmerie, the Ministry of Territorial Administration, Military Security, the army, the civilian Minister of Defense, the civilian head of police, and, to a lesser extent, the Presidential Guard are responsible for internal security; the DGSN and Gendarmerie have primary responsibility for law enforcement. The Ministry of Defense, including the Gendarmerie, DGSN, and DRGE, are under an office of the Presidency, resulting in strong presidential control of internal security forces. Although civilian authorities generally maintained effective control of the security forces, there were frequent instances in which elements of the security forces acted independently of government authority. Members of the security forces continued to commit numerous serious human rights abuses. The majority of the population of approximately 16.3 million resided in rural areas; agriculture accounted for 24 percent of gross domestic product. -

Proceedingsnord of the GENERAL CONFERENCE of LOCAL COUNCILS
REPUBLIC OF CAMEROON REPUBLIQUE DU CAMEROUN Peace - Work - Fatherland Paix - Travail - Patrie ------------------------- ------------------------- MINISTRY OF DECENTRALIZATION MINISTERE DE LA DECENTRALISATION AND LOCAL DEVELOPMENT ET DU DEVELOPPEMENT LOCAL Extrême PROCEEDINGSNord OF THE GENERAL CONFERENCE OF LOCAL COUNCILS Nord Theme: Deepening Decentralization: A New Face for Local Councils in Cameroon Adamaoua Nord-Ouest Yaounde Conference Centre, 6 and 7 February 2019 Sud- Ouest Ouest Centre Littoral Est Sud Published in July 2019 For any information on the General Conference on Local Councils - 2019 edition - or to obtain copies of this publication, please contact: Ministry of Decentralization and Local Development (MINDDEVEL) Website: www.minddevel.gov.cm Facebook: Ministère-de-la-Décentralisation-et-du-Développement-Local Twitter: @minddevelcamer.1 Reviewed by: MINDDEVEL/PRADEC-GIZ These proceedings have been published with the assistance of the German Federal Ministry for Economic Cooperation and Development (BMZ) through the Deutsche Gesellschaft für internationale Zusammenarbeit (GIZ) GmbH in the framework of the Support programme for municipal development (PROMUD). GIZ does not necessarily share the opinions expressed in this publication. The Ministry of Decentralisation and Local Development (MINDDEVEL) is fully responsible for this content. Contents Contents Foreword ..............................................................................................................................................................................5 -
NZB Newsletter
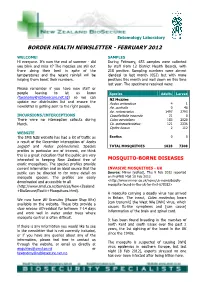
Entomology Laboratory BORDER HEALTH NEWSLETTER - FEBRUARY 2012 WELCOME! SAMPLES Hi everyone. It’s now the end of summer - did During February, 653 samples were collected you blink and miss it? The mozzies are still out by staff from 12 District Health Boards, with there doing their best in spite of the 218 positive. Sampling numbers were almost temperatures and the recent rainfall will be identical to last month (652) but with more helping them boost their numbers. positives this month and well down on this time last year. The specimens received were: Please remember if you have new staff or people leaving to let us know Species Adults Larvae ([email protected]) so we can NZ Mozzies update our distribution list and ensure the Aedes antipodeus 4 1 newsletter is getting sent to the right people. Ae. australis 0 46 Ae. notoscriptus 1497 2793 INCURSIONS/INTERCEPTIONS Coquillettidia iracunda 21 0 There were no interception callouts during Culex pervigilans 183 2020 March. Cx. quinquefasciatus 121 2336 Opifex fuscus 2 112 WEBSITE The SMS NZB website has had a lot of traffic as Exotics 0 0 a result of the December interception of Aedes aegypti and Aedes polynesiensis. Species TOTAL MOSQUITOES 1828 7308 profiles in particular are of interest, we think this is a great indication that the public are very interested in keeping New Zealand free of MOSQUITO-BORNE DISEASES exotic mosquitoes. The species profiles provide current information and an ideal source that the INVASIVE MOSQUITOES - UK public can be directed to for more detail on Source: Mirror [edited], Thu 9 Feb 2012 reported mosquito species. -

Consideration of Reports Submitted by States Parties Under Article 19 of the Convention
United Nations CAT/C/CMR/4 Convention against Torture Distr.: General 5 August 2009 and Other Cruel, Inhuman English or Degrading Treatment Original: French or Punishment Committee against Torture Consideration of reports submitted by States parties under article 19 of the Convention Fourth periodic report of States parties due in 2000 Cameroon* ** [27 November 2008] * For the third periodic report, see CAT/C/34/Add.17; for its consideration by the Committee on 18, 19 and 20 November 2003, see CAT/C/SR.585, 588 and 590. ** The annexes to the present report may be consulted in the files of the secretariat. GE.09-44036 (E) 141209 231209 CAT/C/CMR/4 Contents Abbreviations and acronyms Chapter Paragraphs Page Introduction............................................................................................................. 1–2 4 I. New information on the general framework for implementation of the Convention in domestic law.................................................................................... 3–20 4 A. Normative measures ....................................................................................... 4–9 4 B. Institutional measures..................................................................................... 10–20 6 II. Responses to the Committee’s recommendations................................................... 21–147 8 A. Response of the State of Cameroon to the recommendations in paragraph 8 of the Committee’s concluding observations.............................. 21–81 8 B. Response of the State of Cameroon -

Monthly Humanitarian Situation Report CAMEROON Date: 27Th May 2013
Monthly Humanitarian Situation Report CAMEROON Date: 27th May 2013 Highlights The Health and Nutrition week (SASNIM) was organized in the 10 regions from 26 to 30 April; 1,152,045 children aged 6-59 months received vitamin A and 1,349,937 children aged 12-59 months were dewormed in the Far North and North region. 1,727,391 (101%) children under 5 received Polio drops (OPV), and 38,790 pregnant women received Intermittent Preventive treatment (IPT). A mass screening of acute malnutrition in the North and Far North region was carried out during [the Mother and Child Health and Nutrition Action Week (SASNIM), reaching 90% of children. Out of 1,420,145 children 6-59 months estimated to be covered, 1,288,475 children were enrolled in the mass screening with MUAC, 425,892 in the North region and 862,583 in the Far North. 50,583 MAM cases and 9,269 SAM cases were found and referred to outpatient centres. 10 health districts out of 43 require urgent action. A 10 member delegation led by the UN Foundation team consisting of US Congressional aides and Rotary International visited Garoua - North Region to look at Child Survival and HIV initiatives from April 27 – May 2nd 2013. Following the declaration of state of emergency on May 14 in Nigeria, the actions carried out by Nigerian Government towards the Boko Haram rebels in Maiduguru State (neighbor of Cameroon) may lead to displacement of population from Nigeria to Cameroun. Some Cameroonians living near Nigeria Borno State are moving into Far North region of Cameroon. -

N.Pmruixior Uurrrm DIRECTION DES RESSOURCES RESOURCES HUMAINES
REPUBLIQUE DU CAMEROUN Rf,PUBLTC OF CAMEROON Paix-Travail-Patrie Peace.Work-Fatherlând MINISTERE DE L'EDUCATION DE MINISTRY OF BASIC EDUCATION BASE GENERAL SECRETARIAT SECRETARIAT Gf,NERAL n.pmruixior uurrrm DIRECTION DES RESSOURCES RESOURCES HUMAINES TROISIEME PROGRAMME DE CONTRACTUALISATION DES INSTITUTEURS AU MINISTERE DE L'EDUCATION DE BASE DEUXIEME OPERATION AU TITRE DE L'EXERCICE 2O2O usrE DEs EcoLEs NECESSTTEUSES (JOB POSTING ) REGION DU NORD N" REGION DEPARTEMENT ARRONDISSEMENT NOM DE L'ECOLE 1 NORD BENOUE BASCHEO ECOLE PUBLIQUE DE BASCHEO 2 NORD BEN OU E BASCHEO EP BANTAYE-BASCH EO 3 NORD BE NOU E BASCHEO EP BARGOUMA 4 NORD BENOUE BASCHEO EP BOMBOL 5 NORD BENOU E BASCHEO EP DARAM 6 NORD BE NOU E BASCHEO EP DARPATA 7 NORD BE NOU E BASCHEO EP DJALINGO.BELEL 8 NORD BEN OU E BASCHEO EP DJAOURO-MOUSSA 9 NORD BEN OU E BASCHEO EP DJARENGOL 10 NORD BEN OU E BASCHEO EP DORBA 11 NORD B ENOU E BASCHEO EP FOULBERE 72 NORD BENOUE BASCHEO EP GASSIRE -15 NORD B ENOU E BASCHEO EP HAMAKOUSSOU 14 NORD B ENOU E BASCHEO EP HAMAYEL 15 NORD BENO U E BASCHEO EP HARKOU NORD BENOUE BASCHEO EP KATAKO 17 NORD 8 ENOU E BASCHEO EP KATCHATCHIA 18 NORD BENOUE BASCHEO EP KERZING 19 NORD BENOUE EASCHEO EP KOBOSSI 20 NORD B ENOU E BASCHEO EP LARIA 2t NORD BENOUE BASCHEO EP MALKOUROU NORD BENOU E BASCHEO EP MAPOUTKI 23 NORD BENOUE BASCHEO EP MAYO-OULO-FALI 24 NORD BENOUE BASCHEO EP MBABI 25 NORD BENOUE BASCHEO EP MBOULMI 26 NORD BENOUE BASCHEO EP NARO-KOUBADJE 27 NORD 8 ENOU E BASCHEO EP NASSARAO 28 NORD BENOUE BASCHEO EP NGOUROU-DABA 29 NORD BENOUE BASCHEO EP