Skin Disorders Affecting the Feet
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Idiopathic Spiny Keratoderma: a Report of Two Cases and Literature Review
Idiopathic Spiny Keratoderma: A Report of Two Cases and Literature Review Jessica Schweitzer, DO,* Matthew Koehler, DO,** David Horowitz, DO*** *Intern, Largo Medical Center, Largo, FL **Dermatology Resident, Third Year, College Medical Center/Western University, Long Beach, CA ***Dermatology Residency Program Director, College Medical Center/Western University, Long Beach, CA Abstract Spiny keratoderma is a rare and likely underreported condition that presents with punctate hyperkeratotic growths localized to the palms and soles. We present two cases of clinically diagnosed spiny keratoderma. Although the lesions were asymptomatic, patients are at risk of an underlying internal malignancy with this condition, so diagnosis is crucial. Neither men were seeking treatment for the lesions when they were discovered, suggesting that this condition may be much more common than reported. Patients with histories of manual labor, increased UV exposure, and non-melanoma skin cancer (NMSC) may also be at higher risk for developing spiny keratoderma.1 The epidemiology, histopathologic features, differential diagnosis, and current treatments for spiny keratoderma are reviewed. Introduction Case 2 enthusiast for his entire life, spending significant Spiny keratoderma is a rare palmoplantar A 67-year-old Caucasian male presented with a time using his hands to maintain and fire his keratoderma that presents with keratotic, pinpoint one-year history of insidiously growing, pinpoint weapons and many hours outside without sun papules on the palms and soles. There are both hyperkeratotic papules projecting from his palms protection. The patient was referred back to his hereditary and acquired forms. When found, bilaterally (Figures 4-5). He presented to the clinic primary care physician for internal evaluation. -

Smelly Foot Rash
CLINICAL Smelly foot rash Paulo Morais Ligia Peralta Keywords: skin diseases, infectious Case study A previously healthy Caucasian girl, 6 years of age, presented with pruritic rash on both heels of 6 months duration. The lesions appeared as multiple depressions 1–2 mm in diameter that progressively increased in size. There was no history of trauma or insect bite. She reported local pain when walking, worse with moisture and wearing sneakers. On examination, multiple small crater- like depressions were present, some Figure 1. Heel of patient coalescing into a larger lesion on both heels (Figure 1). There was an unpleasant ‘cheesy’ protective/occluded footwear for prolonged odour and a moist appearance. Wood lamp periods.1–4 examination and potassium hydroxide testing for fungal hyphae were negative. Answer 2 Question 1 Pitted keratolysis is frequently seen during What is the diagnosis? summer and rainy seasons, particularly in tropical regions, although it occurs Question 2 worldwide.1,3,4 It is caused by Kytococcus What causes this condition? sedentarius, Dermatophilus congolensis, or species of Corynebacterium, Actinomyces or Question 3 Streptomyces.1–4 Under favourable conditions How would you confirm the diagnosis? (ie. hyperhidrosis, prolonged occlusion and increased skin surface pH), these bacteria Question 4 proliferate and produce proteinases that destroy What are the differential diagnoses? the stratum corneum, creating pits. Sulphur containing compounds produced by the bacteria Question 5 cause the characteristic malodor. What is your management strategy? Answer 3 Answer 1 Pitted keratolysis is usually a clinical Based on the typical clinical picture and the negative diagnosis with typical hyperhidrosis, malodor ancillary tests, the diagnosis of pitted keratolysis (PK) (bromhidrosis) and occasionally, tenderness, is likely. -

What Certified Athletic Trainers and Therapists Need to Know Thomas M
PHYSICIAN PERSPECTIVE Tracy Ray, MD, Column Editor Sports Dermatology: What Certified Athletic Trainers and Therapists Need to Know Thomas M. Dougherty, MD • American Sports Medicine Institute, Birmingham AL OST SPECIAL SKIN problems of athletes are ting shoes for all athletes and gloves for weight lifters M easily observable and can be recognized and racket-sport players can help. and treated early. Proper care can prevent Occlusive folliculitis, also known as acne mechanica disruption of the training or competition schedule. or “football acne,” is a flare of sometimes preexisting Various athletic settings expose the skin to a multi- acne caused by heat, occlusion, and pressure distrib- tude of infectious organisms while increasing its vul- uted in areas under bulky playing equipment (e.g., nerability to infection. A working knowledge of skin shoulders, forehead, chin in football players; legs, arms, disorders in athletes is essential for athletic trainers, trunk in wrestlers). Inflammatory papules and pustules who are often the first to evaluate athletes for medi- are present. A clean absorbent T-shirt should be worn cal problems. under equipment, and the affected areas should be cleansed after a workout. Direct Cutaneous Injury Follicular keloidalis is seen mostly in African-Ameri- can athletes and is a progression of occlusive folliculi- Calluses are the skin’s compensatory, protective re- tis with nontender, firm, fibrous papules around the sponse to friction, most commonly seen on the feet edges of the football helmet, especially at the posterior but also on the hands of golfers and in oar and racket neck and occipital scalp. Surgical treatment, if indicated, sports. -

Palmoplantar Keratoderma with Progressive Gingivitis and Recurrent Pyodermas
Palmoplantar Keratoderma With Progressive Gingivitis and Recurrent Pyodermas Tyler A. Moss, DO; Anne P. Spillane, MD; Sam F. Almquist, MD; Patrick E. McCleskey, MD; Oliver J. Wisco, DO Practice Points Papillon-Lefèvre syndrome (PLS) is an autosomal-recessive inherited transgredient palmoplantar kerato- derma (PPK) that is associated with gingivitis and recurrent pyodermas. The symptoms associated with PLS are thought to be due to cathepsin C gene, CTSC, mutations. CTSC is expressed in epithelial regions commonly affected by PLS and also plays a role in the activation of immune and inflammatory responses. Papillon-Lefèvre syndrome must be differentiated from other conditions causing PPK, such as Haim-Munk syndrome, Greither syndrome, mal de Meleda, Clouston syndrome, Vohwinkel syndrome, and Olmsted syndrome. Treatment of PLS includesCUTIS keratolytics such as urea and/or salicylic acid comb ined with oral retinoids. Active gingivitis may be treated with combined use of amoxicillin and metronidazole. Papillon-Lefèvre syndrome (PLS) is a rare inher- Case Report ited palmoplantar keratoderma (PPK) that is asso- A 30-year-old woman presented to the dermatology ciated with progressive gingivitis and recurrent clinic with erythematous hyperkeratotic plaques on pyodermas.Do We present a caseNot exhibiting classic the palmsCopy and soles. The plaques extended onto features of this autosomal-recessive condition the dorsal aspects of the fingers, toes, hands, and and review the current understanding of its patho- feet (Figures 1 and 2). The patient had psoriasiform physiology, diagnosis, and treatment. Addition- plaques on the extensor surfaces of the knees and ally, a review of pertinent transgredient PPKs is elbows (Figure 3) along with a history of slow- undertaken, with key and distinguishing features progressing gingivitis and periodontal disease that of each syndrome highlighted. -

WO 2014/134709 Al 12 September 2014 (12.09.2014) P O P C T
(12) INTERNATIONAL APPLICATION PUBLISHED UNDER THE PATENT COOPERATION TREATY (PCT) (19) World Intellectual Property Organization International Bureau (10) International Publication Number (43) International Publication Date WO 2014/134709 Al 12 September 2014 (12.09.2014) P O P C T (51) International Patent Classification: (81) Designated States (unless otherwise indicated, for every A61K 31/05 (2006.01) A61P 31/02 (2006.01) kind of national protection available): AE, AG, AL, AM, AO, AT, AU, AZ, BA, BB, BG, BH, BN, BR, BW, BY, (21) International Application Number: BZ, CA, CH, CL, CN, CO, CR, CU, CZ, DE, DK, DM, PCT/CA20 14/000 174 DO, DZ, EC, EE, EG, ES, FI, GB, GD, GE, GH, GM, GT, (22) International Filing Date: HN, HR, HU, ID, IL, IN, IR, IS, JP, KE, KG, KN, KP, KR, 4 March 2014 (04.03.2014) KZ, LA, LC, LK, LR, LS, LT, LU, LY, MA, MD, ME, MG, MK, MN, MW, MX, MY, MZ, NA, NG, NI, NO, NZ, (25) Filing Language: English OM, PA, PE, PG, PH, PL, PT, QA, RO, RS, RU, RW, SA, (26) Publication Language: English SC, SD, SE, SG, SK, SL, SM, ST, SV, SY, TH, TJ, TM, TN, TR, TT, TZ, UA, UG, US, UZ, VC, VN, ZA, ZM, (30) Priority Data: ZW. 13/790,91 1 8 March 2013 (08.03.2013) US (84) Designated States (unless otherwise indicated, for every (71) Applicant: LABORATOIRE M2 [CA/CA]; 4005-A, rue kind of regional protection available): ARIPO (BW, GH, de la Garlock, Sherbrooke, Quebec J1L 1W9 (CA). GM, KE, LR, LS, MW, MZ, NA, RW, SD, SL, SZ, TZ, UG, ZM, ZW), Eurasian (AM, AZ, BY, KG, KZ, RU, TJ, (72) Inventors: LEMIRE, Gaetan; 6505, rue de la fougere, TM), European (AL, AT, BE, BG, CH, CY, CZ, DE, DK, Sherbrooke, Quebec JIN 3W3 (CA). -

An Update of Pitted Keratolysis: a Review
Journal of Current and Advance Medical Research January 2017, Vol. 4, No. 1, pp. 27-30 http://www.banglajol.info/index.php/JCAMR ISSN (Print) 2313-447X Review Article An Update of Pitted Keratolysis: A Review Tania Hoque; Bhuiya Mohammad Mahatab Uddin 1Assistant Professor, Department of Dermatolgy and Venereology, Gonoshasthaya Somaj Vittic Medical college and Hospital, Savar, Dhaka, Bangladesh; 2Assistant Professor, Department of Microbiology, Enam Medical College, Savar, Dhaka, Bangladesh [Reviewed: 30 September 2016; Accepted on: 1 October 2016; Published on: 1 January 2017] Abstract Pitted keratolysis is a bacterial infection of the soles of the feet or less commonly, the palms of the hands. Pitted keratolysis is easily identified by its shallow, crater-like pits. Collection of specimen using swab may be helpful to identify causative bacteria and skin scraping is often taken to exclude fungal infection. The diagnosis is sometimes made by skin biopsy revealing characteristic histopathological feature of Pitted Keratolysis. Treatment generally consists of hygienic measures, sometimes supplemented by medication and perhaps on oral medication. This review is aimed to consolidate present information about aetiopathogenesis, diagnosis and management of Pitted Keratolysis. It is worth mentioning that Pitted Keratolysis is non-contagious. [Journal of Current and Advance Medical Research 2017;4(1):27-30] Keywords: Pitted keratolysis; bacterial infection; non-contagious Correspondence: Dr. Tania Hoque, Assistant Professor, Dept of Dermatolgy and Venereology, Gonoshasthaya Somaj Vittic Medical college and Hospital, Savar, Dhaka, Bangladesh Cite this article as: Hoque T, Uddin BMM. An Update of Pitted Keratolysis: A Review. Journal of Current and Advance Medical Research 2017;4(1):27-30 Conflict of Interest: All the authors have declared that there was no conflict of interest. -

Erythrokeratodermia Variabilis Et Progressiva Allelic to Oculo-Dento
View metadata, citation and similar papers at core.ac.uk brought to you by CORE provided by Elsevier - Publisher Connector COMMENTARY See related article on pg 1540 translocated into the plasma membrane. Once expressed on the cell surface, the hemichannel docks with a connexon of an adjacent cell to form a channel that Erythrokeratodermia Variabilis et is termed gap junction. Connexons can form either homotypic (docking of two Progressiva Allelic to Oculo-Dento- identical connexons), heterotypic (docking of two dissimilar homomeric Digital Dysplasia connexons), or heteromeric (docking of two heteromeric connexons) channels Sabine Duchatelet1,2 and Alain Hovnanian1,2,3 (Mese et al., 2007). These diverse Erythrokeratodermia variabilis et progressiva (EKVP) is a genodermatosis with combinations of connexins create clinical and genetic heterogeneity, most often transmitted in an autosomal different types of channels, each having dominant manner, caused by mutations in GJB3 and GJB4 genes encoding unique properties (ionic conductance, connexins (Cx)31 and 30.3, respectively. In this issue, Boyden et al. (2015) report permeability, sensitivity to voltage, or for the first time de novo dominant mutations in GJA1 encoding the ubiquitous pH). Of note, several connexins may also Cx43 in patients with EKVP. These results expand the genetic heterogeneity of form functional nonjunctional hemi- EKVP and the human disease phenotypes associated with GJA1 mutations. They channels, although their physiological disclose that EKVP is allelic to oculo-dento-digital dysplasia, a rare syndrome relevance remains uncertain (Pfenniger previously known to be caused by dominant GJA1 mutations. et al., 2010). Mutations in 11 connexin genes cause a variety of genetic dis- Journal of Investigative Dermatology (2015) 135, 1475–1478. -

Palmoplantar Keratoderma: Rare Case Report
Case Report Journal of Volume 12:4, 2021 Cytology & Histology ISSN: 2157-7099 Open Access Palmoplantar Keratoderma: Rare Case Report Dr. Ayushi Bansal1, Dr. Hemlata Munde2*, Dr. Munish Gupta3 and Dr. Santosh Munde4 1Senior Resident, Department of Pathology, Kalpana Chawla Government Medical College, Karnal, Haryana, India. 2Professor and Head of Department of Pathology, Kalpana Chawla Government Medical College, Karnal, Haryana, India. 3Assistant Professor, Department of medicine, Kalpana Chawla Government Medical College, Karnal, Haryana, India. 4Professor and Head of Department of Orthopaedics, Kalpana Chawla Government Medical College, Karnal, Haryana, India. Abstract Palmoplantar keratodermas(PPK) are group of cornification disorders characterized by epidermal hyperkeratotic lesions involving the palms and soles. A 50years old healthy male, presented with history of multiple punctate hyperkeratotic papules since last 5 years. Keywords: Palmoplantar keratoderma • Punctate •Hyperkeratotic papules Abbreviations: PPK: Palmoplantar keratodermas • PUVA: Psoralen plus Ultraviolet A • PPPK: Punctate Palmoplantar keratodermas • USG: Ultrasound Sonography• VRDL: Venereal Disease Research Laboratory Test • ELISA: Enzyme-Linked Immunosorbent Assay Introduction Mucosal surfaces were not involved. Biopsy sample was received. On histopathological examination of biopsy revealed massive hyperkeratosis over sharply limited area with depression of malphigian layer below general Palmoplantar keratoderma (PPK), clinically and genetically comprises level of epidermis. There was increase in the thickness of granular layer. The of heterogenous group of disorders characterised by hyperkeratosis of dermis was free of inflammation. Compilation of clinical and laboratory data palms and soles [1]. It can be hereditary or acquired. Hereditary PPK can helped to conclude the diagnosis of Palmoplantar Keratoderma-Punctate be further divided into three major categories: diffuse, focal, and punctate type. -

Dermatologic Features of Smith–Magenis Syndrome
Pediatric Dermatology Vol. 32 No. 3 337–341, 2015 Dermatologic Features of Smith–Magenis Syndrome Morgane Guerin-Moreau, M.D.,*,** Estelle Colin, M.D.,†,** Sylvie Nguyen, M.D., Ph.D.,‡,** Joris Andrieux, M.D., Ph.D.,§ Helene de Leersnyder, M.D.,¶ Dominique Bonneau, M.D., Ph.D.,†,** and Ludovic Martin, M.D., Ph.D.*,** Departments of *Dermatology, †Biochemistry and Genetics, and ‡Pediatrics, University Hospital of Angers, Angers, France, §Department of Genetics, University Hospital of Lille, Lille, France, ¶Department of Pediatrics, Hopital^ Robert Debre, University of Paris VII, Paris, France, **L’UNAM University, Nantes, France Abstract: Smith–Magenis syndrome (SMS) is characterized by dis- tinctive facial and skeletal features, developmental delay, cognitive impairment, and behavioral abnormalities, including self-injurious behav- iors. We aimed to investigate whether cutaneous features are common in SMS. We performed a complete skin examination in 20 young SMS patients. Skin features secondary to self-injurious behavior, such as bites, abrasions, dystrophic scars, limited spots of hyperkeratosis, anomalies of the nails, and whitlows, were found in the majority of patients. Acral pachydermia and fissured plantar keratoderma were common. Xerosis was constant and associated with extensive keratosis pilaris in the majority of patients. Dermatofibromas were frequent in older patients. The hair was dense and shiny, with an unusual hairline. Eyelash trichomegaly and heavy brows were common, as well as folliculitis on the back. The skin features of SMS have rarely been reported in the literature. Some of these are the consequence of neurobehavioral features, but some cutaneous features and abnormalities of appendages have not been reported in other related syndromes. -
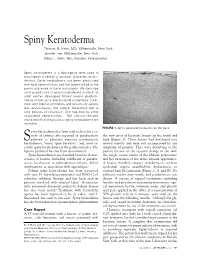
Spiny Keratoderma Thomas N
Spiny Keratoderma Thomas N. Helm, MD, Williamsville, New York Jennifer Lee, Williamsville, New York Klaus F. Helm, MD, Hershey, Pennsylvania Spiny keratoderma is a descriptive term used to encompass a variety of unusual, disparate kerato- dermas. Spiny keratoderma has been associated with lipid abnormalities and has been limited to the palms and soles in some individuals. We describe an acquired case of spiny keratoderma in which an adult woman developed filiform lesions predomi- nating on the trunk and proximal extremities. Treat- ment with topical emollients and keratolytic agents was unsuccessful, but topical tazarotene led to long periods of resolution. She has had no other associated abnormalities. The clinical features and differential diagnosis of spiny keratoderma are reviewed. FIGURE 1. Spiny keratoderma lesions on the back. piny keratoderma has been used to describe a va- riety of entities also reported as porokeratosis the new onset of keratotic lesions on the trunk and S palmaris et plantaris, punctate porokeratotic back (Figure 1). These lesions had developed over keratoderma, “music spine keratosis,” and, most re- several months and were not accompanied by any cently, spiny keratoderma of the palms and soles. Ma- symptoms of pruritus. They were disturbing to the lignant potential has not been documented. patient because of the textural change in the skin; Spiny keratodermas are classified based on charac- the rough, coarse nature of the filiform projections; teristics of lesions, including exhibition of paraker- and her awareness of her skin’s unusual appearance. atosis, localization to palmoplantar surfaces, diffuse A biopsy revealed compact orthokeratosis without involvement, or association with appendages.1 epidermal atypia, acantholytic dyskeratosis, or Palmar spiny keratoderma has been associated cornoid lamella formation (Figure 2, A and B). -

Superficial Fungal Infection
Infeksi jamur superfisial (mikosis superfisialis) R. Wahyuningsih Dep. Parasitologi FK UKI 31 Maret 2020 Klasifikasi mikosis superfisialis berdasarkan penyebab • Dermatofitosis • kandidiasis superfisialis • Infeksi Malassezia/panu M. Raquel Vieira, ESCMID Dermatofitosis • Infeksi jaringan keratin (kulit, kuku & rambut) oleh jamur filamen gol. dermatofita • genus dermatofita – Tricophyton, – Microsporum – Epidermophyton, • ± 10 spesies menyebabkan dermatofitosis pada manusia Asian incidence of the most common mycoses identified All values are percentages In Asia, T. rubrum and T. mentagrophytes are the most commonly isolated pathogens, causing tinea pedis and unguium, as is the case in Europe. Havlickova et al, Mycoses Dermatophytosis di Indonesia • Geofilik: M . gypseum • Zoofilik: M. canis • Antropofilik: – T. rubrum – T. concentricum – E. floccosum Patologi & organ terinfeksi Kuku kulit rambut Trichophyton + + + Microsporum + + + Epidermophyton + + - http://www.njmoldinspection.com/mycoses/moldinfections.html Dermatophytoses...... • Gejala klinik tergantung pada: • Lokalisasi infeksi • Respons imun pejamu • Spesies jamur • Lesi: karakteristik (ring worm) tetapi dalam kondisi imuno supresi menjadi tidak khas perlu pemeriksaan laboratorium Dermatofita & dermatofitosis T. rubrum: biakan. kapang, pigmen merah, mikrokonidia lonjong, tetesan air mata/anggur, makrokonidia seperti pinsil/cerutu . antropofilik, . kelainan kronik mis. • tinea kruris, onikomiksosis De Berker, N Engl J Med 2009;360:2108-16 Dermatofita & dermatofitosis M. canis -

Hereditary Hearing Impairment with Cutaneous Abnormalities
G C A T T A C G G C A T genes Review Hereditary Hearing Impairment with Cutaneous Abnormalities Tung-Lin Lee 1 , Pei-Hsuan Lin 2,3, Pei-Lung Chen 3,4,5,6 , Jin-Bon Hong 4,7,* and Chen-Chi Wu 2,3,5,8,* 1 Department of Medical Education, National Taiwan University Hospital, Taipei City 100, Taiwan; [email protected] 2 Department of Otolaryngology, National Taiwan University Hospital, Taipei 11556, Taiwan; [email protected] 3 Graduate Institute of Clinical Medicine, National Taiwan University College of Medicine, Taipei City 100, Taiwan; [email protected] 4 Graduate Institute of Medical Genomics and Proteomics, National Taiwan University College of Medicine, Taipei City 100, Taiwan 5 Department of Medical Genetics, National Taiwan University Hospital, Taipei 10041, Taiwan 6 Department of Internal Medicine, National Taiwan University Hospital, Taipei 10041, Taiwan 7 Department of Dermatology, National Taiwan University Hospital, Taipei City 100, Taiwan 8 Department of Medical Research, National Taiwan University Biomedical Park Hospital, Hsinchu City 300, Taiwan * Correspondence: [email protected] (J.-B.H.); [email protected] (C.-C.W.) Abstract: Syndromic hereditary hearing impairment (HHI) is a clinically and etiologically diverse condition that has a profound influence on affected individuals and their families. As cutaneous findings are more apparent than hearing-related symptoms to clinicians and, more importantly, to caregivers of affected infants and young individuals, establishing a correlation map of skin manifestations and their underlying genetic causes is key to early identification and diagnosis of syndromic HHI. In this article, we performed a comprehensive PubMed database search on syndromic HHI with cutaneous abnormalities, and reviewed a total of 260 relevant publications.