Vestibular Dysfunction Associated with Hearing Impairment
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Electromagnetic Field and TGF-Β Enhance the Compensatory
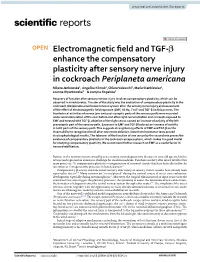
www.nature.com/scientificreports OPEN Electromagnetic feld and TGF‑β enhance the compensatory plasticity after sensory nerve injury in cockroach Periplaneta americana Milena Jankowska1, Angelika Klimek1, Chiara Valsecchi2, Maria Stankiewicz1, Joanna Wyszkowska1* & Justyna Rogalska1 Recovery of function after sensory nerves injury involves compensatory plasticity, which can be observed in invertebrates. The aim of the study was the evaluation of compensatory plasticity in the cockroach (Periplaneta americana) nervous system after the sensory nerve injury and assessment of the efect of electromagnetic feld exposure (EMF, 50 Hz, 7 mT) and TGF‑β on this process. The bioelectrical activities of nerves (pre‑and post‑synaptic parts of the sensory path) were recorded under wind stimulation of the cerci before and after right cercus ablation and in insects exposed to EMF and treated with TGF‑β. Ablation of the right cercus caused an increase of activity of the left presynaptic part of the sensory path. Exposure to EMF and TGF‑β induced an increase of activity in both parts of the sensory path. This suggests strengthening efects of EMF and TGF‑β on the insect ability to recognize stimuli after one cercus ablation. Data from locomotor tests proved electrophysiological results. The takeover of the function of one cercus by the second one proves the existence of compensatory plasticity in the cockroach escape system, which makes it a good model for studying compensatory plasticity. We recommend further research on EMF as a useful factor in neurorehabilitation. Injuries in the nervous system caused by acute trauma, neurodegenerative diseases or even old age are hard to reverse and represent an enormous challenge for modern medicine. -

Hearing Screening Training Manual REVISED 12/2018
Hearing Screening Training Manual REVISED 12/2018 Minnesota Department of Health (MDH) Community and Family Health Division Maternal and Child Health Section 1 2 For more information, contact Minnesota Department of Health Maternal Child Health Section 85 E 7th Place St. Paul, MN 55164-0882 651-201-3760 [email protected] www.health.state.mn.us Upon request, this material will be made available in an alternative format such as large print, Braille or audio recording. 3 Revisions made to this manual are based on: Guidelines for Hearing Screening After the Newborn Period to Kindergarten Age http://www.improveehdi.org/mn/library/files/afternewbornperiodguidelines.pdf American Academy of Audiology, Childhood Screening Guidelines http://www.cdc.gov/ncbddd/hearingloss/documents/AAA_Childhood%20Hearing%2 0Guidelines_2011.pdf American Academy of Pediatrics (AAP), Hearing Assessment in Children: Recommendations Beyond Neonatal Screening http://pediatrics.aappublications.org/content/124/4/1252 4 Contents Introduction .................................................................................................................... 7 Audience ..................................................................................................................... 7 Purpose ....................................................................................................................... 7 Overview of hearing and hearing loss ............................................................................ 9 Sound, hearing, and hearing -
Auditory System & Hearing
Auditory System & Hearing Chapters 9 part II Lecture 17 Jonathan Pillow Sensation & Perception (PSY 345 / NEU 325) Fall 2017 1 Cochlea: physical device tuned to frequency! • place code: tuning of different parts of the cochlea to different frequencies 2 The auditory nerve (AN): fibers stimulated by inner hair cells • Frequency selectivity: Clearest when sounds are very faint 3 Threshold tuning curves for 6 neurons (threshold = lowest intensity that will give rise to a response) Characteristic frequency - frequency to which the neuron is most sensitive threshold(dB) frequency (kHz) 4 Information flow in the auditory pathway • Cochlear nucleus: first brain stem nucleus at which afferent auditory nerve fibers synapse • Superior olive: brainstem region thalamus MGN in the auditory pathway where inputs from both ears converge • Inferior colliculus: midbrain nucleus in the auditory pathway • Medial geniculate nucleus (MGN): part of the thalamus that relays auditory signals to the cortex 5 • Primary auditory cortex (A1): First cortical area for processing audition (in temporal lobe) • Belt & Parabelt areas: areas beyond A1, where neurons respond to more complex characteristics of sounds 6 Basic Structure of the Mammalian Auditory System Comparing overall structure of auditory and visual systems: • Auditory system: Large proportion of processing before A1 • Visual system: Large proportion of processing after V1 7 Basic Structure of the Mammalian Auditory System Tonotopic organization: neurons organized spatially in order of preferred frequency • -

Sensory Change Following Motor Learning
A. M. Green, C. E. Chapman, J. F. Kalaska and F. Lepore (Eds.) Progress in Brain Research, Vol. 191 ISSN: 0079-6123 Copyright Ó 2011 Elsevier B.V. All rights reserved. CHAPTER 2 Sensory change following motor learning { k { { Andrew A. G. Mattar , Sazzad M. Nasir , Mohammad Darainy , and { } David J. Ostry , ,* { Department of Psychology, McGill University, Montréal, Québec, Canada { Shahed University, Tehran, Iran } Haskins Laboratories, New Haven, Connecticut, USA k The Roxelyn and Richard Pepper Department of Communication Sciences and Disorders, Northwestern University, Evanston, Illinois, USA Abstract: Here we describe two studies linking perceptual change with motor learning. In the first, we document persistent changes in somatosensory perception that occur following force field learning. Subjects learned to control a robotic device that applied forces to the hand during arm movements. This led to a change in the sensed position of the limb that lasted at least 24 h. Control experiments revealed that the sensory change depended on motor learning. In the second study, we describe changes in the perception of speech sounds that occur following speech motor learning. Subjects adapted control of speech movements to compensate for loads applied to the jaw by a robot. Perception of speech sounds was measured before and after motor learning. Adapted subjects showed a consistent shift in perception. In contrast, no consistent shift was seen in control subjects and subjects that did not adapt to the load. These studies suggest that motor learning changes both sensory and motor function. Keywords: motor learning; sensory plasticity; arm movements; proprioception; speech motor control; auditory perception. Introduction the human motor system and, likewise, to skill acquisition in the adult nervous system. -

Hearing Loss, Vertigo and Tinnitus
HEARING LOSS, VERTIGO AND TINNITUS Jonathan Lara, DO April 29, 2012 Hearing Loss Facts S Men are more likely to experience hearing loss than women. S Approximately 17 percent (36 million) of American adults report some degree of hearing loss. S About 2 to 3 out of every 1,000 children in the United States are born deaf or hard-of-hearing. S Nine out of every 10 children who are born deaf are born to parents who can hear. Hearing Loss Facts S The NIDCD estimates that approximately 15 percent (26 million) of Americans between the ages of 20 and 69 have high frequency hearing loss due to exposure to loud sounds or noise at work or in leisure activities. S Only 1 out of 5 people who could benefit from a hearing aid actually wears one. S Three out of 4 children experience ear infection (otitis media) by the time they are 3 years old. Hearing Loss Facts S There is a strong relationship between age and reported hearing loss: 18 percent of American adults 45-64 years old, 30 percent of adults 65-74 years old, and 47 percent of adults 75 years old or older have a hearing impairment. S Roughly 25 million Americans have experienced tinnitus. S Approximately 4,000 new cases of sudden deafness occur each year in the United States. Hearing Loss Facts S Approximately 615,000 individuals have been diagnosed with Ménière's disease in the United States. Another 45,500 are newly diagnosed each year. S One out of every 100,000 individuals per year develops an acoustic neurinoma (vestibular schwannoma). -

Hearing Loss
Randal W. Swenson, M.D. Joshua G. Yorgason, M.D. David K. Palmer, M.D. Wesley R. Brown, M.D. John E. Butler, M.D. Nancy J. Stevenson, PA-C Justin D. Gull, M.D. ENT SPECIALISTS Kristin G. Hoopes, PA-C www.entslc.com Hearing Loss Approximately one in ten persons in the United may result from blockage of the ear canal (wax), States has some degree of hearing loss. Hearing is from a perforation (hole) in the ear drum, or from measured in decibels (dB), and a hearing level of 0- infection or disease of any of the three middle ear 25 dB is considered normal hearing. Your level is: bones. With a conductive loss only, the patient will never go deaf, but will always be able to hear, either Right ear _______ dB Left ear _______dB with reconstructive ear surgery or by use of a properly fitted hearing aid. Some patients who are Hearing Severity / % Loss not candidates for surgery, may benefit from a new 25 dB (normal).….0% 65dB(Severe)……...60% technology, the Baha (bone-anchored hearing aid). 35 dB (mild)……..15% 75dB(Severe)……...75% When there is a problem with the inner ear or 45 dB (moderate)..30% >85dB (Profound)..>90% nerve of hearing, a sensori-neural hearing loss occurs. This is most commonly from normal aging, Normal speech discrimination is 88-100%. Yours is: is usually worse in high frequencies, and can progress to total deafness. Noise exposure is another Right ear _______ % Left ear_______% common cause of high frequency hearing loss. Patients with sensori-neural hearing loss usually complain of difficulty hearing in loud environments. -

Audiometric Test Procedures
Audiometric Test Procedures 101 This information is meant to help you better understand the various test procedures as well as some of the terms you might see on an audiometric report. By Larry Medwetsky individual could, in fact, exhibit nor- In the previous issue of Hearing mal hearing acuity across these three Loss Magazine, I provided an over- Anyone who has ever had their frequencies, yet, exhibit a significant view concerning hearing threshold hearing tested should know how hearing loss in the higher frequencies results as recorded on the audiogram to read the audiogram, but that’s (3000-8000 Hz). Thus, it is important and an explanation of the pure-tone easier said than done. Hopefully, to examine the SRT in the context of audiogram. In this article, I will after reading this article you will the other audiometric test findings. describe various test procedures have a greater understanding of the Speech Awareness Threshold that are typically administered in principles discussed and use your (SAT): an audiometric evaluation and what knowledge going forward—be it in Compound words are pre- information the tests provide. reviewing hearing test results you sented, the goal being to determine already have or when discussing your the softest level one can detect the Audiometric Test Procedures results at your next hearing test. presence of words. This test is often Pure-tone Audiometry: Tones of used when an individual’s hearing loss different frequencies are presented; the is so great that the person is unable goal is to find the softest sound level relatively flat hearing losses, and the to recognize/repeat the words, yet is which one can hear (threshold) the average of 500 and 1000 Hz for those aware that words have been presented. -

Audiology and Hearing Aid Services
For more information, call the Hearing Aid Services office nearest you: Comprehensive hearing aid related services Barbourville Bowling Green are available to children diagnosed with (800) 348-4279 (800) 843-5877 permanent childhood hearing loss (PCHL). (606) 546-5109 (270) 746-7816 Elizabethtown Hazard Who should be referred to the OCSHCN (800) 995-6982 (800) 378-3357 Hearing Aid Services program? (270) 766-5370 (606) 435-6167 Children who are in need of new or Lexington Louisville replacement hearing aids and want to (800) 817-3874 (800) 232-1160 receive hearing aids and related services (859) 252-3170 (502) 429-4430 through a OCSHCN audiologist and wish to Morehead Owensboro receive Otology care outside of the (800) 928-3049 (877) 687-7038 clinical Otology program. (606) 783-8610 (270) 687-7038 What audiology services are available Paducah Prestonsburg (800) 443-3651 (800) 594-7058 through the OCSHCN Hearing Aid Services (270) 443-3651 (606) 889-1761 program? Licensed, certified audiologists conduct Somerset (800) 525-4279 periodic comprehensive hearing evaluations, (606) 677-4120 hearing aid checks, hearing aid repairs and Audiology and hearing aid evaluations according to ASHA best practices guidelines. Comprehensive Kentucky Cabinet for Health and Family Services Hearing Aid Services Office for Children with Special Health Care Needs reports are provided to the managing 310 Whittington Parkway, Suite 200, Louisville, KY 40222 otolaryngologist on an on-going basis; Phone: (502) 429-4430 or (800) 232-1160 FAX: (502) 429-4489 additional follow up testing will be http://chfs.ky.gov/agencies/ccshcn Information for Parents and Equal Opportunity Employer M/D/F completed at physician request. -

Anatomy of the Ear ANATOMY & Glossary of Terms
Anatomy of the Ear ANATOMY & Glossary of Terms By Vestibular Disorders Association HEARING & ANATOMY BALANCE The human inner ear contains two divisions: the hearing (auditory) The human ear contains component—the cochlea, and a balance (vestibular) component—the two components: auditory peripheral vestibular system. Peripheral in this context refers to (cochlea) & balance a system that is outside of the central nervous system (brain and (vestibular). brainstem). The peripheral vestibular system sends information to the brain and brainstem. The vestibular system in each ear consists of a complex series of passageways and chambers within the bony skull. Within these ARTICLE passageways are tubes (semicircular canals), and sacs (a utricle and saccule), filled with a fluid called endolymph. Around the outside of the tubes and sacs is a different fluid called perilymph. Both of these fluids are of precise chemical compositions, and they are different. The mechanism that regulates the amount and composition of these fluids is 04 important to the proper functioning of the inner ear. Each of the semicircular canals is located in a different spatial plane. They are located at right angles to each other and to those in the ear on the opposite side of the head. At the base of each canal is a swelling DID THIS ARTICLE (ampulla) and within each ampulla is a sensory receptor (cupula). HELP YOU? MOVEMENT AND BALANCE SUPPORT VEDA @ VESTIBULAR.ORG With head movement in the plane or angle in which a canal is positioned, the endo-lymphatic fluid within that canal, because of inertia, lags behind. When this fluid lags behind, the sensory receptor within the canal is bent. -

Sensory Overamplification in Layer 5 Auditory Corticofugal Projection Neurons Following Cochlear Nerve Synaptic Damage
Corrected: Publisher correction ARTICLE DOI: 10.1038/s41467-018-04852-y OPEN Sensory overamplification in layer 5 auditory corticofugal projection neurons following cochlear nerve synaptic damage Meenakshi M. Asokan1,2, Ross S. Williamson1,3, Kenneth E. Hancock1,3 & Daniel B. Polley1,2,3 Layer 5 (L5) cortical projection neurons innervate far-ranging brain areas to coordinate integrative sensory processing and adaptive behaviors. Here, we characterize a plasticity in 1234567890():,; L5 auditory cortex (ACtx) neurons that innervate the inferior colliculus (IC), thalamus, lateral amygdala and striatum. We track daily changes in sound processing using chronic widefield calcium imaging of L5 axon terminals on the dorsal cap of the IC in awake, adult mice. Sound level growth functions at the level of the auditory nerve and corticocollicular axon terminals are both strongly depressed hours after noise-induced damage of cochlear afferent synapses. Corticocollicular response gain rebounded above baseline levels by the following day and remained elevated for several weeks despite a persistent reduction in auditory nerve input. Sustained potentiation of excitatory ACtx projection neurons that innervate multiple limbic and subcortical auditory centers may underlie hyperexcitability and aberrant functional coupling of distributed brain networks in tinnitus and hyperacusis. 1 Eaton-Peabody Laboratories, Massachusetts Eye and Ear Infirmary, Boston, MA 02114, USA. 2 Division of Medical Sciences, Harvard University, Boston, MA 02114, USA. 3 Department of Otolaryngology, Harvard Medical School, Boston, MA 02114, USA. Correspondence and requests for materials should be addressed to M.M.A. (email: [email protected]) NATURE COMMUNICATIONS | (2018) 9:2468 | DOI: 10.1038/s41467-018-04852-y | www.nature.com/naturecommunications 1 ARTICLE NATURE COMMUNICATIONS | DOI: 10.1038/s41467-018-04852-y he auditory system employs a variety of gain control to the IC and striatum33 or both to the IC and brainstem34). -

Differential Diagnosis and Treatment of Hearing Loss JON E
Differential Diagnosis and Treatment of Hearing Loss JON E. ISAACSON, M.D., and NEIL M. VORA, M.D., Milton S. Hershey Medical Center, Hershey, Pennsylvania Hearing loss is a common problem that can occur at any age and makes verbal communication difficult. The ear is divided anatomically into three sections (external, middle, and inner), and pathology contributing to hearing loss may strike one or more sections. Hearing loss can be cat- egorized as conductive, sensorineural, or both. Leading causes of conductive hearing loss include cerumen impaction, otitis media, and otosclerosis. Leading causes of sensorineural hear- ing loss include inherited disorders, noise exposure, and presbycusis. An understanding of the indications for medical management, surgical treatment, and amplification can help the family physician provide more effective care for these patients. (Am Fam Physician 2003;68:1125-32. Copyright© 2003 American Academy of Family Physicians) ore than 28 million Amer- tive, the sound will be heard best in the icans have some degree of affected ear. If the loss is sensorineural, the hearing impairment. The sound will be heard best in the normal ear. differential diagnosis of The sound remains midline in patients with hearing loss can be sim- normal hearing. Mplified by considering the three major cate- The Rinne test compares air conduction gories of loss. Conductive hearing loss occurs with bone conduction. The tuning fork is when sound conduction is impeded through struck softly and placed on the mastoid bone the external ear, the middle ear, or both. Sen- (bone conduction). When the patient no sorineural hearing loss occurs when there is a longer can hear the sound, the tuning fork is problem within the cochlea or the neural placed adjacent to the ear canal (air conduc- pathway to the auditory cortex. -

Shopping Wisely for Hearing Aids
Consumer’s Edge Consumer Protection Division, Maryland Office of the Attorney General Brian E. Frosh, Maryland Attorney General Listen Up! Shopping Wisely for Hearing Aids Evelyn spent $2,300 for hearing aids but they did not your problem is diagnosed properly, since a hearing loss improve her ability to hear. Although she informed the may be a symptom of a more serious medical condition. seller, he repeatedly insisted she simply needed more time to get used to them. The sales contract didn’t in- A hearing aid seller is required by federal law to inform clude the 30-day notice of cancellation as required by you that it is in your best interest to have a medical exam law. After contacting the Attorney General’s Consumer by a licensed physician. In fact, your hearing must be Protection Division, she was able to get a refund. evaluated by a doctor before you buy a hearing aid, unless you sign a statement saying you’ve waived that protection. Don’t sign it. It’s always wise to have a medical evaluation to make sure all medically treatable conditions that may affect your hearing are identified and treated before you purchase a hearing aid. What kind of doctor should you see to have your hearing evaluated? The U.S. Food and Drug Administration recom- mends an ear, nose and throat specialist (otolaryngologist), an ear specialist (otologist) or any licensed physician. Look for the right seller. Once your doctor confirms you need a hearing aid, you’ll need a hearing aid evaluation. Hearing aids can be difficult to fit, often requiring several adjustments.