PE2370 Device Options for Hearing Loss
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Age-Related Hearing Loss
U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES ∙ National Institutes of Health NIDCD Fact Sheet | Hearing and Balance Age-Related Hearing Loss What is age-related hearing loss? The auditory system Age-related hearing loss (presbycusis) is the loss of hearing that gradually occurs in most of us as we grow older. It is one of the most common conditions affecting older and elderly adults. Approximately one in three people in the United States between the ages of 65 and 74 has hearing loss, and nearly half of those older than 75 have difficulty hearing. Having trouble hearing can make it hard to understand and follow a doctor’s advice, respond to warnings, and hear phones, doorbells, and smoke alarms. Hearing loss can also make it hard to enjoy talking with family and friends, leading to feelings of isolation. Age-related hearing loss most often occurs in both ears, affecting them equally. Because the loss is gradual, if you have age-related hearing loss you Credit: NIH Medical Arts may not realize that you’ve lost some of your ability to hear. How do we hear? There are many causes of age-related hearing Hearing depends on a series of events that change loss. Most commonly, it arises from changes in sound waves in the air into electrical signals. Your the inner ear as we age, but it can also result auditory nerve then carries these signals to your from changes in the middle ear, or from complex brain through a complex series of steps. changes along the nerve pathways from the ear 1. -

Perforated Eardrum
Vinod K. Anand, MD, FACS Nose and Sinus Clinic Perforated Eardrum A perforated eardrum is a hole or rupture m the eardrum, a thin membrane which separated the ear canal and the middle ear. The medical term for eardrum is tympanic membrane. The middle ear is connected to the nose by the eustachian tube. A perforated eardrum is often accompanied by decreased hearing and occasional discharge. Paih is usually not persistent. Causes of Eardrum Perforation The causes of perforated eardrum are usually from trauma or infection. A perforated eardrum can occur: if the ear is struck squarely with an open hand with a skull fracture after a sudden explosion if an object (such as a bobby pin, Q-tip, or stick) is pushed too far into the ear canal. as a result of hot slag (from welding) or acid entering the ear canal Middle ear infections may cause pain, hearing loss and spontaneous rupture (tear) of the eardrum resulting in a perforation. In this circumstance, there may be infected or bloody drainage from the ear. In medical terms, this is called otitis media with perforation. On rare occasions a small hole may remain in the eardrum after a previously placed P.E. tube (pressure equalizing) either falls out or is removed by the physician. Most eardrum perforations heal spontaneously within weeks after rupture, although some may take up to several months. During the healing process the ear must be protected from water and trauma. Those eardrum perforations which do not heal on their own may require surgery. Effects on Hearing from Perforated Eardrum Usually, the larger the perforation, the greater the loss of hearing. -
Learning About Hearing Aids
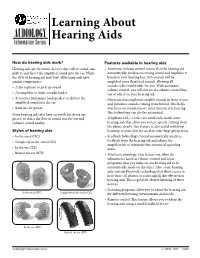
Learning About AUDIOLOGY Information Series Hearing Aids How do hearing aids work? Features available in hearing aids Hearing aids are electronic devices that collect sound, am- • Automatic volume control means that the hearing aid plify it, and direct the amplified sound into the ear. While automatically analyzes incoming sound and amplifies it the style of hearing aid may vary, all hearing aids have based on your hearing loss. Soft sounds will be similar components: amplified more than loud sounds, allowing all • A microphone to pick up sound sounds to be comfortable for you. With automatic volume control, you will not need a volume control but- • An amplifier to make sounds louder ton or wheel on your hearing aid. • A receiver (miniature loudspeaker) to deliver the • Directional microphones amplify sounds in front of you amplified sound into the ear and minimize sounds coming from behind. This helps • Batteries for power you focus on sound you are most interested in hearing. This technology can also be automated. Some hearing aids also have earmolds (or dome ear pieces) to direct the flow of sound into the ear and • Telephone coils (t-coils) are small coils inside some enhance sound quality. hearing aids that allow you to hear speech coming from the phone clearly. This feature is also useful with loop Styles of hearing aids listening systems that are used in some large group areas. • In-the-canal (ITC) • Feedback (whistling) control automatically analyzes • Completely-in-the-canal (CIC) feedback from the hearing aid and adjusts the amplification to minimize this unwanted squealing • In-the-ear (ITE) noise. -

A Study on Wireless Hearing Aids System Configuration and Simulation
View metadata, citation and similar papers at core.ac.uk brought to you by CORE provided by ScholarBank@NUS A STUDY ON WIRELESS HEARING AIDS SYSTEM CONFIGURATION AND SIMULATION TANG BIN NATIONAL UNIVERSITY OF SINGAPORE 2005 A STUDY ON WIRELESS HEARING AIDS SYSTEM CONFIGURATION AND SIMULATION TANG BIN (B. ENG) A THESIS SUBMITTED FOR THE DEGREE OF MASTER OF SCIENCE GRADUATE PROGRAM IN BIOENGINEERING NATIONAL UNIVERSITY OF SINGAPORE 2005 ACKNOWLEDGEMENT I would like to thank my supervisors, Dr. Ram Singh Rana, A/Prof. Hari Krishna Garg, and Dr. Wang De Yun for their invaluable guidance, advice and motivation. Without their generous guidance and patience, it would have been an insurmountable task in completing this work. Their research attitudes and inspirations have impressed me deeply. I have learned from them not only how to do the research work, but also the way to difficulties and life. I would also like to extend my appreciation to A/Prof. Hanry Yu and Prof. Teoh Swee Hin, for the founding and growing of the Graduate Program in bioengineering, and also the perfect research environment they have created for the students. Special thanks to Dr. Hsueh Yee Lim from National University Hospital for her precious suggestions and encouragement as a hearing clinician to my research work. Thanks my colleague Zhang Liang, who is pursuing his master degree in department of Electrical and Computer Engineering. The valuable suggestions and discussions with him have contributed a lot to this work. This work would have been impossible without the consent for Dr. Wang De Yun to support my scholarship. -

Hearing Screening Training Manual REVISED 12/2018
Hearing Screening Training Manual REVISED 12/2018 Minnesota Department of Health (MDH) Community and Family Health Division Maternal and Child Health Section 1 2 For more information, contact Minnesota Department of Health Maternal Child Health Section 85 E 7th Place St. Paul, MN 55164-0882 651-201-3760 [email protected] www.health.state.mn.us Upon request, this material will be made available in an alternative format such as large print, Braille or audio recording. 3 Revisions made to this manual are based on: Guidelines for Hearing Screening After the Newborn Period to Kindergarten Age http://www.improveehdi.org/mn/library/files/afternewbornperiodguidelines.pdf American Academy of Audiology, Childhood Screening Guidelines http://www.cdc.gov/ncbddd/hearingloss/documents/AAA_Childhood%20Hearing%2 0Guidelines_2011.pdf American Academy of Pediatrics (AAP), Hearing Assessment in Children: Recommendations Beyond Neonatal Screening http://pediatrics.aappublications.org/content/124/4/1252 4 Contents Introduction .................................................................................................................... 7 Audience ..................................................................................................................... 7 Purpose ....................................................................................................................... 7 Overview of hearing and hearing loss ............................................................................ 9 Sound, hearing, and hearing -

Facts About Noise-Induced Hearing Loss Over 85 Db
Facts about Noise-Induced Hearing Loss over 85 dB. Sound loudness is measured in Approximately 40 million American adults may have units called decibels (dB). hearing loss resulting from noise exposure.1 Noise- 60 dB Normal conversations, induced hearing loss is caused by damage to the dishwashers hair cells found in the inner ear. Hair cells are small 80 dB Alarm clocks sensory cells that convert the sounds we hear 90 dB Hair dryers, blenders, (sound energy) into electrical signals that travel to lawnmowers the brain. Once damaged, our hair cells cannot 100 dB MP3 players at full volume grow back, which results in permanent hearing loss. 110 dB Concerts (any music genre), car racing, sporting events Hearing protection decreases the intensity, or 120 dB Jet planes at take off loudness, of noise and helps preserve your hearing. 130 dB Ambulance, fire engine sirens 140 dB Gun shots, fireworks, custom car Harmful sounds are those that are too loud and last stereos at full volume too long or are very loud and sudden. For example, exposure to a one-time intense “impulse” sound Protect your hearing: such as an explosion, or continuous exposure to • Wear hearing protection when around loud sounds over an extended period of time such sounds louder than 85 dB. There are as at a concert may be harmful. The louder the different types of hearing protection such as sound, the shorter the amount of time you can foam earplugs, earmuffs, and custom safely be around it. hearing protection devices • Contact your local audiologist for custom You may encounter harmful sounds at work, at hearing protection devices. -

SENSORY MOTOR COORDINATION in ROBONAUT Richard Alan Peters
SENSORY MOTOR COORDINATION IN ROBONAUT 5 Richard Alan Peters 11 Vanderbilt University School of Engineering JSC Mail Code: ER4 30 October 2000 Robert 0. Ambrose Robotic Systems Technology Branch Automation, Robotics, & Simulation Division Engineering Directorate Richard Alan Peters II Robert 0. Ambrose SENSORY MOTOR COORDINATION IN ROBONAUT Final Report NASNASEE Summer Faculty Fellowship Program - 2000 Johnson Space Center Prepared By: Richard Alan Peters II, Ph.D. Academic Rank: Associate Professor University and Department: Vanderbilt University Department of Electrical Engineering and Computer Science Nashville, TN 37235 NASNJSC Directorate: Engineering Division: Automation, Robotics, & Simulation Branch: Robotic Systems Technology JSC Colleague: Robert 0. Ambrose Date Submitted: 30 October 2000 Contract Number: NAG 9-867 13-1 ABSTRACT As a participant of the year 2000 NASA Summer Faculty Fellowship Program, I worked with the engineers of the Dexterous Robotics Laboratory at NASA Johnson Space Center on the Robonaut project. The Robonaut is an articulated torso with two dexterous arms, left and right five-fingered hands, and a head with cameras mounted on an articulated neck. This advanced space robot, now dnven only teleoperatively using VR gloves, sensors and helmets, is to be upgraded to a thinking system that can find, in- teract with and assist humans autonomously, allowing the Crew to work with Robonaut as a (junior) member of their team. Thus, the work performed this summer was toward the goal of enabling Robonaut to operate autonomously as an intelligent assistant to as- tronauts. Our underlying hypothesis is that a robot can deveZop intelligence if it learns a set of basic behaviors ([.e., reflexes - actions tightly coupled to sensing) and through experi- ence learns how to sequence these to solve problems or to accomplish higher-level tasks. -
Remote Microphone + Operations Manual
Remote Microphone + OPERATIONS MANUAL Table of Contents Overview � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 2 Basic Use � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 6 Daily Use � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 8 Wearing the Remote Mic + � � � � � � � � � � � � � � � � � � � � � � 10 Pairing with Hearing Aids � � � � � � � � � � � � � � � � � � � � � � � 11 Pairing with Bluetooth Devices � � � � � � � � � � � � � � � � � � � 13 Using the Input Mode Button � � � � � � � � � � � � � � � � � � � � 14 Remote Microphone � � � � � � � � � � � � � � � � � � � � � � � � � � � 14 Bluetooth Phone and Audio � � � � � � � � � � � � � � � � � � � � � 15 Loop System � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 17 FM System � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 17 Line-In � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 17 Start/Stop Audio Streaming � � � � � � � � � � � � � � � � � � � � � 18 Assembling the Power Adapter � � � � � � � � � � � � � � � � � � � 19 Troubleshooting � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 20 Safety Information � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 23 Regulatory Notices � � � � � � � � � � � � � � � � � � � � � � � � � � � � 26 2 | Overview Overview | 3 The Remote Microphone + is designed to stream 2 audio from different audio sources directly to your 2.4 3 GHz wireless hearing aids. 1 When worn by a distant -

Status and Strategies Analysis on International Standardization of Auricular Acupuncture Points
Online Submissions:http://www.journaltcm.com J Tradit Chin Med 2013 June 15; 33(3): 408-412 [email protected] ISSN 0255-2922 © 2013 JTCM. All rights reserved. REVIEWTOPIC Status and strategies analysis on international standardization of auricular acupuncture points Lei Wang, Baixiao Zhao, Liqun Zhou aa Lei Wang, Baixiao Zhao, School of Acupuncture-Moxibus- Germany. Clinical AAP research was done in Italy, tion and Tuina, Beijing University of Chinese Medicine, Bei- Austria, Switzerland, Spain, the UK, Holland, Japan, jing 100029, China Russia, and Africa. However, AAP research was not Liqun Zhou, Department of Humanities of Traditional Chi- communicated internationally. The World Federa- nese Medicine, School of Basic Medical Sciences, Beijing Uni- tion of Acupuncture-Moxibustion Societies recom- versity of Chinese Medicine, Beijing 100029, China Supported by a Grant of Key Technology Standard Promo- mended international standard of auricular acu- tion Project (No. 2006BAK04A20) from the Ministry of Sci- puncture points (ISAAPs). Standardized nomencla- ence and Technology of China, and a Grant (No. 2009B26) ture and locations of AAPs would provide a solid from the World Federation of Acupuncture and Moxibustion basis to draft an international standard organiza- Societies tion. Correspondence to: Prof. Baixiao Zhao, School of Acu- puncture-Moxibustion and Tuina, Beijing University of Chi- CONCLUSION: Experts need to find common nese Medicine, Beijing 100029, China. baixiao100@gmail. points from different countries or regions, provide com evidence of different ideas, and list the proposal as Telephone: +86-10-64286737; +86-13911040781 a recommendation for an international standard. Accepted: January 27, 2013 © 2013 JTCM. All rights reserved. Abstract Key words: Acupuncture, ear; Reference standards; Information storage and retrieval OBJECTIVE: To supply literature for developing an international standard of auricular acupuncture points. -

Study Guide Medical Terminology by Thea Liza Batan About the Author
Study Guide Medical Terminology By Thea Liza Batan About the Author Thea Liza Batan earned a Master of Science in Nursing Administration in 2007 from Xavier University in Cincinnati, Ohio. She has worked as a staff nurse, nurse instructor, and level department head. She currently works as a simulation coordinator and a free- lance writer specializing in nursing and healthcare. All terms mentioned in this text that are known to be trademarks or service marks have been appropriately capitalized. Use of a term in this text shouldn’t be regarded as affecting the validity of any trademark or service mark. Copyright © 2017 by Penn Foster, Inc. All rights reserved. No part of the material protected by this copyright may be reproduced or utilized in any form or by any means, electronic or mechanical, including photocopying, recording, or by any information storage and retrieval system, without permission in writing from the copyright owner. Requests for permission to make copies of any part of the work should be mailed to Copyright Permissions, Penn Foster, 925 Oak Street, Scranton, Pennsylvania 18515. Printed in the United States of America CONTENTS INSTRUCTIONS 1 READING ASSIGNMENTS 3 LESSON 1: THE FUNDAMENTALS OF MEDICAL TERMINOLOGY 5 LESSON 2: DIAGNOSIS, INTERVENTION, AND HUMAN BODY TERMS 28 LESSON 3: MUSCULOSKELETAL, CIRCULATORY, AND RESPIRATORY SYSTEM TERMS 44 LESSON 4: DIGESTIVE, URINARY, AND REPRODUCTIVE SYSTEM TERMS 69 LESSON 5: INTEGUMENTARY, NERVOUS, AND ENDOCRINE S YSTEM TERMS 96 SELF-CHECK ANSWERS 134 © PENN FOSTER, INC. 2017 MEDICAL TERMINOLOGY PAGE III Contents INSTRUCTIONS INTRODUCTION Welcome to your course on medical terminology. You’re taking this course because you’re most likely interested in pursuing a health and science career, which entails proficiencyincommunicatingwithhealthcareprofessionalssuchasphysicians,nurses, or dentists. -

Vestibular Neuritis, Labyrinthitis, and a Few Comments Regarding Sudden Sensorineural Hearing Loss Marcello Cherchi
Vestibular neuritis, labyrinthitis, and a few comments regarding sudden sensorineural hearing loss Marcello Cherchi §1: What are these diseases, how are they related, and what is their cause? §1.1: What is vestibular neuritis? Vestibular neuritis, also called vestibular neuronitis, was originally described by Margaret Ruth Dix and Charles Skinner Hallpike in 1952 (Dix and Hallpike 1952). It is currently suspected to be an inflammatory-mediated insult (damage) to the balance-related nerve (vestibular nerve) between the ear and the brain that manifests with abrupt-onset, severe dizziness that lasts days to weeks, and occasionally recurs. Although vestibular neuritis is usually regarded as a process affecting the vestibular nerve itself, damage restricted to the vestibule (balance components of the inner ear) would manifest clinically in a similar way, and might be termed “vestibulitis,” although that term is seldom applied (Izraeli, Rachmel et al. 1989). Thus, distinguishing between “vestibular neuritis” (inflammation of the vestibular nerve) and “vestibulitis” (inflammation of the balance-related components of the inner ear) would be difficult. §1.2: What is labyrinthitis? Labyrinthitis is currently suspected to be due to an inflammatory-mediated insult (damage) to both the “hearing component” (the cochlea) and the “balance component” (the semicircular canals and otolith organs) of the inner ear (labyrinth) itself. Labyrinthitis is sometimes also termed “vertigo with sudden hearing loss” (Pogson, Taylor et al. 2016, Kim, Choi et al. 2018) – and we will discuss sudden hearing loss further in a moment. Labyrinthitis usually manifests with severe dizziness (similar to vestibular neuritis) accompanied by ear symptoms on one side (typically hearing loss and tinnitus). -

Inner Ear Infection (Otitis Interna) in Dogs
Hurricane Harvey Client Education Kit Inner Ear Infection (Otitis Interna) in Dogs My dog has just been diagnosed with an inner ear infection. What is this? Inflammation of the inner ear is called otitis interna, and it is most often caused by an infection. The infectious agent is most commonly bacterial, although yeast and fungus can also be implicated in an inner ear infection. If your dog has ear mites in the external ear canal, this can ultimately cause a problem in the inner ear and pose a greater risk for a bacterial infection. Similarly, inner ear infections may develop if disease exists in one ear canal or when a benign polyp is growing from the middle ear. A foreign object, such as grass seed, may also set the stage for bacterial infection in the inner ear. Are some dogs more susceptible to inner ear infection? Dogs with long, heavy ears seem to be predisposed to chronic ear infections that ultimately lead to otitis interna. Spaniel breeds, such as the Cocker spaniel, and hound breeds, such as the bloodhound and basset hound, are the most commonly affected breeds. Regardless of breed, any dog with a chronic ear infection that is difficult to control may develop otitis interna if the eardrum (tympanic membrane) is damaged as it allows bacteria to migrate down into the inner ear. "Dogs with long, heavy ears seem to bepredisposed to chronic ear infections that ultimately lead to otitis interna." Excessively vigorous cleaning of an infected external ear canal can sometimes cause otitis interna. Some ear cleansers are irritating to the middle and inner ear and can cause signs of otitis interna if the eardrum is damaged and allows some of the solution to penetrate too deeply.