A Medley of Fetal Brain Anomalies No Disclosures
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

A Case Report Cem Yener Trakya University, Turkey
American Journal of Preventive Medicine and Public Health Open Access Iniencephaly: A Case Report Cem Yener Trakya University, Turkey ABSTRACT of head, spinal dysmorphism, and lordosis of cervicothoracic vertebrae. Iniencephaly is in the same family of neural tube defects as spina Iniencephaly is a rare neural tube defect characterized by the presence of occipital bone defects at foramen magnum, fixed retroflexion bifida, but it is more severe. The frequency varies between 0.1-10 / 10,000. Most of the fetuses are female. Etiopathogenesis is not known. According to some sources, it has been associated with trisomy 13, 18 and monosomy X. AFP(alfa-feto protein) as a biochemical marker is generally increased. Here we present a 30 years old 19 weeks pregnant women that was referred to our Perinatology Department. We detected polihydramnios, extreme retroflexion of the head, absent neck, low set ears and major cardiac anomaly on ultrasonography. We informed family and with family consent we terminated pregnancy (Image 1). In conclusion, iniencephaly is a neural tube defect with unknown etiopathogenesis. There is no standard treatment for iniencephaly since most infants rarely live longer than a few hours. Medicine is based more on prevention using supplementation with folic acid. Numerous studies have demonstrated that mothers can reduce the risk of neural tube birth defects such as iniencephaly by up to 70 percent with daily supplements of at least 4 mg of folic disordersacid. Pregnant so prenatal women care should is important avoid taking for these antiepileptic patients. drugs, diuretics, antihistamines, and sulfa drugs, which have been shown to be associated with an increased risk of neural tube defects. -

Iniencephaly: Radiological and Pathological Features of a Series of Three Cases Panduranga Chikkannaiah, V
Published online: 2019-09-25 Case Report Iniencephaly: Radiological and pathological features of a series of three cases Panduranga Chikkannaiah, V. Srinivasamurthy, B. S. Satish Prasad1, Pradeepkumar Lalyanayak, Divya N. Shivaram Department of Pathology, 1Radiology, ESIC Medical College and PGIMSR, Rajajinagar, Bangalore, Karnataka, India ABSTRACT Iniencephaly is a rare form of neural tube defect with an incidence of 0.1‑10 in 10,000 pregnancies. It is characterized by the presence of occipital bone defects at foramen magnum, fixed retroflexion of head, spinal dysmorphism, and lordosis of cervicothoracic vertebrae. It is usually associated with central nervous system, gastrointestinal, and cardiovascular anomalies. We present radiological and autopsy findings in a series of 3 cases of iniencephaly (gestational ages 29.3, 23, and 24 weeks) first fetus in addition showed omphalocele, pulmonary hypoplasia, two lobes in right lung, accessory spleen, atrial septal defect, bilateral clubfoot, ambiguous genitalia, and single umbilical artery. Second fetus was a classical case of iniencephaly apertus with spina bifida. Third fetus had colpocephaly and bifid spine. Key words: Colpocephaly, iniencephaly, omphalocele, pulmonary hypoplasia, spina bifida Introduction as her routine anomalous ultrasonogram (USG) done at a primary center revealed defective development of spine, Iniencephaly is a rare, fatal neural tube defect (NTD) atrial septal defect (ASD), aplasia of the right kidney, characterized by occipital bone defects at foramen magnum, and encephalocele. The mother’s routine blood and fixed retroflexion of head, spinal dysmorphism, and biochemical investigations were within normal limits. lordosis of cervicothoracic vertebrae.[1] Howkin and Lawrie She was not a known diabetic or hypertensive and had in 1939 classified iniencephaly into two types based on the a history of nonconsanguineous marriage. -

Ultrasound Anomaly Details
Appendix 2. Association of Copy Number Variants With Specific Ultrasonographically Detected Fetal Anomalies Ultrasound Anomaly Details Abdominal wall Bladder exstrophy Body-stalk anomaly Cloacal exstrophy Gastroschisis Omphalocele Other: free text box CNS Absent cerebellar vermis Agenesis of corpus collosum Anencephaly Arachnoid cyst Cerebellar hypoplasia Chiari malformation Dandy-Walker malformation Encephalocele Anterior Posterior Holoprosencephaly Hydranencephaly Iniencephaly Lissencephaly Parenchymal defect Posterior fossa cyst Spina bifida Vascular anomaly Ventriculomegaly/Hydrocephaly Unilateral Mild (10-12mm) Moderate (13-15mm) Severe (>15mm) Bilateral Mild (10-12mm) Moderate (13-15mm) Severe (>15mm) Other: free text box Ear Outer ear malformation Unilateral Bilateral Other: free text box Effusion Hydrops Single effusion only Ascites Pericardial effusion Pleural effusion Skin edema Donnelly JC, Platt LD, Rebarber A, Zachary J, Grobman WA, and Wapner RJ. Association of copy number variants with specific ultrasonographically detected fetal anomalies. Obstet Gynecol 2014;124. The authors provided this information as a supplement to their article. © Copyright 2014 American College of Obstetricians and Gynecologists. Page 1 of 6 Other: free text box Fac Eye anomalies Cyclopia Hypertelorism Hypotelorism Microphthalmia Other: free text box Facial tumor Lip - Cleft Unilateral Midline Bilateral Nose Absent / hypoplastic nose bone Depressed nasal bridge Palate – Cleft Profile -

INIENCEPHALY: a RARE NEURAL TUBE Defectu
INIENCEPHALY: A RARE NEURAL TUBE DEFECT◆ (İniensefali: Nadir Bir Nöral Tüp Defekti) Banu Dane*, Cem Dane*, Murat Kıray*, Salih Dural*, Ahmet Çetin*, Murat Yayla* Summary Background: Iniencephaly is a rare craniocervical deformity characterized by marked, fixed retroflexion of the head and a short, immobile neck. We report a case of iniencephaly diagnosed prenatally by ultrasound examination. Case presentation: A 20-year-old gravida 1 woman was first seen in our antenatal clinic at 24 weeks' pregnancy. On ultrasound examination a fixed retroflexion of the head, severe microcephaly, anencephaly, meningocele, deformed spine with cervical dysraphism, and omphalocele were found. She delivered a 440 g, 24 weeks- old female fetus. Postmortem examination confirmed the diagnosis of iniencephaly. Discussion: The ultrasonic diagnosis of iniencephaly should be based on the finding of extreme retroflexion of the head accompanied by an abnormally short and deformed spine. Early diagnosis and termination of pregnancy reduces the maternal risks. The mother should be recommended folic acid supplementation for future pregnancies. Key words: Iniencephaly, neural tube defect, prenatal ultrasonography. Özet Giriş: İniensefali, başın fikse ve belirgin retrofleksiyonu, ayrıca kısa ve hareketsiz ense ile karakterize nadir bir kranioservikal deformitedir. Biz bu vaka sunumunda prenatal dönemde ultrasonografi ile tanı koyduğumuz iniensefali vakasını bildirdik. Vaka Sunumu: İlk gebeliğin 24. haftasında gebe polikliniğine başvuran hastanın yapılan ultrasonografi muayenesinde fetal başın fikse enseye yapışık olması, şiddetli mikrosefali, anensefali, meningosel, servikal açıklıkla beraber deforme olmuş omurga ve omfalosel saptandı. Bu bulgularla 440 g ağırlığında kız bebek doğurtuldu. Doğum sonrası yapılan otopside iniensefali tanısı doğrulandı. Tartışma: İniensefalinin ultrasonografik olarak tanısında temel olarak oldukça kısa ve deforme olmuş omurga ile birlikte başın ileri derecede retrofleksiyonu mutlaka bulunmalıdır. -

Iniencephaly and Holoprosencephaly: Report of a Rare Association
Hindawi Publishing Corporation Case Reports in Obstetrics and Gynecology Volume 2014, Article ID 849589, 4 pages http://dx.doi.org/10.1155/2014/849589 Case Report Iniencephaly and Holoprosencephaly: Report of a Rare Association Aytekin Tokmak, Hakan Timur, Korkut DaLlar, and Özgür Kara Department of Obstetrics and Gynecology, Dr. Zekai Tahir Burak Women’s Health Education and Research Hospital, 06240 Ankara, Turkey Correspondence should be addressed to Aytekin Tokmak; [email protected] Received 9 May 2014; Revised 22 June 2014; Accepted 23 June 2014; Published 2 July 2014 Academic Editor: Eliezer Shalev Copyright © 2014 Aytekin Tokmak et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. The aim of this study is to discuss a rare association of iniencephaly and holoprosencephaly and to state the importance of pregnancy termination in early gestational weeks. An 18-year-old nullipara was admitted to our perinatology service with a diagnosis of neural tube defect. Based on the ultrasonographic findings of alobar holoprosencephaly and iniencephaly during a prenatal screening, termination was recommended at the 13th week of pregnancy. However, she rejected the termination and received no prenatal care until the onset of parturition. At the time of admission, she was in her 28th week of pregnancy. Her medical and family histories were unremarkable. She delivered a stillbirth female weighing 1100 gr complicated with iniencephaly. The infant’s postmortem examination showed iniencephaly associated with holoprosencephaly and cyclops. The family declined an autopsy and genetic counseling. -
Neurocranial Defects with Neuro-Ophthalmic Significance
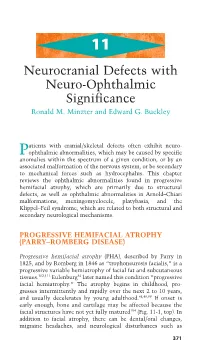
11 Neurocranial Defects with Neuro-Ophthalmic Significance Ronald M. Minzter and Edward G. Buckley atients with cranial/skeletal defects often exhibit neuro- Pophthalmic abnormalities, which may be caused by specific anomalies within the spectrum of a given condition, or by an associated malformation of the nervous system, or be secondary to mechanical forces such as hydrocephalus. This chapter reviews the ophthalmic abnormalities found in progressive hemifacial atrophy, which are primarily due to structural defects, as well as ophthalmic abnormalities in Arnold–Chiari malformations, meningomyelocele, platybasia, and the Klippel–Feil syndrome, which are related to both structural and secondary neurological mechanisms. PROGRESSIVE HEMIFACIAL ATROPHY (PARRY–ROMBERG DISEASE) Progressive hemifacial atrophy (PHA), described by Parry in 1825, and by Romberg in 1846 as “trophoneurosis facialis,” is a progressive variable hemiatrophy of facial fat and subcutaneous tissues.102,111 Eulenburg34 later named this condition “progressive facial hemiatrophy.” The atrophy begins in childhood, pro- gresses intermittently and rapidly over the next 2 to 10 years, and usually decelerates by young adulthood.48,49,99 If onset is early enough, bone and cartilage may be affected because the facial structures have not yet fully matured104 (Fig. 11-1, top). In addition to facial atrophy, there can be dental/oral changes, migraine headaches, and neurological disturbances such as 371 372 handbook of pediatric neuro-ophthalmology A B CD FIGURE 11-1A–D. Progressive nature of progressive hemifacial atrophy (PHA) in a patient at 8 years old (A) and again at 15 years (B), showing left-sided atrophy. Fundus photos of the normal contralateral side (C) and the ipsilateral affected side with hypopigmentary disturbances (D), par- ticularly along the inferior arcade. -

Late Diagnosis Iniencephaly with Spina Bifida
International Journal of Reproduction, Contraception, Obstetrics and Gynecology Chapman DM Int J Reprod Contracept Obstet Gynecol. 2015 Oct;4(5):1543-1545 www.ijrcog.org pISSN 2320-1770 | eISSN 2320-1789 DOI: http://dx.doi.org/10.18203/2320-1770.ijrcog20150741 Case Report Late diagnosis iniencephaly with spina bifida Dilek Marangoz Chapman* Department of Obstetrics & Gynaecology, Vezirkopru State Hospital, Samsun, Turkey Received: 25 August 2015 Revised: 28 August 2015 Accepted: 09 September 2015 *Correspondence: Dr. Dilek Marangoz Chapman, E-mail: [email protected] Copyright: © the author(s), publisher and licensee Medip Academy. This is an open-access article distributed under the terms of the Creative Commons Attribution Non-Commercial License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited. ABSTRACT Herein a rare case of iniencephaly combined with spina bifida is reported, which was diagnosed late because the G6P5 mother had not attended hospital for first trimester anomaly scans and alpha-fetoprotein measurement. A woman aged 33 years who was 38 weeks pregnant presented for ante-natal follow-up. Her clinical results were normal but abnormalities including polyhydramnios, retroflexion of the head with absence of neck, acrania, and severe growth retardation were observed in the fetus. The infant was delivered through Cesarean section and died shortly after birth. The results of a gross examination revealed acrania, iniencephaly, spina bifida, and an imperforated anus. Iniencephaly is a rare and fatal neural tube defect characterized by extreme retroflexion of the head and severs distortion of the spine. This case report underlines the importance of first trimester anomaly scans and alpha- fetoprotein measurement. -

Typical Lesions in the Fetal Nervous System: Correlations Between Fetal Magnetic Resonance Imaging and Obstetric Ultrasonography Findings
Typical lesions in the fetal nervous system: correlations between fetal magnetic resonance imaging and obstetric ultrasonography findings PICTORIAL ESSAY Heron Werner1, Taisa Davaus Gasparetto1, Pedro Daltro1, Emerson Leandro Gasparetto1, https://doi.org/10.14366/usg.17040 2 Edward Araujo Júnior pISSN: 2288-5919 • eISSN: 2288-5943 Ultrasonography 2018;37:261-274 1Department of Radiology, Clínica de Diagnóstico por Imagem (CDPI), Rio de Janeiro; 2Department of Obstetrics, Paulista School of Medicine, Federal University of São Paulo (EPM-UNIFESP), São Paulo, Brazil Received: May 29, 2017 Revised: October 21, 2017 Central nervous system (CNS) malformations play a role in all fetal malformations. Accepted: October 21, 2017 Ultrasonography (US) is the best screening method for identifying fetal CNS malformations. Correspondence to: Edward Araujo Júnior, PhD, Department A good echographic study depends on several factors, such as positioning, fetal mobility and of Obstetrics, Paulista School of growth, the volume of amniotic fluid, the position of the placenta, the maternal wall, the quality Medicine, Federal University of São Paulo (EPM-UNIFESP), Rua Belchior de of the apparatus, and the sonographer’s experience. Although US is the modality of choice for Azevedo, 156 apto. 111 Torre Vitoria, routine prenatal follow-up because of its low cost, wide availability, safety, good sensitivity, São Paulo, CEP 05089-030, Brazil and real-time capability, magnetic resonance imaging (MRI) is promising for the morphological Tel. +55-11-37965944 Fax. +55-11-37965944 evaluation of fetuses that otherwise would not be appropriately evaluated using US. The aim of E-mail: [email protected] this article is to present correlations of fetal MRI findings with US findings for the major CNS malformations. -

Iniencephaly: a Rare Anomaly
THIEME Case Report 43 Iniencephaly: A Rare Anomaly Shantanu B. Chavan1 1Department of Anatomy, R.C.S.M. Government Medical College, Address for correspondence Shantanu B. Chavan, MD (Anat), Kolhapur, Maharashtra, India E-18, Vardhaman Nagar Apartments, 6th Lane, Rajarampuri, Kolhapur 416008, Maharashtra (e-mail: [email protected]). Natl J Clin Anat 2019;8:43–46 Abstract Following case report is an attempt to ascertain that the fetus obtained and evaluated presents with iniencephaly, which is one of the rare variants of neural tube defects. Most of the cases of iniencephaly are reported as isolated incidences. However, some researchers have reported its occurrence in cluster, in a short span of time in a specific population. This case report elaborates various gross anomalies in a fetus which differentiates it from other neural tube defects. The study was performed by Keywords examining the external features as well as the radiograph of the abortus. The study ► neural tube defects also elaborates in brief the different versions of neural tube anomalies which are ► anencephaly sometimes concomitantly observed in the same fetus. Prenatal or postnatal diagnoses ► cervical rachischisis of iniencephaly with or without associated anomalies are suggestive of chromosomal ► prenatal diagnosis abnormalities and in such cases cytogenetic investigations are highly recommended. Introduction the first fetal malformation diagnosed prenatally by Camp- bellet al, using transabdominal ultrasound.3 However, Congenital malformation (CMF) is a physical, metabolic, or iniencephaly (“inion” means the nape of the neck) was first anatomical defect which is apparent before birth, at birth, or reported by Saint-Hilaire in 1836.4 1 detected during the first year of life. -

Prenatal Diagnosis of Congenital Anomalies
PRENATAL DIAGNOSIS OF CONGENITAL ANOMALIES Roberto Romero, M.D. Associate Professor of Obstetrics and Gynecology Director of Perinatal Research Yale University School of Medicine New Haven, Connecticut Gianluigi Pilu, M.D. Attending Physician Section of Prenatal Pathophysiology Second Department of Obstetrics and Gynecology University of Bologna School of Medicine Bologna, Italy Philippe Jeanty, M.D. Assistant Professor Department of Radiology Vanderbilt University Nashville, Tennessee Alessandro Ghidini, M.D. Research Fellow Department of Obstetrics and Gynecology Yale University School of Medicine New Haven, Connecticut John C. Hobbins, M.D. Professor of Obstetrics and Gynecology and Diagnostic Imaging Yale University School of Medicine Director of Obstetrics Yale-New Haven Hospital New Haven, Connecticut APPLETON & LANGE Norwalk, Connecticut/San Mateo, Califomia ©1987-2002 Romero-Pilu-Jeanty-Ghidini-Hobbins 0-8385-7921-3 Notice: Our knowledge in clinical sciences is constantly changing. As new information becomes available, changes in treatment and in the use of drugs become necessary. The author(s) and the publisher of this volume have taken care to make certain that the doses of drugs and schedules of treatment are correct and compatible with the standards generally accepted at the time of publication. The reader is advised to consult carefully the instruction and information material included in the package insert of each drug or therapeutic agent before administration. This advice is especially important when using new or infrequently used drugs. Copyright © 1988 by Appleton & Lange A Publishing Division of Prentice Hall All rights reserved. This book, or any parts thereof, may not be used or reproduced in any manner without written permission. -

Skeletal Anomalies
Donald School Journal of Ultrasound inMachado Obstetrics LE andet al Gynecology, Jan-Mar 2007;1(1):48-72 Skeletal Anomalies Machado LE1, Bonilla-Musoles F2, Obsborne N3, Sanz M2, Raga F2, Machado F1, Bonilla Jr F1, Dolz M2 1INTRO, Salvador (Ba), Brazil 2Department of Obstetrics and Gynecology, Valencia School of Medicine, Spain 3Howard University, Washington INTRODUCTION Thanatophoric dysplasia, the most common lethal osteochondrodysplasia, occurs with an estimated frequency The development of the thorax, the central nervous system of 0.5 and 0.69 cases in 100,00 newborns. A recent study in (CNS) as well as the peripheral nervous system during the Spain reported an incidence of 2.53 to 2.70 cases of intrauterine life is of most importance for the posterior wellbeing achondroplastic dysplasia, but the worldwide frequency is of life, especially because many of their abnormalities are estimated at between 5.0 and 6.9 cases per 100.000 newborns. compatible with life and can create serious disabilities. In other words, one fourth of all congenital skeletal anomalies Therefore, the prenatal diagnosis of these defects, especially are due to thanatophoric dysplasia. the open ones, is essential for the correct neonatal treatment, especially, when the effort is being made to give an intrauterine CLASSIFICATION OF SKELETAL DYSPLASIA surgical solution to some of these abnormalities (myelo- meningocele). Skeletal dysplasia is frequently associated with limb The neurological postnatal prognosis will depend, malformations. Although they are usually divided into five therefore, on the intrauterine diagnosis as early as possible, of: different types, a universally accepted classification is still • The vertebral level where the medullar injury is located lacking, mainly because of a lack of uniformity in the criteria (Iniencephaly) used for diagnosis. -

Magnetic Resonance Imaging in the Prenatal Diagnosis of Neural Tube Defects
Insights Imaging (2013) 4:225–237 DOI 10.1007/s13244-013-0223-2 PICTORIAL REVIEW Magnetic resonance imaging in the prenatal diagnosis of neural tube defects A. Zugazaga Cortazar & C. Martín Martinez & C. Duran Feliubadalo & M. R. Bella Cueto & L. Serra Received: 22 October 2012 /Revised: 7 January 2013 /Accepted: 10 January 2013 /Published online: 1 March 2013 # The Author(s) 2013. This article is published with open access at Springerlink.com Abstract Key Points Objective To assess the role of magnetic resonance imaging • To learn about the normal anatomy of the neural tube on MRI (MRI) in the prenatal diagnosis of neural tube defects (NTDs). • To recognise the MR appearance of neural tube defects Background NTDs comprise a heterogeneous group of con- • To understand the value of MRI in assessing NTDs genital anomalies that derive from the failure of the neural tube to close. Advances in ultrasonography and MRI have Keywords Prenataldiagnosis .Magneticresonanceimaging . considerably improved the diagnosis and treatment of NTDs Congenital abnormalities . Neural tube defects . Spinal both before and after birth. Ultrasonography is the first dysraphism technique in the morphological study of the fetus, and it often makes it possible to detect or suspect NTDs. Fetal MRI is a complementary technique that makes it possible to Introduction clear up uncertain ultrasonographic findings and to detect associated anomalies that might go undetected at ultraso- Technological developments in diagnostic imaging have nography. The progressive incorporation of intrauterine improved the diagnosis and treatment of congenital anoma- treatments makes an accurate diagnosis of NTDs essential lies immensely, and this progress is especially evident in to ensure optimal perinatal management.