The Policies and Production in Maternal Mortality Reduction in Cross
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Human Migratory Pattern: an Appraisal of Akpabuyo, Cross River State, Nigeria
IOSR Journal Of Humanities And Social Science (IOSR-JHSS) Volume 22, Issue 7, Ver. 16 (July. 2017) PP 79-91 e-ISSN: 2279-0837, p-ISSN: 2279-0845. www.iosrjournals.org Human Migratory Pattern: An Appraisal of Akpabuyo, Cross River State, Nigeria. 1Iheoma Iwuanyanwu, 1Joy Atu (Ph.D.), 1Chukwudi Njoku, 1TonyeOjoko (Arc.), 1Prince-Charles Itu, 2Frank Erhabor 1Department of Geography and Environmental Science, University of Calabar, Calabar, Cross River State, Nigeria 2Department of Geography and Environmental Management, Ahmadu Bello University, Zaria, Kaduna State, Nigeria Corresponding Author: IheomaIwuanyanwu ABSTRACT: This study assessed migration in Akpabuyo Local Government Area (LGA) of Cross River State, Nigeria. The source regions of migrants in the area were identified; the factors that influence their movements, as well as the remittances of migrants to their source regions were ascertained. A total of 384 copies of questionnaires were systematically administered with a frequency of 230 and 153 samples for migrants and non-migrants respectively. Amongst other findings from the analyses, it was established that Akpabuyo is home to migrants from other LGAs and States, especially BakassiLGA and EbonyiState. There were also migrants from other countries such as Cameroon and Equatorial Guinea. The Pearson‟s correlation analysis depicted significant relationship (P = 0.012) between distance to Akpabuyo and the number of migrants that come into the area, implying that distance significantly influences migration to Akpabuyo. Furthermore, the Correspondence Analysis (CA) showed a weak association between the pull and push factors in the area, buttressed by the chi-square testwhich showed insignificant statistical similarity (p = 0.118). It was also established that migrants remitted 74% of their income to their source regions. -

Print This Article
European Journal of Social Sciences Studies ISSN: 2501-8590 ISSN-L: 2501-8590 Available on-line at: www.oapub.org/soc doi: 10.5281/zenodo.3866894 Volume 5 │ Issue 2 │ 2020 REFUGEE INFLUX: A SOCIOLOGICAL INSIGHT AND EMPIRICAL ANALYSIS OF ITS CONCOMITANT EFFECT ON FOOD SECURITY IN ETUNG CROSS RIVER STATE, NIGERIA Omang, Thomas A.1, Ojong-Ejoh, Mary U.2, Bisong Kenneth B.3, Egom Njin O.4 1&2Department of Sociology, University of Calabar, Cross River State, Nigeria 3Institute of Public Administration, University of Calabar, Cross River State, Nigeria 4Graduate Student, University of Abuja, Nigeria Abstract: The study examines the impact of Cameroun refugee influx and its impact on food security in Etung Local Government Area of Cross River State, Nigeria. The study adopted the survey research method in eliciting information from 400 samples from two political wards in Etung Local Government Area of Cross River State, Nigeria, using the purposive and random sampling technique. a self-administered structured questionnaire was the instrument of Data collection. Data gathered from the field was meticulously collated, coded and analyzed using simple percentages, frequency distribution, figures and simple lineal regression at 0.05 confidence level. Result revealed that there is a significant relationship between refugee influx and Food Security in Etung Local Government Area of Cross River State, Nigeria. The study recommends That the Cross- River state synergizes with the relevant agencies of the Federal Government as well as other international Agencies to stimulate production in Etung through agricultural programs such as farmers smallholders schemes, cassava, banana, yam, plantain plantations schemes, animal husbandry, cottage industries etc. -

Cross River STATE-WIDE RAPID HEALTH FACILITY ASSESSMENT
Report of the Cross River STATE-WIDE RAPID HEALTH FACILITY ASSESSMENT In Preparation for Elimination of Mother-to-Child Transmission of HIV March 2013 Report of the Cross River STATE-WIDE RAPID HEALTH FACILITY ASSESSMENT In Preparation for Elimination of Mother-to-Child Transmission of HIV May 2013 This publication may be freely reviewed, quoted, reproduced, or translated, in full or in part, provided the source is acknowledged. The mention of specific organizations does not imply endorsement and does not suggest that they are recommended by the Cross River State Ministry of Health over others of a similar nature not mentioned. Copyright © 2013 Cross River State Ministry of Health, Nigeria Citation: Cross River State Ministry of Health and FHI 360. 2013. Cross River State-wide Rapid Health Facility Assessment, Nigeria: Cross River State Ministry of Health and FHI 360. The Cross River State-wide Rapid Health Facility Assessment was supported in part by the U.S. Agency for International Development (USAID). FHI 360 provided assistance to the Cross River State Government to conduct this assessment. Financial assistance was provided by USAID under the terms of the Cooperative Agreement AID-620-A-00002, of the Strengthening Integrated Delivery of HIV/ AIDS Services Project. This report does not necessarily reflect the views of FHI 360, USAID or the United States Government. Table of Contents Foreword ...................................................................................................................................................................................................... -

Nigeria - Accessibility to Emonc Facilities in the State of Cross River
Nigeria - Accessibility to EmONC facilities in the State of Cross River Last Update: March 2016 Nigeria - Accessibility to EmONC facilities for the Cross River State Table of Contents Acknowledgements ..................................................................................................................... 4 1. Introduction ............................................................................................................................. 5 2. Measured indicators and assumptions .................................................................................... 5 3. Tool used for the different analyses: AccessMod 5.0 ............................................................. 7 4. Data and national norms used in the different analyses .......................................................... 8 4.1 Statistical Data ............................................................................................................... 9 4.1.1 LGA Number of pregnant women for 2010 and 2015 ........................................... 9 4.2 Geospatial Data ........................................................................................................... 12 4.2.1 Administrative boundaries and extent of the study area ...................................... 13 4.2.2 Geographic location of the EmONC facilities and associated information ......... 17 4.2.4 Transportation network ........................................................................................ 26 4.2.5 Hydrographic network ........................................................................................ -
Cross River State
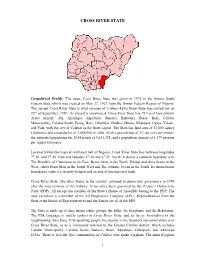
CROSS RIVER STATE Geopolitical Profile: The name Cross River State was given in 1976 to the former South Eastern State which was created on May 27, 1967 from the former Eastern Region of Nigeria. The current Cross River State is what remains of it when Akwa Ibom State was carved out on 23rd of September, 1987. As presently constituted, Cross River State has 18 Local Government Areas namely; Abi, Akamkpa, Akpabuyo, Bakassi, Bekwarra, Biase, Boki, Calabar Municipality, Calabar South, Etung, Ikom, Obanliku, Obubra, Obudu, Odukpani, Ogoja, Yakurr, and Yala; with the city of Calabar as the State capital. The State has land area of 23,000 square kilometres and a population of 2,888,966 in 2006. With a growth rate of 2.9 per cent per annum, the estimated population for 2014 stands at 3,631,328, and a population density of 1,579 persons per square kilometre. Located within the tropical rainforest belt of Nigeria, Cross River State lies between longitudes 7⁰ 50’ and 9⁰ 28’ East and latitudes 4⁰ 28’and 6⁰ 55’ North. It shares a common boundary with The Republic of Cameroun in the East, Benue State in the North, Ebonyi and Abia States in the West, Akwa Ibom State in the South West and The Atlantic Ocean in the South. Its international boundaries make it a security hotspot and an axis of international trade. Cross River State, like other States in the country, returned to democratic governance in 1999 after the interventions of the military. It has since been governed by the People’s Democratic Party (PDP). -

Cameroonian Refugee Situation, Nigeria 1 6 - 31 October 2018
EMERGENCY UPDATE Cameroonian refugee situation, Nigeria 1 6 - 31 October 2018 135 permanent shelters for 1,636 Cameroonian refugees 90 refugees from Adagom and refugees have been completed and 252 members of the host Anyake settlements completed in Adagom settlement (Cross community received free vocational training on River state). health care services in Anyake vegetable farming and small settlement (Benue state). plots of land were allocated to set up a small vegetable production. K EY INDICATORS 29,078 Cameroonian refugees registered with Level 1 and Level 2 registration [As of 30th October 2018] 2,999 Cameroonian refugees registered in Anyake settlement, Benue State [as of 31st October 2018] 4,997 Cameroonian refugees registered in Adagom settlement, st Eva Caroline (right), and her family arrived at the end of October Cross River State [as of 31 October 2018] 2018 in Amana, Obanliku LGA, Cross River state. They initially fled to another village within Cameroon but the conflict reached them there so they crossed into Nigeria. © UNHCR/C. Cavalcanti Operational Context ■ Cameroonian refugees continued to arrive in Nigeria albeit in limited numbers through unofficial entry points mainly on foot, motorcycles and canoes as official borders remained closed. Some 340 new arrivals were verified by UNHCR in the border localities of Obanliku, Ikom, Etung and Boki Local Government Areas (Cross River state) during the reporting period. Most new arrivals reported an increase in the attacks to villages to drive out combatants, including in villages not reached by the conflict before, where many Cameroonians had moved in search of safety and they are now pushed to cross into Nigeria. -

Journal of Agriculture and Crops Allocative and Technical
Journal of Agriculture and Crops ISSN(e): 2412-6381, ISSN(p): 2413-886X Vol. 4, Issue. 6, pp: 68-72, 2018 Academic Research Publishing URL: http://arpgweb.com/?ic=journal&journal=14&info=aims Group Original Research Open Access Allocative and Technical Efficiencies Among Small Holder Cocoyam Farmers in Cross River State Central Agricultural Zone, Nigeria Ettah Otu I.* Department of Agricultural Economics, Faculty of Agriculture, Forestry and Wildlife Resources Management, University of Calabar, PMB 1115 Calabar, Nigeria Ani Stella O. Department of Agricultural Economics, Faculty of Agriculture, University of Nigeria, Nsukka, Nigeria Abstract The authors investigated the allocative and technical efficiencies of resources used in cocoyam production among small scale farmers in Central Agricultural Zone of Cross River State, Nigeria. The objectives of the study were to: determine the allocative efficiency of resources used in cocoyam production in the area and determine also the technical efficiency of resources used in cocoyam production in the area. Primary data were used to conduct the study. Statistical tools employed were allocative efficiency index (AEI) and stochastic frontier production function (SFPF). Results of the allocative efficiency index showed that farm size (x1), fertilizer (x3) and herbicide (x5) were all found to be grossly underutilized since their allocative efficiency index were greater than one (1) and their marginal value product (MVP) were greater than their marginal factor cost (MFC). However, Labour (x2) alone was over-utilized. The following were recommended cocoyam farmers are advised to improve on their use of farm resources like land, fertilizer, herbicide and seeds as they were found to be under-utilized and labour should be controlled in such a way that it can be used in other farm enterprises. -

16 the Impact of Religion, Culture and World View Of
International Journal of African Society, Cultures and Traditions Vol.8, No.1, pp.16-37, June 2020 Published by ECRTD-UK Print ISSN: ISSN 2056-5771(Print) Online ISSN: ISSN 2056-578X (Online) THE IMPACT OF RELIGION, CULTURE AND WORLD VIEW OF THE PEOPLE OF CROSS RIVER STATE ON THE SLOW GROWTH OF SEVENTH-DAY (SDA) CHURCH MISSION IN THE STATE 1Eko, Enebieni Enebieni, Ph. D Department of Religious Studies Clifford University P. M. B: 8001 2Ekpenyong, Ekpenyong Obo, Ph. D Department of Religious and Cultural Studies University Of Calabar P. M. B: 1115 ABSTRACT: The research looks at the impact of religion, culture and worldview of the people of Cross River State on the spread of the Seventh-day Adventist Church in Cross River State. To realize this, three (3) point purpose of the study was considered, data were collected from the field-work and the study employed statistical, sociological, historical and theological methods in analyzing its data. From the investigation conducted on this study, it is apparent that the following are the major factors impacted on the slow growth of the Seventh-day Adventist Church in Cross River State, namely: Religio-Cultural Factors and Church Growth; Socio-Economic Factor and Church Growth, and Religious Factors and Church Growth. This recommended church organization can be understood through the adoption of the under-listed missiological approaches: Incarnation, Inculturation, and Contextualization of the gospel, in addition to Inclusive Community Paradigm in reaching out to the people of Cross River State. KEYWORDS: worldview, religion, culture, church growth. INTRODUCTION The name, Cross River State, came from Cross River, one of the major geo-physical features in the State. -

NIGERIA INDEPENDENCE in the UPPER CROSS RIVER REGION: PEOPLES’ EXPECTATIONS and FEELINGS Dr
International Journal of Multidisciplinary Research and Modern Education (IJMRME) ISSN (Online): 2454 - 6119 (www.rdmodernresearch.org) Volume II, Issue I, 2016 NIGERIA INDEPENDENCE IN THE UPPER CROSS RIVER REGION: PEOPLES’ EXPECTATIONS AND FEELINGS Dr. Chinyere S. Ecoma Department of History and International Relations, Veritas University, Abuja, Abuja- Nigeria Abstract: Situated within the present Cross River State of Nigeria, in this study, the Upper Cross River covers the entire northern half of the State comprising Biase, Ugep, Obubra, Ikom, Ogoja and Obudu administrative divisions. This unique setting experienced colonial rule with its attendant socio-cultural, educational and other legacies under the former Eastern Region, until independence was granted to Nigeria on October 1, 1960. The general impression is that independence was widely embraced with a lot of euphoria throughout the country. Recent research reveals that the picture was variegated and that numerous factors conditioned peoples’ response to the event. These factors include the existing communication profile, remoteness of the area from the centres where the main celebrations took place, the age and occupation of respondents in a locality, and the peculiarities of different areas. However, with the emancipation story, some respondents dreamt dreams of high expectations for Nigeria. The thrust of this paper is to examine the response of people in this region to the attainment of independence by Nigeria on October 1, 1960 and to explain why they reacted the way they did. Keywords: Nigeria, Independence, Upper Cross River Region & Expectations. 1. Introducing the Upper Cross River Region of Nigeria: Situated within the present Cross River State of Nigeria, the Upper Cross River Region (UCRR) (see Figure 1) occupies the entire Northern half of Cross River State lying between latitudes 4° 30 7°, and, longitudes 7° 30 and 9° east of the equator (Erim: 1990: 40). -

Government of Cross Rivers State of Nigeria HIV/AIDS Programme
Government of Cross Rivers State of Nigeria HIV/AIDS Programme Development Project (World Bank Assisted) Cross Rivers State Agency for the Control of Aids (CRSACA) No 4, Barracks Road by Eyo Eta Line Calabar, Cross River State E-mail: [email protected]; [email protected] Request for Expressions of Interest (IDA CREDIT/GRANT No. CR-4596-NG) CRS/HPDP II/Eol/CON/2012/03 Advertisement for Civil Society Organizations (CSOs) including Non Government Organizations, Faith Based Organisations, Private Sector Organisations Umbrella Organizations to Provide HIV/AIDS Related Services. Issuance Date: 14th November, 2012. The Cross Rivers Agency for the Control of AIDS (CRSACA) has received financing from World Bank toward the cost of the Second HIV/AIDS Programme Development Project (HP0P2) and intends to apply part of the proceeds for consultant services. 1. 1. Assignment Description & Services Requested (Scope of Work) This is a call for Expression of Interest from qualified and competent organizations (Civil Society Organizations (CSOs) including Non Government Organizations. Faith Based Organizations, Private Sector Organisations and Umbrella Organizations) lo provide support to Cross River SACA in implementing the HIV/AIDS Fund (HAF). The focus is on prevention of new HIV infections and is for an initial two years Organizations are expected to identify and work with any or all specified target populations within the specified geographic coverage areas to deliver, evidence based HIV intervention packages in line with international standard and best practices. 1. Most At Risk Population (MARPS).The target population are; 2. i. Female Sex Workers (FSW), Geographical Area: Calabar South, Abi, Akamkpa, Akpabuyo, Bakassi, Boki, obudu, Yakurr, Ikom, Bekwarra, Odukpani, Biase, Ogoja, & Yala. -

Language and Power in Cross River State, Nigeria
ISSN 2039-2117 (online) Mediterranean Journal of Social Sciences Vol 5 No 10 ISSN 2039-9340 (print) MCSER Publishing, Rome-Italy June 2014 Language and Power in Cross River State, Nigeria Mercy Ugot, Ph.D Department of Language and Linguistic Science Cross River University of Technology, Calabar, Cross River State Nigeria E-mail: [email protected] Mathew Nsing Ogar, Ph.D Department of Curriculum and Instructional Technology Cross River University of Technology, Calabar, Nigeria Email: [email protected] Doi:10.5901/mjss.2014.v5n10p648 Abstract This work focuses on the languages of Cross River State and their relative relevance in the state. Cross River State is a multilingual state with many of Nigeria’s minority languages to be found within it. The paper examines the relative status and functions of the languages in use in the state and their relevance to affairs of the state. The languages have been seen to be state languages, Local Government Area (LGA) languages while others do not have any functional status. Coupled with other non-indigenous languages in the state, some languages are official; others are second languages, lingua francas, trade languages etc. in importance. They are used in the domain of administration, politics, education, trade etc. in the state. For the other indigenous languages in particular, it is suggested that though they are not state languages and are not in use outside of their immediate environment, they should be developed in order to maintain the identity and history of the people. Keyword: Language, power, multilingualism, language policy 1. Introduction Cross River State is one of the 36 states of the Federal Republic of Nigeria and located within the South-South geo- political zone of Nigeria. -
Cameroon SITUATION UPDATE / NIGERIA OPERATION
Cameroon SITUATION UPDATE / NIGERIA OPERATION Cameroon Situation Ju ly 2019 41,087 Cameroonian refugees 3,500 new refugees were UNHCR launched a are registered in Akwa-Ibom, registered in Nigeria during the Supplementary Appeal of Benue, Cross River and Taraba month of July. UNHCR seeks $27.3 M in new requirements to States in Nigeria. funding to provide them with provide food, shelter and basic assistance and protection. needs to Cameroonian refugees in Nigeria. KEY INDICATORS 41,087 | Cameroonian refugees are registered in Nigeria 20,250 | Cameroonian refugees are registered in the Adagom, Okende settlements in Cross River State and in the Anyake settlement in Benue State. 50% | Of Cameroonian refugees in Nigeria live in host communities Some 14 refugee families (82 individuals) live under this hangar provided by UNHCR at the Adagom refugee settlement, Cross River State. When it rains at night they have to stand up as the rains flood the floor. © UNHCR/Tony Aseh 1 Cameroon SITUATION UPDATE / NIGERIA OPERATION Highlights ■ The United Nations Country Team (UNCT) held a retreat in Calabar, Cross River State (CRS) from 11 to 12 July that discussed the current implementation of the Sustainable Development Goals in Nigeria, proposed effective ways of addressing the gender gap in decision-making positions, and suggested sustainable ways to address problems that affect the youth, including unemployment and substance abuse. Senior UNCT members, including Mr Edward Kallon, UN Resident Coordinator, Prof. Ivara Esu, Deputy Governor of CRS, and other Government officials took part in the meeting ■ UNHCR partner, FHI360, undertook 10 advocacy visits with Government officials in Benue and Cross River to solicit support for the UNHCR Health and Nutrition interventions for Cameroonian Refugees.