National Tuberculosis Andf Leprosy Program
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

HIV/AIDS Treatment and Care in a Long-Term Conflict Setting: Observations from the AIDS Support Organization (TASO) in the Teso Region Emma Smith SIT Study Abroad
SIT Graduate Institute/SIT Study Abroad SIT Digital Collections Independent Study Project (ISP) Collection SIT Study Abroad Spring 2008 HIV/AIDS Treatment and Care in a Long-Term Conflict Setting: Observations From The AIDS Support Organization (TASO) in the Teso Region Emma Smith SIT Study Abroad Follow this and additional works at: https://digitalcollections.sit.edu/isp_collection Recommended Citation Smith, Emma, "HIV/AIDS Treatment and Care in a Long-Term Conflict Setting: Observations From The AIDS Support Organization (TASO) in the Teso Region" (2008). Independent Study Project (ISP) Collection. 99. https://digitalcollections.sit.edu/isp_collection/99 This Unpublished Paper is brought to you for free and open access by the SIT Study Abroad at SIT Digital Collections. It has been accepted for inclusion in Independent Study Project (ISP) Collection by an authorized administrator of SIT Digital Collections. For more information, please contact [email protected]. HIV/AIDS Treatment and Care in a Long-Term Conflict Setting: Observations from The AIDS Support Organization (TASO) in the Teso Region Emma Smith Advisor: Alutia Samuel Academic Directors: Charlotte Mafumbo and Martha Wandera Location: TASO Soroti SIT Uganda Spring 2008 Dedication To all the people living with HIV/AIDS in Teso, who continue to live strongly despite decades of suffering from continuous war, displacement and neglect. May the world come to recognize the struggles that you live with. Acknowledgements There are so many people to whom thanks is owed, it would not be possible to acknowledge them all even if time and space allowed. Primarily, I would like to thank the clients of TASO Soroti, who so willingly welcomed a stranger into their communities and allowed so many questions to be asked of them. -

WHO UGANDA BULLETIN February 2016 Ehealth MONTHLY BULLETIN
WHO UGANDA BULLETIN February 2016 eHEALTH MONTHLY BULLETIN Welcome to this 1st issue of the eHealth Bulletin, a production 2015 of the WHO Country Office. Disease October November December This monthly bulletin is intended to bridge the gap between the Cholera existing weekly and quarterly bulletins; focus on a one or two disease/event that featured prominently in a given month; pro- Typhoid fever mote data utilization and information sharing. Malaria This issue focuses on cholera, typhoid and malaria during the Source: Health Facility Outpatient Monthly Reports, Month of December 2015. Completeness of monthly reporting DHIS2, MoH for December 2015 was above 90% across all the four regions. Typhoid fever Distribution of Typhoid Fever During the month of December 2015, typhoid cases were reported by nearly all districts. Central region reported the highest number, with Kampala, Wakiso, Mubende and Luweero contributing to the bulk of these numbers. In the north, high numbers were reported by Gulu, Arua and Koti- do. Cholera Outbreaks of cholera were also reported by several districts, across the country. 1 Visit our website www.whouganda.org and follow us on World Health Organization, Uganda @WHOUganda WHO UGANDA eHEALTH BULLETIN February 2016 Typhoid District Cholera Kisoro District 12 Fever Kitgum District 4 169 Abim District 43 Koboko District 26 Adjumani District 5 Kole District Agago District 26 85 Kotido District 347 Alebtong District 1 Kumi District 6 502 Amolatar District 58 Kween District 45 Amudat District 11 Kyankwanzi District -

Assessing the Impact of the Peace, Recovery and Development Plan 1 in Northern Uganda
WE SAW WHAT WAS DONE BUT NOT OUR WILL WAS DONE: ASSESSING THE IMPACT OF THE PEACE, RECOVERY AND DEVELOPMENT PLAN 1 IN NORTHERN UGANDA © Refugee Law Project, June 2013 The Advisory Consortium on Conflict Sensitivity (ACCS) This report is a product of the Advisory Consortium on Conflict Sensitivity (ACCS), a three member partnership between International Alert, Refugee Law Project and Saferworld. The overall aim of ACCS is to assist the British Department for International Development (DfID) and partners in strengthening the potential of the PRDP to address the causes of conflict in a way that is itself conflict sensitive, and which can contribute to sustainable peace and stability. ACCS has three major objectives: monitoring of the extent to which interventions under the Peace, Recovery and Development Plan (PRDP), particularly those funded under DFID’s Post-Conflict Development Programme (PCDP), succeed or fail in achieving peacebuilding aims (International Alert); contextual analysis of the overall recovery process (conflict indicators, issues and dynamics) and to provide early warning as and when necessary (RLP); and evidence-based advocacy, targeted recommendations, and technical support to improve the recovery and peacebuilding impact of OPM and other PRDP stakeholders (Saferworld). Each con sortium agency leads on one output, supported by the other partners. 2 Acknowledgments This report was authored by an independent consultant, Jamie Hitchen. He is indebted to the work of Martin Kasozi, Dennis Jjuuko and Jimmy Wamimbi who worked tirelessly in collection data from the field and in providing a peer review on the initial draft. Eunice Ouko who provided field contacts for interviews and all ACCS members Jackson Odong, Barnabas Otim and staff of the Conflict, Transitional Justice and Governance Programme at RLP for their support throughout the research. -
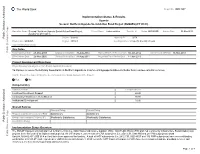
Implementation Status & Results
The World Bank Report No: ISR13907 Implementation Status & Results Uganda Second Northern Uganda Social Action Fund Project (NUSAF2) (P111633) Operation Name: Second Northern Uganda Social Action Fund Project Project Stage: Implementation Seq.No: 8 Status: ARCHIVED Archive Date: 03-May-2014 (NUSAF2) (P111633) Public Disclosure Authorized Country: Uganda Approval FY: 2009 Product Line:IBRD/IDA Region: AFRICA Lending Instrument: Specific Investment Loan Implementing Agency(ies): Key Dates Public Disclosure Copy Board Approval Date 28-May-2009 Original Closing Date 31-Aug-2014 Planned Mid Term Review Date 30-Jan-2012 Last Archived ISR Date 19-Nov-2013 Effectiveness Date 25-Nov-2009 Revised Closing Date 31-Aug-2014 Actual Mid Term Review Date 14-Jun-2013 Project Development Objectives Project Development Objective (from Project Appraisal Document) To improve access of beneficiary households in Northern Uganda to income earning opportunities and better basic socio-economic services. Has the Project Development Objective been changed since Board Approval of the Project? Yes No Public Disclosure Authorized Component(s) Component Name Component Cost Livelihood Investment Support 60.00 Community Infrastructure Rehabilitation 30.00 Institutional Development 10.00 Overall Ratings Previous Rating Current Rating Progress towards achievement of PDO Satisfactory Satisfactory Overall Implementation Progress (IP) Moderately Satisfactory Moderately Satisfactory Public Disclosure Authorized Overall Risk Rating Implementation Status Overview The NUSAF II project originally planned to finance 9750 (i.e. 8000 Household Income Support (HIS), 1000 Public Works (PW) and 750 Community Infrastructure Rehabilitation) sub projects in the five year of its implementation period. As of February 3, 2013 a total of 8,764 subprojects (i.e. -

Bi-Monthly Update 01-19 June 2007
HEALTH ACTION IN CRISES, UGANDA Bi-Monthly Update 01-19 June 2007 WHO- Health Action in Crisis (HAC) programme carried out the following activities during the first two weeks of June 2007: Health systems strengthening Village Health Teams • Kitgum: The VHT/ CORPS Core team meeting was held to discuss the involvement of partners in the training and support of the Village Health Team program. It was agreed that a mapping of community health volunteers trained by the different partners would be carried out, followed by sub-county sensitization, selection of VHT members and training of VHT members. • Pader: The community Co-Artem program is ongoing in 7 of the 18 sub counties. Additional sub counties are expected to be enrolled in the coming weeks depending on the availuability of the registration books or other acceptable record books. CBDS Roll out in Kitgum: CBDS training was conducted in 2 sub-counties of Padibe East and Padibe West from 11 - 15 June 2007. A total of 146 Community surveillance focal persons [86 from Padibe East and 60 from Padibe West] were trained. The total number of CBDS trained in Kitgum district now stands at 556. Roll out CBDS will continue in Lokung sub-county next week, targeting 108 community surveillance focal persons. Below is the summary table of trained CBDS in Kitgum. Sub-county Camp Total Population No. House holds No. of Villages No. of CBDS Trained Akwang Akwang 17,619 4,017 21 42 Omia-Anyima Omiya-Anyima 17,610 3,764 54 108 Paloga Paloga 6,944 1,722 27 54 Madi-Opei Madi Opei 11,135 2,691 25 50 Palabek Kal Palabek Kal 21,575 10,399 31 62 Palabek Gem Palabek Gem 11,731 5,654 29 58 Madi-Kiloch 18 36 Padibe West 17,630 4,042 Padibe West 30 60 Padibe East Padibe East 17,376 4,164 43 86 Total 556 VHTs receive registers, medicine, medicine boxes, gum boots & t-shirts. -
(4) of the Constitution Providing for Creation of New Counties
AMMENDED MOTTON FOR RESOLUTTON OF PARLTAMENT UNDER ARTTCLE 179 (4) OF THE CONSTITUTION PROVIDING FOR CREATION OF NEW COUNTIES WHEREAS, Ariicle 179 (a) of the Constitution of the Republic of Ugondo (os omended) provides for the criterio for olterotion of boundories oflor creotion of Administrotive Units including new Counties; AND WHEREAS Section 7 (7) of the Locql Governments Act Cop. 243, (os omended) empowers Porlioment to opprove olternotion of Boundories of/or creotion of o new County; Honoroble Colleogues willTHUS, recoll thot on Tuesdoy 30rn June, 2020,1 moved o motion on the floor of Porlioment for creotion of I5 (Fitteen) Counties thot were opproved by Cobinet hoving received requests from the District Councils of; Kiboole, Kotokwi, Agogo, lsingiro, Kisoro, Nokoseke, Kibogo, Buhweju, Lomwo, Kokumiro, Nokopiripirit, Mubende, Kwonio, Tororo ond Jinjo to creote the following Counties: - l) Buyanja Eost County out of Buyanjo County in Kibaale Distric[ 2) Ngoriom Covnty out of Usuk County in Kotakwi; 3) Agago Wesf County out of Agogo County in Agogo District; 4) Bukonga Norfh County out of Bukongo County in lsingiro District; 5) Bukimbiri County out of Bufumbira County in Kisoro District; 6) Nokoseke Centrol County out of Nokoseke Norfh County in Nokoseke Disfricf 7) Kibogo Wesf County out of Kibogo Eost County in Kbogo District; B) Buhweju West County aut of Buhweju County in Buhweju District; 9) Palobek County out of Lamwo County in Lamwo District; lA)BugongoiziSouth County out of BugongoiziWest County in Kokumiro Districf; I l)Chekwi Eosf County out of Chekwi County in Nokopiripirit District; l2)Buweku/o Soufh County out of Buweku/o County in Mubende Disfricf, l3)Kwanio Norfh County out of Kwonio Counfy in Kwonio Dislricf l )West Budomo Central County out of Wesf Budomo County inTororo Districf; l5)Kogomo Norfh County out of Kogomo County in Jinjo Districf. -
Use of Pyrethroids and Amidines Against Tsetse and Ticks in Zoonotic Sleeping Sickness Endemic Areas of Uganda Kevin Bardosh1, Charles Waiswa2 and Susan C Welburn3*
Bardosh et al. Parasites & Vectors 2013, 6:204 http://www.parasitesandvectors.com/content/6/1/204 RESEARCH Open Access Conflict of interest: use of pyrethroids and amidines against tsetse and ticks in zoonotic sleeping sickness endemic areas of Uganda Kevin Bardosh1, Charles Waiswa2 and Susan C Welburn3* Abstract Background: Caused by trypanosomes and transmitted by tsetse flies, Human African Trypanosomiasis and bovine trypanosomiasis remain endemic across much of rural Uganda where the major reservoir of acute human infection is cattle. Following elimination of trypanosomes by mass trypanocidal treatment, it is crucial that farmers regularly apply pyrethroid-based insecticides to cattle to sustain parasite reductions, which also protect against tick-borne diseases. The private veterinary market is divided between products only effective against ticks (amidines) and those effective against both ticks and tsetse (pyrethroids). This study explored insecticide sales, demand and use in four districts of Uganda where mass cattle treatments have been undertaken by the ‘Stamp Out Sleeping Sickness’ programme. Methods: A mixed-methods study was undertaken in Dokolo, Kaberamaido, Serere and Soroti districts of Uganda between September 2011 and February 2012. This included: focus groups in 40 villages, a livestock keeper survey (n = 495), a veterinary drug shop questionnaire (n = 74), participatory methods in six villages and numerous semi-structured interviews. Results: Although 70.5% of livestock keepers reportedly used insecticide each month during the rainy season, due to a variety of perceptions and practices nearly half used products only effective against ticks and not tsetse. Between 640 and 740 litres of insecticide were being sold monthly, covering an average of 53.7 cattle/km2. -

Ateso Grammar: a Descriptive Account of an Eastern Nilotic Language
Ateso Grammar: A Descriptive Account of an Eastern Nilotic Language David Barasa Thesis presented for the Degree of DOCTOR OF PHILOSOPHY in Linguistics UNIVERSITY OF CAPE TOWN 15th March, 2017 Supervised by: Prof. Ana Deumert Dr. Mantoa Smouse University of Prof. Cape Gerrit Dimmendaal Town Dr. Helga Schroeder The copyright of this thesis vests in the author. No quotation from it or information derived from it is to be published without full acknowledgementTown of the source. The thesis is to be used for private study or non- commercial research purposes only. Cape Published by the University ofof Cape Town (UCT) in terms of the non-exclusive license granted to UCT by the author. University Declaration I declare that “Ateso Grammar: A Descriptive Account of an Eastern Nilotic Language” is my own work. Each significant contribution to, and quotation in, this thesis from the work, or works, of other people has been attributed, and has been cited and referenced. Signature: Date: 15th March, 2017 ii Abstract This study discusses the structure of Ateso, an Eastern Nilotic language. Based on interview and recorded data from fieldwork conducted in both Uganda and Kenya, where Ateso is spoken, the study provides the first comprehensive description of the phonology, morphology and syntax of the language. The main findings of this study are as follows: The key feature of Ateso’s phonological structure is that vowel alternation strategies are constrained by three harmony rules: root-control, feature-control, and, finally, mid-vowel assimilation. While Ateso shares this structure with the other Eastern Nilotic languages, it has its unique features as well. -

National Internally Displaced Persons Return, Resettlement and Re-Integration Strategic Plan for Lango and Teso Sub Regions
NATIONAL INTERNALLY DISPLACED PERSONS RETURN, RESETTLEMENT AND RE-INTEGRATION STRATEGIC PLAN FOR LANGO AND TESO SUB REGIONS November 2005 Table of Contents Page Introduction Budget Summary ANNEX Component 1 Lira and Amolatar Districts IDP return plan Component 2 Apac District IDP Return Plan Component 3 Katakwi and Amuria Districts IDP Return plan Component 4 Soroti District IDP Return Plan Component 5 Kaberamaido District IDP Return Plan INTRODUCTION 1. Background Recent political and military developments in Northern Uganda have generated optimism for the IDP return process to begin. These include the Southern Sudan peace process, the renewed diplomatic relation between Sudan and Uganda, under which the latter is allowed to pursue the LRA rebels into the former’s territory (Operation Iron Fist II) and the efforts for peaceful agreement between LRA and government brokered by Mrs Betty Bigombe. From July 2004, there has been a marked improvement in the general security situation in the Northern Uganda Districts evidenced by the high rates of LRA desertions which is partly as a result of increased pressure from the UPDF supported by the auxiliary forces and the people, and also as a result of the government amnesty to insurgents who renounce war. In August 2004, Cabinet approved a National Policy for Internally Displaced Persons, which establishes principles for provision of assistance to IDPs while in the camps and procedures for their return and resettlement. In the policy, Government committed itself to ending the insurgency and facilitating the voluntary return, resettlement and re-integration of the IDPs. By October 2004, the LRA capacities to attack civilians became less frequent in Acholiland, and virtually ended in Teso and Lango sub regions except for some few isolated incursions that have been effectively contained. -
Kaberamaido District Hazard, Risk and Vulnerability Profile June 2014
THE REPUBLIC OF UGANDA TESO KABERAMAIDO District Hazard, risk and Vulnerability Profile June 2014 KABERAMAIDO DISTRICT HAZARD, RISK AND VULNERABILITY PROFILE | A With support from: United Nations Development Programme Plot 11, Yusuf Lule Road P.O. Box 7184 Kampala, Uganda For more information: www.undp.org B | KABERAMAIDO DISTRICT HAZARD, RISK AND VULNERABILITY PROFILE Contents Acronyms ................................................................................................................... iii Acknowledgements .................................................................................................... iv EXECUTIVE SUMMARY .............................................................................................1 INTRODUCTION .........................................................................................................2 Objectives ...................................................................................................................2 Methodology ................................................................................................................2 Brief overview of the district ........................................................................................5 Background and history ...........................................................................................5 Geography ...............................................................................................................6 Climate .....................................................................................................................7 -

VSF – Spain) Community-Based Animal Health Workers (CAHW´S) in Ongino and Malera (Kumi District
Participatory Impact Assessment of the Veterinarios Sin Fronteras (VSF – Spain) Community-based Animal Health Workers (CAHW´s) in Ongino and Malera (Kumi District), Uganda Participatory Impact Assessment of the Veterinarios Sin Fronteras (VSF – Spain) Community Animal Health Workers (CAHW´s) in Ongino and Malera (Kumi District), Uganda Contents Acknowledgements 3 List of Abbreviations 4 1. Summary 5 2. Introduction 7 3. Methodology 11 4. Results 15 4.1. Mapping analysis 15 4.2. Matrix Scoring Analysis 17 4.2.1. Rank Analysis 17 4.2.2. Ongino Matrix Scoring 18 4.2.3. Malera Matrix Scoring 20 4.3. Proportional Pilling Analysis 22 4.3.1. Cows Proportional Pilling in Ongino. 24 4.3.2. Cows Proportional Pilling in Malera. 26 4.3.3. Goat Proportional Pilling in Ongino. 27 4.3.4. Goat Proportional Pilling in Malera. 28 5. Conclusions and recommendation 30 Annexes: 1. Visits Work Plan. 31 2. Matrix Scoring Analysis (Ongino and Malera together 32 3. List of diseases names in Ateso. 33 4. Mapping Questionnaire 34 5. Cattle Before – After Proportional Pilling questionnaire 36 6. Goat Before – After Proportional Pilling questionnaire 37 7. Matrix scoring questionnaire 38 8. Paravets Training Plan 39 2 Participatory Impact Assessment of the Veterinarios Sin Fronteras (VSF – Spain) Community Animal Health Workers (CAHW´s) in Ongino and Malera (Kumi District), Uganda Acknowledgements We would like to acknowledge the collaboration of Dr. Paul Ojuman (CoU-TEDDO) and Dr. Simon Arionga (DVO Office-Kumi) who’s wide experience in the veterinary field and in Kumi district have been invaluable for this study. -
Teso Investment Profile 2016
TESO INVESTMENT PROFILE 2016 THE REPUBLIC OF UGANDA Teso Investment Profile 2016 PAGE - 1/30 - Soroti Flying School Page - 2/30 - Teso Investment Profile 2016 Background Information Teso is bordered in the north and east by the semi-arid region of Karamoja, to the west by Lango and to the south by Bukedi. According to the 2014 National Population and Housing Census, 1.8 million people are living in Teso, 80% of whom are the Iteso who speak Ateso. But there is also a different, smaller tribal group living alongside and intermarrying with the Iteso called the Kumam who speak Kumam, a language related to Luo. The countryside of Teso is an undulating plateau, with large outcrops of rock, divided by shallow lakes and swamps. The region has bimodal rainfall regime, supporting two cropping seasons. The first and major cropping season normally starts in March and runs until mid to late June/July when the dry season sets in. The second and minor rains are often received between August and early December when second season harvests begin. For most of the location, there is no distinct lean period; however, districts close to Karamoja Region (Amuria and Katakwi) tend to experience nearly similar seasonal trends as their neighbors on the Karamoja side and are most impacted by any inordinate actions of their Karimojong neighbors. The vegetation in the sub-region can best be described as grassland savannah. The soils are mainly sandy loam with a variation from sandy to loamy soils depending on the terrain. The area is endowed with lakes, rivers and vast wetlands.